Iodine for Metabolism & Energy
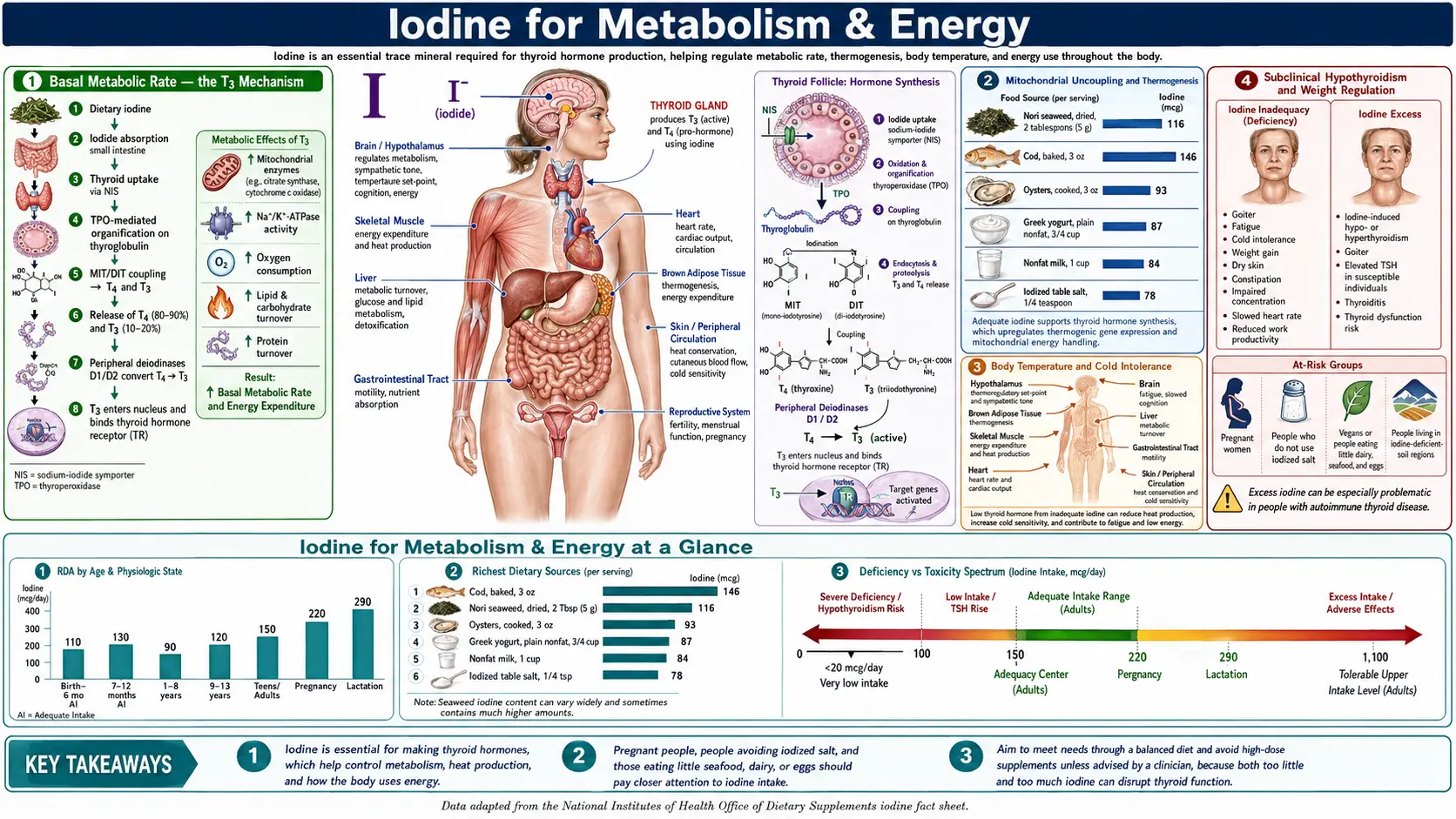
Thyroid hormones are the master regulators of basal metabolic rate (BMR) — the energy the body consumes at rest to maintain core temperature, perfuse organs, and run baseline cellular biochemistry. T3 (the active form, three iodine atoms) binds nuclear thyroid hormone receptors in essentially every cell and increases the expression of mitochondrial biogenesis genes, uncoupling proteins (UCP1 in brown fat, UCP3 in skeletal muscle), Na+/K+ ATPase, and the entire oxidative phosphorylation machinery. When T3 falls because iodine deficiency has throttled thyroid hormone synthesis at the source, BMR falls with it. The clinical signature is the patient who is cold all the time, exhausted by mid-afternoon, gaining weight despite reduced food intake, constipated, depressed, and unable to lose weight on a diet that would work for an iodine-sufficient peer. This page walks through the BMR mechanism, mitochondrial uncoupling and thermogenesis, the metabolic adaptations of subclinical hypothyroidism, the cold-intolerance and fatigue phenotype, and the practical clinical pattern of restoring iodine sufficiency as a precondition for successful weight management.
Table of Contents
- Basal Metabolic Rate — the T3 Mechanism
- Mitochondrial Uncoupling and Thermogenesis
- Body Temperature and Cold Intolerance
- Subclinical Hypothyroidism and Weight Regulation
- Fatigue as an Iodine-Deficiency Signal
- Deiodinases — the T4-to-T3 Conversion Bottleneck
- Iodine and Metabolic Syndrome
- The Clinical Pattern of Stuck-Weight Patients
- Iodine Repletion as Metabolic Rehabilitation
- Key Research Papers
- Connections
- Featured Videos
Basal Metabolic Rate — the T3 Mechanism
Basal metabolic rate (BMR) is the energy expenditure of a resting awake adult in a thermoneutral environment after a 12-hour fast — the energy the body consumes simply to stay alive without doing any external work. For a typical adult, BMR accounts for 60-75% of total daily energy expenditure. It is the dominant variable in determining how many calories the body burns per day, and small changes in BMR have large cumulative effects on body weight over weeks and months.
Thyroid hormone is the single most important hormonal regulator of BMR. The mechanism is direct genomic action: T3 (triiodothyronine) binds to nuclear thyroid hormone receptors (TRα1, TRβ1, TRβ2) which heterodimerize with retinoid X receptors (RXR) and bind to thyroid hormone response elements (TREs) in the promoter regions of hundreds of target genes. The downstream effects on metabolic rate are:
- Upregulation of Na+/K+ ATPase — the cellular ion pump that maintains sodium and potassium gradients across every cell membrane. The Na+/K+ ATPase is one of the largest ATP-consuming activities in the resting cell, and increasing its expression directly increases ATP demand and therefore BMR.
- Mitochondrial biogenesis — T3 upregulates PGC-1α (peroxisome proliferator-activated receptor gamma coactivator 1 alpha), the master regulator of mitochondrial biogenesis. More mitochondria per cell means more capacity for oxidative phosphorylation and more baseline oxygen consumption.
- Uncoupling protein expression — T3 upregulates UCP1 in brown adipose tissue and UCP3 in skeletal muscle. These proton-leak proteins dissipate the mitochondrial proton gradient as heat rather than ATP, increasing oxygen consumption and heat production without doing useful chemical work.
- Increased substrate cycling — T3 increases the rate of futile substrate cycles (such as the glucose-glucose 6-phosphate cycle and the triglyceride-fatty acid cycle) that consume ATP without net biosynthesis, contributing to BMR.
- Cardiac output — T3 increases heart rate and stroke volume, raising cardiac oxygen consumption and contributing to BMR.
The net effect of physiologic T3 on BMR is substantial. A patient with frank hypothyroidism may have a BMR 20-40% below normal. Even subclinical hypothyroidism (free T4 in the lower half of the reference range, TSH in the upper half) is associated with measurable BMR depression of 10-15% in metabolic chamber studies. For a 150 lb sedentary woman with a baseline BMR of 1,400 kcal/day, a 15% reduction translates to 210 kcal/day — equivalent to roughly 22 lbs of body weight per year if uncompensated by reduced caloric intake.
Mitochondrial Uncoupling and Thermogenesis
The uncoupling protein family (UCP1, UCP2, UCP3) sits in the inner mitochondrial membrane and allows protons to flow back across the membrane without passing through ATP synthase. The proton gradient established by the electron transport chain is therefore dissipated as heat rather than captured as ATP. This is a controlled "energy waste" mechanism whose biological purpose is heat production (thermogenesis) and metabolic flexibility.
- UCP1 — expressed almost exclusively in brown adipose tissue (BAT). UCP1 activation in response to cold or sympathetic nervous system signaling is the primary mechanism of mammalian non-shivering thermogenesis. BAT is abundant in infants (where it is essential for thermoregulation in the absence of effective shivering) and persists in smaller depots in adults (around the supraclavicular fat pads, paravertebral region, and perirenal fat). T3 is required for UCP1 expression and activity. Hypothyroid patients have measurably reduced BAT activity.
- UCP3 — expressed in skeletal muscle. UCP3 contributes to muscle thermogenesis and may protect mitochondria from reactive oxygen species generated during fatty acid oxidation. T3 upregulates UCP3 expression in skeletal muscle, contributing to the BMR effect of thyroid hormone.
- UCP2 — expressed ubiquitously, with functions in regulating insulin secretion (pancreatic beta cells), reactive oxygen species production, and immune cell function. Less prominently regulated by thyroid hormone than UCP1 and UCP3.
The thermogenic role of T3 has been a topic of considerable pharmaceutical interest. Synthetic thyromimetics (such as the TRβ-selective agonist eprotirome) were developed in the 2000s with the hope of stimulating BAT thermogenesis for weight loss without the cardiac and bone side effects of T3 itself. Clinical development largely failed because of off-target toxicity, and the most physiologic route to optimizing thermogenesis remains adequate iodine intake to support endogenous T3 synthesis combined with cold exposure to activate BAT.
Body Temperature and Cold Intolerance
Core body temperature is maintained by a balance between heat production (BMR plus thermogenesis plus shivering) and heat loss (radiation, conduction, convection, evaporation). Thyroid hormone is the principal hormonal regulator of baseline heat production, and hypothyroidism produces a reproducible drop in baseline body temperature of approximately 0.3-0.5°F (0.2-0.3°C) at the population level. The clinical manifestation is cold intolerance — the hypothyroid patient feels cold when others are comfortable, wears extra layers indoors, cannot tolerate air conditioning, and may have cold hands and feet that do not warm easily.
Broda Barnes, a mid-20th-century American physician, proposed the basal body temperature test as a screen for hypothyroidism: take axillary temperature first thing in the morning before getting out of bed, on three consecutive days (in menstruating women, days 2-4 of the cycle to avoid the luteal-phase temperature elevation). Persistently low readings (below 97.4°F) were interpreted as evidence of hypothyroidism even when TSH was within the reference range. The test fell out of mainstream use because of poor specificity (low body temperature has many causes), but it remains useful in integrative practice as one piece of evidence in evaluating a patient whose symptoms suggest hypothyroidism in the setting of normal TSH.
The cold-intolerance phenotype is one of the most reliable clinical pointers to suboptimal thyroid status and, by extension, to potential iodine insufficiency. A patient who is consistently cold when others are comfortable, who needs extra layers indoors, and who has chronically cold extremities, should have iodine status considered in addition to TSH and free T4.
Subclinical Hypothyroidism and Weight Regulation
Subclinical hypothyroidism is defined by an elevated TSH with a normal free T4. In population terms, approximately 4-10% of adults meet criteria, with prevalence rising in older age groups and approaching 20% of women over age 60. The "subclinical" label is misleading because the condition is associated with measurable metabolic abnormalities:
- Reduced basal metabolic rate (10-15% below euthyroid controls in calorimetry studies)
- Modest weight gain (typically 5-10 lbs over the years of subclinical state, mostly fluid retention but with some adipose accumulation)
- Elevated LDL cholesterol and total cholesterol
- Elevated triglycerides
- Elevated C-reactive protein (low-grade inflammation)
- Increased arterial stiffness and diastolic dysfunction
- Insulin resistance and impaired glucose tolerance
- Fatigue, cold intolerance, and depression at lower rates than overt hypothyroidism but at meaningfully elevated rates compared to controls
The relationship between subclinical hypothyroidism and weight gain is real but modest in magnitude. The literature suggests that the average TSH-elevation-related weight gain is 5-10 lbs over 5-10 years — not a fully sufficient explanation for severe obesity, but a meaningful contributor to the inability to lose weight on a diet that should be effective. For patients who plateau at a higher-than-expected weight despite genuine caloric restriction and exercise, evaluating thyroid status and underlying iodine sufficiency is a reasonable component of the workup.
For more on the metabolic-syndrome context, see our pages on Metabolic Syndrome and Obesity.
Fatigue as an Iodine-Deficiency Signal
Persistent fatigue is one of the most common presenting complaints in primary care and is one of the symptoms most consistently associated with hypothyroidism in patient self-report. The mechanism is straightforward: T3 governs mitochondrial biogenesis and oxidative phosphorylation capacity, and a body operating with depressed T3 has less mitochondrial energy production capacity per unit of cellular work. Patients describe:
- Difficulty waking in the morning despite adequate sleep
- Mid-afternoon energy crash, often around 2-4 PM
- Need for caffeine to function
- Post-exertional fatigue disproportionate to the work performed
- Reduced exercise tolerance and slower recovery from exercise
- "Brain fog" — slowed thinking, word-finding difficulty, reduced mental sharpness
- Persistent depression-like mood that does not respond well to conventional antidepressants
Fatigue has many causes, and iodine deficiency is one of them — not the only one and often not the most important one. In a workup for chronic fatigue, the differential diagnosis should include: anemia (iron, B12, folate), vitamin D deficiency, sleep apnea, depression, chronic fatigue syndrome (myalgic encephalomyelitis), adrenal insufficiency, chronic infections (Lyme, EBV), and thyroid dysfunction including iodine insufficiency. The thyroid workup should include TSH, free T4, free T3, TPO and thyroglobulin antibodies, and ideally urinary iodine measurement.
For more on fatigue evaluation, see our Fatigue page and Brain Fog page.
Deiodinases — the T4-to-T3 Conversion Bottleneck
The thyroid produces predominantly T4 (about 80% of output) with smaller amounts of T3. The metabolic effects discussed in this page require T3 specifically — T4 itself has weak intrinsic activity and functions essentially as a prohormone. The conversion of T4 to T3 is performed by the deiodinase enzyme family, all of which require selenium as a selenocysteine residue in the active site:
- Type 1 deiodinase (D1) — expressed primarily in the liver and kidneys, contributes to circulating T3 levels by deiodinating T4 in the blood-facing membrane. D1 is the principal target of propylthiouracil (PTU) in hyperthyroidism treatment.
- Type 2 deiodinase (D2) — expressed in the brain, pituitary, brown adipose tissue, and skeletal muscle. D2 produces local intracellular T3 from circulating T4 to drive local thyroid hormone effects. D2 is particularly important in brain and BAT, where it is the dominant source of intracellular T3.
- Type 3 deiodinase (D3) — an inactivating deiodinase that converts T4 to reverse T3 (rT3) and T3 to T2 (diiodothyronine). D3 is highly expressed in the placenta (limiting fetal T3 exposure to maternal T4), in the brain during development, and in many tumors.
Clinical implications of the deiodinase biology:
- Selenium deficiency reduces deiodinase function and can produce a clinical picture of "T3 hypothyroidism" with normal T4 and elevated rT3 — this is why selenium supplementation often produces symptomatic improvement in patients with normal TSH and free T4 but low free T3
- Acute and chronic illness, fasting, and severe caloric restriction shift deiodinase activity from T3-producing D2 to T3-inactivating D3, producing "low T3 syndrome" or "non-thyroidal illness syndrome" — an adaptive metabolic slowdown
- The reverse T3 (rT3) measurement is useful when iodine and thyroid status appear adequate but the patient remains symptomatic — high rT3 / free T3 ratios suggest a deiodinase-shift pattern that responds to selenium, stress reduction, and reversal of caloric restriction
- Some patients respond better to combined T4/T3 thyroid replacement (such as natural desiccated thyroid extracts) than to T4 alone, presumably because of impaired deiodinase function in their tissues
For more on the selenium-iodine partnership, see our Selenium page and the Thyroid Function deep-dive page in this Benefits set.
Iodine and Metabolic Syndrome
Metabolic syndrome is the clustered presentation of central obesity, hypertension, dyslipidemia (high triglycerides, low HDL), elevated fasting glucose, and a heightened cardiovascular risk profile. Approximately one-third of U.S. adults meet diagnostic criteria. The connection to iodine status is indirect but biologically real:
- Subclinical hypothyroidism is associated with insulin resistance and impaired glucose tolerance, contributing to the diabetes-and-prediabetes component of metabolic syndrome
- The dyslipidemia of subclinical hypothyroidism (elevated LDL, elevated triglycerides) overlaps with the dyslipidemia of metabolic syndrome
- The BMR depression of subclinical hypothyroidism contributes to the weight-gain dimension of metabolic syndrome
- The diastolic hypertension of subclinical hypothyroidism contributes to the hypertension dimension
- Low-grade systemic inflammation (elevated CRP) is shared by both conditions
The clinical question is not whether iodine deficiency causes metabolic syndrome, but whether iodine repletion in an iodine-insufficient patient with metabolic syndrome can move some of the metabolic-syndrome parameters toward normal. The pragmatic answer is yes, in patients who genuinely have iodine insufficiency and where the metabolic-syndrome parameters have a thyroid-mediated component. The repletion typically takes 3-6 months to manifest measurable changes in TSH, free T4, free T3, lipid panel, and weight.
The Clinical Pattern of Stuck-Weight Patients
One of the most common presentations in integrative endocrinology practice is the patient (typically a woman in her 30s-50s) who:
- Has gradually gained 15-30 lbs over 5-15 years despite no clear change in diet or activity
- Reports being unable to lose weight despite caloric restriction that should produce a deficit (counted calories, food diaries, MyFitnessPal logs to confirm)
- Has elevated thyroid antibodies (positive TPO or thyroglobulin) but TSH and free T4 within the laboratory reference range
- Is consistently cold, especially in the hands and feet
- Has dry skin, brittle hair, thinning eyebrows, occasional constipation
- Reports persistent low energy, mid-afternoon crash, and "brain fog"
- Has urinary iodine in the marginal range (below 100 µg/L in spot urine) or has never been tested
- Has been told by her primary care doctor that her thyroid labs are "normal" and that her symptoms are stress, perimenopause, or weight-related
This clinical picture often responds to a thoughtful workup that includes urinary iodine measurement, free T3, reverse T3, TPO and thyroglobulin antibodies, and selenium status. If iodine and selenium are both insufficient, structured repletion with selenium (200-400 mcg/day for 4-8 weeks first) followed by gradual iodine introduction (starting at a few hundred mcg/day and titrating to 3-6 mg/day over 2-3 months) often produces measurable improvement in fatigue, cold intolerance, and the ability to lose weight on a calorically-appropriate diet.
The repletion does not produce dramatic weight loss directly — it does not turn the body into a calorie-burning furnace. What it does is remove the metabolic-rate handbrake that has been preventing the patient's deficit-producing diet from actually producing weight loss. Patients who were stuck at a plateau despite 1,400 kcal/day intake often find that the same diet now produces gradual sustained weight loss as their BMR moves back into the appropriate range for their body composition.
Iodine Repletion as Metabolic Rehabilitation
A reasonable structured repletion protocol for the metabolic-syndrome / stuck-weight phenotype with documented iodine and selenium insufficiency:
- Baseline workup — TSH, free T4, free T3, reverse T3, TPO and thyroglobulin antibodies, urinary iodine (spot urine creatinine-adjusted, or 24-hour collection), serum selenium or red-cell selenium, ferritin, vitamin D, B12, fasting glucose, HbA1c, lipid panel
- Selenium first — 200-400 mcg/day selenomethionine (or one Brazil nut daily if dietary preference) for 4-8 weeks before introducing or escalating iodine. This is the cofactor prerequisite that prevents iodine-supplementation-related Hashimoto's exacerbation.
- Gradual iodine introduction — start at a few hundred mcg/day (typical prenatal vitamin level) for 2 weeks; advance to 1 mg/day for 2 weeks; advance to 3 mg/day for 2 weeks; advance to 6-12.5 mg/day if tolerated and indicated. The form should be combined iodide-plus-molecular-iodine (Lugol's drops or Iodoral tablets) for full extra-thyroidal tissue coverage.
- Cofactor support during iodine titration — continue selenium 200-400 mcg/day; unrefined sea salt to support bromide excretion (1/4 to 1/2 teaspoon daily); magnesium 400 mg/day; vitamin C 1,000-3,000 mg/day; B-complex with riboflavin for FAD-dependent enzymes
- Monitor for bromide detox symptoms — skin rash, metallic taste, headache, sinus congestion, irritability, gastrointestinal disturbance. These typically resolve in days to weeks. Slow the titration if intolerable; adequate salt and water support helps.
- Repeat labs at 3 and 6 months — TSH, free T4, free T3, TPO antibodies, thyroglobulin antibodies, urinary iodine. Adjust dose based on clinical response and lab trajectory. The goal is iodine sufficiency (urinary iodine 150-300 µg/L) and stable or falling thyroid antibody titers.
- Address other metabolic-syndrome dimensions — iodine repletion alone will not fix metabolic syndrome. It removes a metabolic handbrake but the underlying insulin resistance, dietary patterns, sleep quality, stress load, and physical activity all need attention.
Patients who undertake this protocol with appropriate clinical guidance and lab monitoring typically report measurable improvement in fatigue, cold intolerance, mental clarity, and weight trajectory within 3-6 months. The improvement is real but is rarely dramatic in the first month — the metabolic adaptations of long-standing iodine and selenium insufficiency take months to reverse.
Key Research Papers
- Silva JE (1995). Thyroid hormone control of thermogenesis and energy balance. Thyroid. — PubMed
- Bianco AC, Salvatore D, Gereben B, Berry MJ, Larsen PR (2002). Biochemistry, cellular and molecular biology, and physiological roles of the iodothyronine selenodeiodinases. Endocr Rev. — PubMed
- Krotkiewski M (2002). Thyroid hormones in the pathogenesis and treatment of obesity. Eur J Pharmacol. — PubMed
- Biondi B (2010). Thyroid and obesity: an intriguing relationship. JCEM. — PubMed
- Kim B (2008). Thyroid hormone as a determinant of energy expenditure and the basal metabolic rate. Thyroid. — PubMed
- Lowell BB, Spiegelman BM (2000). Towards a molecular understanding of adaptive thermogenesis. Nature. — PubMed
- Cypess AM et al. (2009). Identification and importance of brown adipose tissue in adult humans. NEJM. — PubMed
- Mullur R, Liu YY, Brent GA (2014). Thyroid hormone regulation of metabolism. Physiol Rev. — PubMed
- Razvi S et al. (2018). Thyroid hormones and cardiovascular function and diseases. JACC. — PubMed
- Pearce EN (2012). Thyroid hormone and obesity. Curr Opin Endocrinol Diabetes Obes. — PubMed
- Tiller J et al. (2015). Effect of levothyroxine on body weight in patients with subclinical hypothyroidism. Endocr Pract. — PubMed
- Mehran L et al. (2019). Thyroid disease and the metabolic syndrome. Curr Opin Endocrinol Diabetes Obes. — PubMed
PubMed Topic Searches
- PubMed: BMR and T3
- PubMed: UCP1 thermogenesis
- PubMed: Subclinical hypothyroidism and weight
- PubMed: Deiodinase selenium conversion
- PubMed: Cold intolerance and hypothyroidism
Connections
- Iodine Benefits Hub
- Iodine Overview
- Iodine for Thyroid Function
- Iodine for Brain Development
- Iodine for Breast Health
- Selenium (deiodinase cofactor)
- Metabolic Syndrome
- Obesity
- Hashimoto's Thyroiditis
- Thyroid Disorders
- Fatigue
- Brain Fog
- Depression
- Tyrosine
- All Minerals