Iodine — Benefits Deep Dive
Iodine is arguably the most under-appreciated essential mineral in modern nutrition. The thyroid gland needs it to build T4 (four iodine atoms) and T3 (three iodine atoms) — the master regulators of every cell's metabolism — and the World Health Organization identifies iodine deficiency as the single most preventable cause of intellectual disability worldwide. Yet median U.S. urinary iodine fell by more than 50% between the 1970s and the early 2000s as commercial bakers swapped iodate dough conditioners for bromate, restaurants moved to non-iodized salt, and bromide / fluoride / perchlorate exposure surged. The four benefit pages below cover the biggest clinical effect domains where iodine status changes outcomes — thyroid hormone synthesis itself, fetal and childhood brain development, breast tissue health (fibrocystic disease and breast cancer epidemiology), and the basal-metabolic-rate / thermogenesis / weight-regulation axis that explains why iodine-deficient adults feel cold, tired, and stuck at a stubbornly high body weight.
Deep-Dive Articles
Thyroid Function
How T4 (four iodine atoms) and T3 (three iodine atoms) are built by thyroid peroxidase (TPO) on tyrosine residues in thyroglobulin, the sodium-iodide symporter (NIS) that concentrates iodide 20-40× against the plasma gradient, the Wolff-Chaikoff effect and its escape, iodine-deficiency goiter and hypothyroidism, the David Brownstein / Guy Abraham high-dose iodine protocols, Lugol's solution, iodide-vs-molecular-iodine pharmacology, and the history of U.S. salt iodization (Marine and Kimball, Akron 1917).
Brain Development
Why iodine deficiency is the world's leading preventable cause of intellectual disability, cretinism in its myxedematous and neurological forms, the maternal-fetal iodine transfer that drives fetal brain wiring in the first trimester, breast-milk iodine content as the sole iodine source for the nursing infant, the WHO and Iodine Global Network universal salt iodization (USI) program, and the 10-15 IQ-point deficit measured in mildly deficient populations (Qian 2005 China meta-analysis, ALSPAC UK cohort).
Breast Health
Breast tissue is the body's second most avid iodine-concentrating organ after the thyroid (via NIS and the pendrin transporter), Bernard Eskin's animal data linking iodine deficiency to fibrocystic dysplasia and mammary neoplasia, Ghent et al. (1993 Canadian Journal of Surgery) randomized trial of molecular iodine for fibrocystic breast disease, the Japan low-breast-cancer-rate hypothesis tied to dietary seaweed iodine, and the ongoing controversy over therapeutic dosing.
Metabolism & Energy
Thyroid hormone's control of basal metabolic rate (BMR), mitochondrial uncoupling proteins, brown-adipose-tissue thermogenesis and body temperature, the cold intolerance and fatigue that mark subclinical hypothyroidism, weight regulation when T3 falls below tissue-saturation, and the practical clinical pattern of iodine-deficient adults who diet and exercise without losing weight because their metabolic rate has been throttled at the thyroid level.
Table of Contents
- Deep-Dive Articles
- Why Iodine Produces Effects Across Many Systems
- Research Papers: Thyroid Function
- Research Papers: Brain Development & IQ
- Research Papers: Breast Health
- Research Papers: Metabolism & Energy
- Research Papers: Cross-Cutting (Mechanism, Status, Safety)
- External Authoritative Resources
- Connections
- Featured Videos
Why Iodine Produces Effects Across Many Systems
Most minerals act through a small number of enzyme cofactor roles (zinc in carbonic anhydrase, magnesium as an ATP counter-ion, selenium in glutathione peroxidase). Iodine is unusual because it has one dominant systemic mechanism — thyroid hormone synthesis — that secondarily controls the metabolic rate of every nucleated cell in the body, plus a set of distinct extra-thyroidal roles in tissues that express the sodium-iodide symporter (NIS) and concentrate iodide directly from the bloodstream.
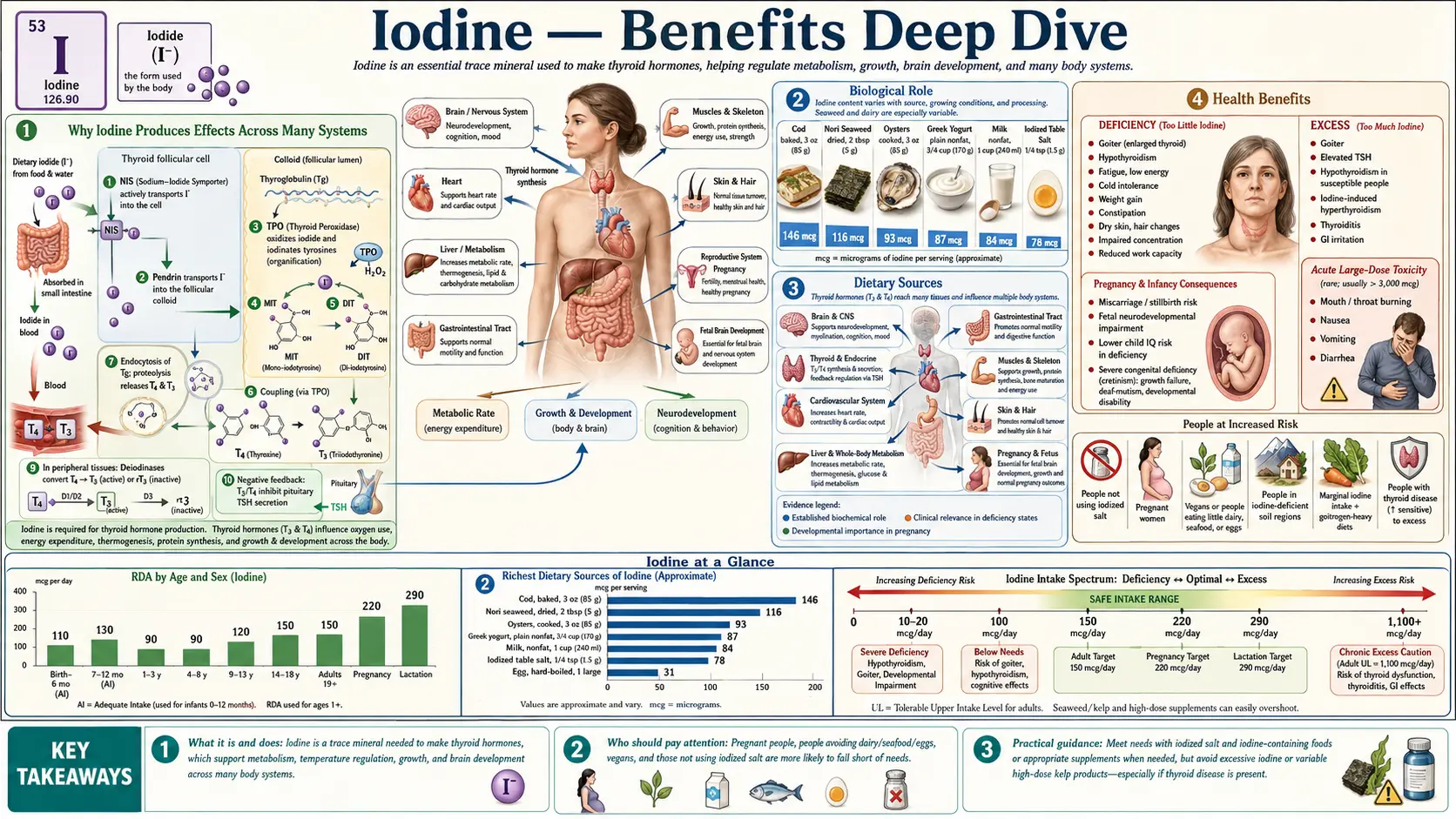
- Thyroid hormone synthesis (the dominant mechanism) — iodide is concentrated by the NIS into thyroid follicular cells, oxidized by thyroid peroxidase (TPO), and covalently bound to tyrosine residues on thyroglobulin to form mono- and di-iodotyrosines that couple into T4 (four iodine atoms) and T3 (three iodine atoms). The resulting thyroid hormones bind nuclear thyroid hormone receptors (TRα and TRβ) in essentially every tissue, driving the basal metabolic rate, mitochondrial biogenesis, body temperature, neuronal differentiation in the developing fetus, cardiac output, and hundreds of other genomic effects. This mechanism alone explains the thyroid effects, the brain-development effects, and the metabolism / energy / weight effects covered in the four deep-dive pages.
- Extra-thyroidal NIS distribution — the same sodium-iodide symporter is expressed in the breast (especially during pregnancy and lactation), the salivary glands, the gastric mucosa, the ovaries, the prostate, the choroid plexus of the brain, the ciliary body of the eye, and the lacrimal glands. These tissues concentrate iodide independent of the thyroid and use it for local antimicrobial and antioxidant functions. The most clinically important extra-thyroidal effect is in breast tissue, where molecular iodine (I₂) appears to drive apoptosis of pre-neoplastic ductal cells and reduce fibrocystic disease.
- Direct iodine chemistry as an antioxidant and antimicrobial — molecular iodine scavenges reactive oxygen species and lipid peroxides, generates antimicrobial hypoiodous acid (HOI) when oxidized by peroxidases in saliva, gastric juice, and breast milk, and forms iodolactones from arachidonic acid that activate PPAR-γ and promote apoptosis. These mechanisms add a layer of protection in mucosal tissues that is independent of thyroid hormone signaling.
The clinical complication is that the same nutrient that is required at 150 µg/day (the U.S. RDA, sufficient to prevent goiter) is given at 12.5-50 mg/day in the Brownstein / Abraham high-dose protocols (a 100-300× multiplier intended to saturate all extra-thyroidal tissues). The dose range across legitimate clinical use spans more than two orders of magnitude, and the optimal dose for any individual depends on baseline iodine status, selenium status (because thyroid peroxidase generates hydrogen peroxide that requires selenium-dependent glutathione peroxidase to neutralize), bromide / fluoride body burden, and the presence or absence of thyroid autoimmunity. The high end of the dose range remains controversial and should be approached gradually with appropriate cofactor support and laboratory monitoring.
Research Papers: Thyroid Function
- Marine D, Kimball OP (1917) Akron Ohio schoolgirls goiter prevention trial — the first U.S. iodine prophylaxis study — PubMed: Marine and Kimball 1917
- Sodium-iodide symporter (NIS) cloning and characterization (Dai, Levy, Carrasco 1996) — PubMed: NIS cloning
- Thyroid peroxidase (TPO) structure and iodination mechanism — PubMed: TPO mechanism
- Wolff-Chaikoff effect and escape (acute iodide block of T4 synthesis) — PubMed: Wolff-Chaikoff
- WHO global iodine status monitoring and urinary iodine medians — PubMed: WHO iodine status
- Goiter epidemiology and the Great Lakes goiter belt — PubMed: Goiter belt
- NHANES urinary iodine decline 1971-2002 — PubMed: NHANES decline
- Brownstein D, high-dose iodine clinical observations — PubMed: Brownstein iodine
- Abraham GE, iodine project and orthoiodosupplementation — PubMed: Abraham iodine project
- Selenium and thyroid peroxidase H2O2 / glutathione peroxidase coupling — PubMed: Selenium and TPO
Research Papers: Brain Development & IQ
- WHO iodine deficiency as leading preventable cause of intellectual disability — PubMed: WHO intellectual disability
- Qian M et al. (2005) meta-analysis of iodine deficiency and IQ in Chinese children — PubMed: Qian 2005 China meta-analysis
- Bath SC et al. ALSPAC cohort: mild maternal iodine deficiency and child IQ (Lancet 2013) — PubMed: ALSPAC iodine cohort
- Cretinism (myxedematous and neurological forms) — PubMed: Cretinism forms
- Maternal-fetal iodine transfer and fetal thyroid ontogeny — PubMed: Maternal-fetal transfer
- Breast milk iodine content and infant iodine sufficiency — PubMed: Breast milk iodine
- Universal salt iodization (USI) and the Iodine Global Network — PubMed: USI program
- Hetzel BS, iodine deficiency disorders (IDD) concept — PubMed: Hetzel IDD concept
- Pearce EN, iodine status of US pregnant women — PubMed: US pregnancy iodine
- Zimmermann MB, iodine and brain development review — PubMed: Zimmermann brain review
Research Papers: Breast Health
- Eskin BA, iodine deficiency and mammary dysplasia (animal model) — PubMed: Eskin mammary dysplasia
- Ghent WR et al. (1993) molecular iodine for fibrocystic breast disease — PubMed: Ghent 1993 FBD trial
- Kessler JH (2004) molecular iodine for cyclic mastalgia — PubMed: Kessler mastalgia
- Aceves C, Anguiano B, Delgado G — iodine and breast cancer mechanism (UNAM Mexico) — PubMed: Aceves iodine breast cancer
- Iodolactone formation from arachidonic acid and PPAR-gamma activation — PubMed: Iodolactones
- Japan dietary iodine intake and breast cancer epidemiology — PubMed: Japan breast cancer hypothesis
- Pendrin transporter and breast iodine uptake — PubMed: Pendrin breast
- NIS expression in breast cancer tissue — PubMed: NIS in breast cancer
- Molecular iodine vs iodide differential effects on breast tissue — PubMed: I2 vs I- in breast
- Iodine and estrogen receptor expression in breast cancer cells — PubMed: Iodine and ER
Research Papers: Metabolism & Energy
- Thyroid hormone control of basal metabolic rate — PubMed: T3 and BMR
- Mitochondrial uncoupling proteins (UCP1, UCP3) and thyroid hormone — PubMed: UCP and T3
- Brown adipose tissue thermogenesis regulation by T3 — PubMed: BAT and T3
- Subclinical hypothyroidism and weight gain — PubMed: Subclinical hypothyroidism weight
- Cold intolerance and hypothyroidism — PubMed: Cold intolerance
- Deiodinase enzymes (D1, D2, D3) and tissue T4-to-T3 conversion — PubMed: Deiodinases
- Thyroid hormone resistance and tissue T3 sensitivity — PubMed: T3 resistance
- Reverse T3 (rT3) and the low-T3 syndrome — PubMed: Reverse T3
- Metabolic rate and resting energy expenditure measurement — PubMed: REE and thyroid
- Iodine supplementation in subclinical hypothyroidism — PubMed: Iodine subclinical hypothyroidism
Research Papers: Cross-Cutting (Mechanism, Status, Safety)
- Bromide and iodine competition for NIS uptake — PubMed: Bromide vs iodide competition
- Fluoride and thyroid function — PubMed: Fluoride and thyroid
- Perchlorate as a NIS inhibitor — PubMed: Perchlorate inhibition
- Hashimoto's thyroiditis and iodine supplementation controversy — PubMed: Hashimoto's and iodine
- Urinary iodine concentration as the standard population biomarker — PubMed: Urinary iodine biomarker
- Iodine loading test (24-hour urinary iodine after 50 mg load) — PubMed: Iodine loading test
- Iodine and selenium interaction in thyroid health — PubMed: Iodine x selenium
- Lugol's solution composition and dosing — PubMed: Lugol's solution
- Linus Pauling Institute iodine micronutrient review — PubMed: LPI iodine review
- Iodine-induced hyperthyroidism (Jod-Basedow phenomenon) — PubMed: Jod-Basedow
External Authoritative Resources
- WHO — Iodine Deficiency — the global epidemiologic authority on iodine status, urinary iodine medians, and the Universal Salt Iodization (USI) program
- Iodine Global Network (IGN) — the NGO that monitors national iodine status and supports USI implementation in 80+ countries
- NIH Office of Dietary Supplements — Iodine Fact Sheet (Health Professionals)
- Linus Pauling Institute — Iodine Micronutrient Information Center
- American Thyroid Association — Iodine Deficiency
- PubMed — All research on iodine and thyroid
Connections
- Iodine (Main Page)
- Iodine for Thyroid Function
- Iodine for Brain Development
- Iodine for Breast Health
- Iodine for Metabolism & Energy
- All Minerals
- Selenium (TPO cofactor)
- Zinc
- Magnesium
- Tyrosine (thyroid hormone backbone)
- Hashimoto's Thyroiditis
- Thyroid Disorders
- Thyroid Cancer
- Infertility
- Brain Fog
- Fatigue
- Fluoride (halide competitor)