Haptoglobin Test
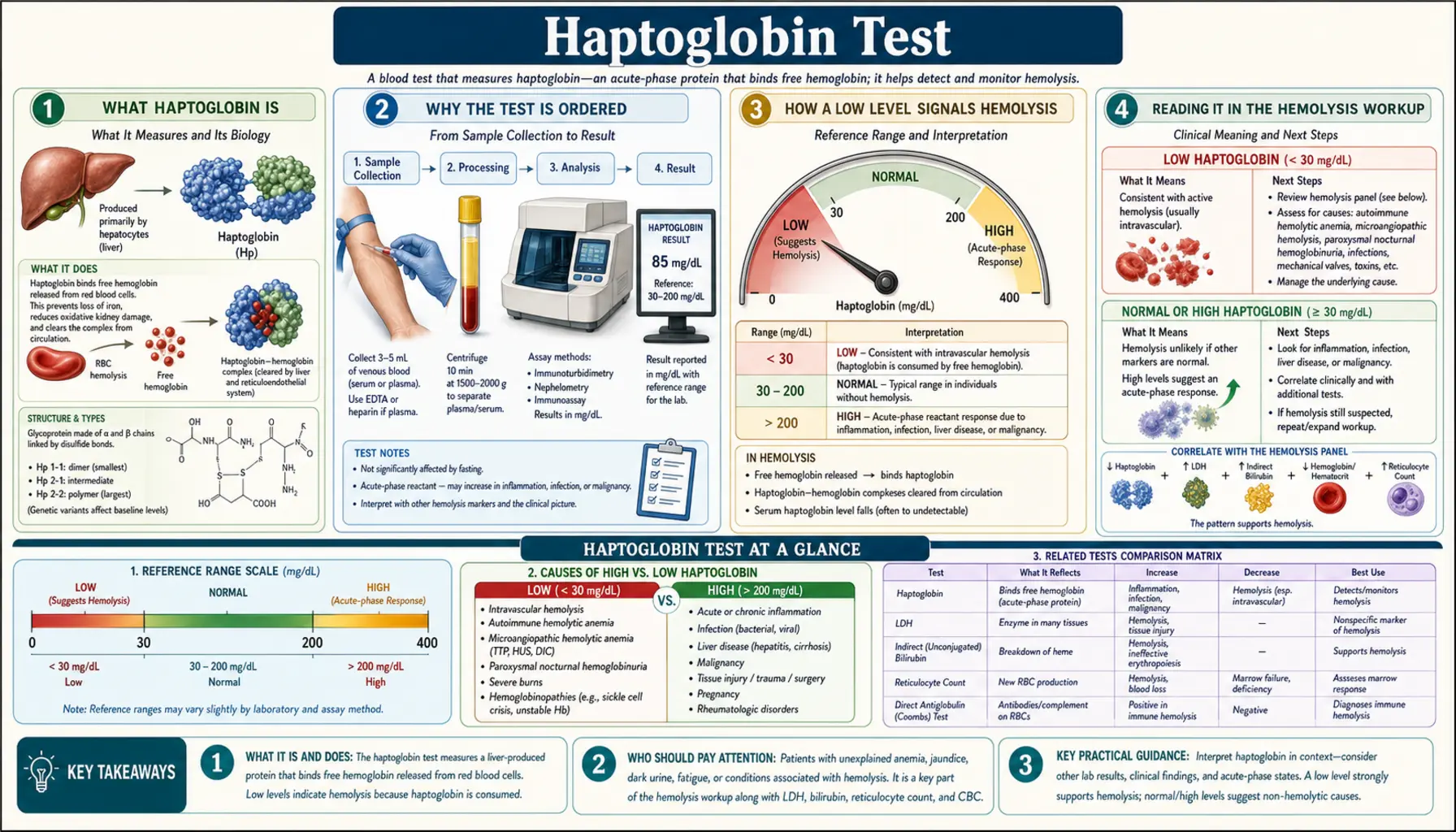
Haptoglobin is a protein made by your liver whose everyday job is to be a cleanup crew for hemoglobin — the oxygen-carrying pigment packed inside red blood cells. Red cells are supposed to keep their hemoglobin safely tucked away. When they rupture and spill it loose into the bloodstream, haptoglobin grabs the free hemoglobin and hauls it off for safe disposal and recycling. That cleanup role is exactly why doctors measure it. When red cells are being destroyed faster than normal — a process called hemolysis — haptoglobin gets used up faster than the liver can replace it, and its blood level drops, often to nearly nothing. A low haptoglobin is therefore one of the most useful early clues that a hemolytic process is underway. This page explains what the test measures, how doctors read it alongside other results, and the important catches — including the fact that inflammation can quietly hide a real problem.
Table of Contents
- What Haptoglobin Is
- Why the Test Is Ordered
- How a Low Level Signals Hemolysis
- Reading It in the Hemolysis Workup
- The Big Catch: An Acute-Phase Reactant
- Congenital Anhaptoglobinemia & Gene Variants
- Reference Ranges & What Your Number Means
- How the Test Is Done & How to Prepare
- Research Papers
- Connections
- Featured Videos
What Haptoglobin Is
Haptoglobin is a glycoprotein — a protein with sugar chains attached — that your liver builds and releases into the blood, where it circulates continuously. Chemists classify it as an alpha-2 globulin, one of the plasma proteins you would see on a protein electrophoresis test. Its defining talent is that it binds to free hemoglobin with extraordinary strength, forming a tight haptoglobin–hemoglobin complex that almost never lets go.
Why does the body devote a dedicated protein to mopping up loose hemoglobin? Because free hemoglobin outside a red cell is genuinely dangerous. Inside a red blood cell, hemoglobin is contained and controlled. Once it leaks into plasma it causes trouble in several ways:
- It mops up nitric oxide. Free hemoglobin greedily scavenges nitric oxide, the molecule blood vessels use to relax and stay open. Losing it can trigger blood-vessel constriction, high blood pressure in the lungs, and cramping.
- Its iron drives oxidative damage. The heme and iron at the center of hemoglobin are chemically reactive and can generate tissue-damaging free radicals once they are no longer safely packaged.
- It injures the kidneys. Free hemoglobin is small enough to be filtered by the kidneys, where it can clog and damage the delicate filtering tubules — the reason severe intravascular hemolysis can turn the urine dark and harm kidney function.
Haptoglobin defuses all of this. By clamping onto free hemoglobin the instant it appears, haptoglobin keeps it out of the kidneys, blunts the nitric-oxide problem, and flags the complex for orderly removal so its iron can be recycled rather than lost or turned loose. It works alongside a partner protein called hemopexin, which scavenges free heme after haptoglobin is overwhelmed. Together they form the body's front-line defense against the hemoglobin that spills whenever red cells break.
Why the Test Is Ordered
The haptoglobin blood test has one dominant purpose: to help detect and confirm hemolysis — the accelerated destruction of red blood cells. It is rarely ordered on its own. Instead, a doctor reaches for it when the clinical picture suggests red cells may be breaking down faster than the body is replacing them.
Common reasons to order a haptoglobin level include:
- Unexplained anemia. When someone is anemic and the cause is not obvious, a low haptoglobin helps decide whether the anemia comes from destruction of red cells (hemolysis) rather than blood loss or a failure of the marrow to make enough.
- Signs that point to red-cell breakdown. Fatigue and pallor, yellowing of the skin or eyes (jaundice), dark or tea-colored urine, an enlarged spleen, or shortness of breath can all raise suspicion of hemolysis.
- Monitoring a known hemolytic condition. In diseases such as autoimmune hemolytic anemia, sickle cell disease, or the inherited red-cell disorders, haptoglobin can be tracked over time to gauge how active the hemolysis is.
- Suspected transfusion reaction. If a patient develops fever, back pain, or dark urine during or shortly after a blood transfusion, a falling haptoglobin is one signal that the transfused cells are being destroyed.
- Mechanical red-cell damage. Artificial heart valves, circulatory support devices, and certain small-vessel diseases can physically shear red cells apart, and haptoglobin helps detect that.
Because haptoglobin answers a specific question — "are red cells being destroyed?" — it almost always travels in a group of tests ordered together, described in the workup section below.
How a Low Level Signals Hemolysis
The logic behind the test is elegant and worth understanding, because it explains both the test's power and its blind spots.
Picture a steady population of haptoglobin molecules patrolling the plasma. Normally there is very little free hemoglobin around, so most haptoglobin sits idle, and the level stays in its usual range. Now suppose red cells start rupturing. Each burst cell releases hemoglobin into the plasma. Haptoglobin immediately binds it, one molecule of haptoglobin locking onto the hemoglobin. The resulting complex is then recognized by a receptor called CD163 on the surface of macrophages — the body's large scavenger cells — which swallow the whole complex, break it down, and salvage the iron.
Here is the crucial detail: haptoglobin is consumed in the process. It is not released and reused; it is degraded along with the hemoglobin it captured. So during active hemolysis, haptoglobin is being spent far faster than the liver can manufacture replacements. The plasma level falls — often all the way to undetectable. That drop is the signal the test picks up. A low or absent haptoglobin says, in effect, "something has been dumping hemoglobin into the blood and using up the cleanup supply."
One important nuance separates the two main kinds of hemolysis:
- Intravascular hemolysis — red cells rupture inside the blood vessels, releasing hemoglobin directly into the plasma. Examples include mechanical heart-valve damage, severe transfusion reactions, some small-vessel clotting disorders, and paroxysmal nocturnal hemoglobinuria. Because hemoglobin floods the plasma directly, haptoglobin is consumed heavily and often becomes undetectable. This is where the test shines.
- Extravascular hemolysis — red cells are engulfed and destroyed by macrophages in the spleen and liver, so relatively little free hemoglobin ever reaches the open plasma. Examples include warm autoimmune hemolytic anemia and hereditary spherocytosis. Here haptoglobin may be only mildly reduced or even normal, especially if the hemolysis is slow.
So a strikingly low haptoglobin leans toward intravascular destruction, while a normal haptoglobin does not fully rule out a gentler, extravascular process. This is one reason haptoglobin is never read in isolation.
Reading It in the Hemolysis Workup
No single blood test proves hemolysis by itself. Doctors diagnose it by recognizing a pattern across several results that all point the same direction. Haptoglobin is one member of a classic quartet of hemolysis markers:
- Haptoglobin — LOW. Consumed while clearing free hemoglobin, as described above.
- LDH (lactate dehydrogenase) — HIGH. This enzyme is abundant inside red cells; when the cells rupture, it spills into the blood and the level rises. (LDH is not specific to red cells, so it is read as one clue among several.)
- Indirect (unconjugated) bilirubin — HIGH. Bilirubin is the yellow pigment made when heme from hemoglobin is broken down. A surge of red-cell destruction produces a surge of bilirubin, which is why hemolysis can cause jaundice.
- Reticulocyte count — HIGH. Reticulocytes are young, freshly released red cells. When the marrow senses that red cells are being lost, it responds by pumping out extra young cells, so their count climbs. A high reticulocyte count shows the marrow is trying to compensate.
Put together, the signature of active hemolysis is low haptoglobin + high LDH + high indirect bilirubin + high reticulocytes. When all four line up, hemolysis becomes very likely. When they clearly do not, it becomes unlikely.
A landmark 1980 study helped quantify just how useful haptoglobin is within this pattern. It found that a low serum haptoglobin was a strong and specific indicator of hemolytic disease, and that combining haptoglobin with LDH sharpened the assessment further — a very low haptoglobin together with a raised LDH strongly favored hemolysis, whereas normal values for both made hemolysis quite unlikely (see Research Papers). That combination remains a practical bedside rule of thumb today.
Additional tests round out the workup and help pin down the cause once hemolysis is confirmed:
- Peripheral blood smear — a technologist examines the red cells under a microscope for tell-tale shapes: fragmented cells (schistocytes) suggest mechanical or small-vessel destruction, while sphere-shaped cells (spherocytes) suggest an autoimmune or membrane cause.
- Direct antiglobulin test (DAT, or Coombs test) — detects antibodies stuck to the red cells, distinguishing immune-mediated hemolysis from other kinds.
- Urine hemoglobin and hemosiderin — signs that free hemoglobin has spilled into the urine, pointing to intravascular hemolysis.
Haptoglobin's job in all of this is to answer the first question — is hemolysis happening at all? — quickly and inexpensively, so the rest of the workup can focus on why.
The Big Catch: An Acute-Phase Reactant
This is the single most important thing to understand about interpreting a haptoglobin result, and it is easy to miss. Haptoglobin has a second identity: it is a positive acute-phase reactant. That means the liver deliberately ramps up its production during inflammation, infection, tissue injury, surgery, and some cancers — a response driven largely by inflammatory signaling molecules such as interleukin-6. In those settings, haptoglobin goes up.
Now combine the two roles and you can see the trap. Suppose a person has mild hemolysis (which is pulling haptoglobin down) at the same time as an infection or inflammatory condition (which is pushing haptoglobin up). The two effects can cancel each other out, leaving a haptoglobin level that reads deceptively normal — even though real red-cell destruction is occurring underneath. Inflammation can, in effect, mask hemolysis and produce a false-negative result. Studies that examined the clinical factors influencing haptoglobin confirmed exactly this kind of distortion (see Research Papers).
Because of this, a normal haptoglobin should never be used to confidently exclude hemolysis in a patient who is also sick or inflamed. Good clinicians interpret haptoglobin alongside markers of inflammation — such as C-reactive protein or the erythrocyte sedimentation rate — and lean on the rest of the hemolysis panel (LDH, bilirubin, reticulocytes, smear) rather than trusting haptoglobin alone.
The reverse caution matters too: a low haptoglobin is not perfectly specific for hemolysis either. Other conditions can lower it, including:
- Advanced liver disease. Since the liver manufactures haptoglobin, severe liver damage reduces production and the level drops — without any hemolysis.
- Congenital absence. Some people are simply born with little or no haptoglobin (see the next section).
- Newborn physiology. Infants normally have very low levels in the first months of life.
- Dilution. Large-volume fluid resuscitation or massive transfusion can dilute the measured level.
None of this makes haptoglobin a poor test. It makes it a test that must be read in context — which is true of nearly every lab value, and especially true of this one.
Congenital Anhaptoglobinemia & Gene Variants
Not everyone who has a low or undetectable haptoglobin is hemolyzing. Some people are born that way. Congenital anhaptoglobinemia is the complete, inherited absence of haptoglobin, and hypohaptoglobinemia is a persistently very low inherited level. Neither reflects red-cell destruction — the person simply does not make the protein — yet a routine test will show a strikingly low result that can be mistaken for hemolysis if the possibility is not considered.
The gene that codes for haptoglobin (called HP) comes in two common versions, historically labeled Hp1 and Hp2. Because everyone inherits one copy from each parent, three main genetic types result: Hp1-1, Hp2-1, and Hp2-2. These types differ in the size and shape of the haptoglobin molecule they build, and in subtle ways in how efficiently that molecule binds and clears hemoglobin. Researchers have studied whether particular types are linked to differences in inflammation, infection, and cardiovascular or kidney disease, though the practical clinical use of typing is still limited. For the purposes of the haptoglobin blood test, the key takeaway is simpler: genetic variation means baseline haptoglobin levels differ from person to person.
Congenital anhaptoglobinemia is more common in people of African and Southeast Asian ancestry, and it carries two practical implications:
- A false signal for hemolysis. A persistently undetectable haptoglobin, in someone with an otherwise normal reticulocyte count, LDH, and bilirubin, may reflect congenital absence rather than active red-cell destruction. Recognizing this avoids an unnecessary hemolysis workup.
- A rare transfusion risk. People who make no haptoglobin at all can, uncommonly, form antibodies against the haptoglobin in donated blood, which in rare cases has been linked to severe allergic (anaphylactic) transfusion reactions. This is unusual but is one reason the finding is worth noting in a person's record.
The bottom line is that a very low haptoglobin always deserves a moment's thought: is this hemolysis, liver disease, inflammation masking, or simply the level this person was born with? The rest of the panel usually settles the question.
Reference Ranges & What Your Number Means
Haptoglobin is reported as a concentration in the blood, most often in milligrams per deciliter (mg/dL) in the United States or grams per liter (g/L) elsewhere. As a rough conversion, 100 mg/dL equals 1 g/L. Reference ranges differ from one laboratory and method to another, so the numbers below are typical guides, not universal cutoffs. Always interpret your result against the reference range printed on your own report, and in the context of the rest of your bloodwork.
A commonly cited adult reference range is roughly 30 to 200 mg/dL (about 0.3 to 2.0 g/L), though some laboratories report slightly different lower and upper bounds. Within that framework:
- Low or undetectable haptoglobin (well below the reference range, often near zero) is the finding that matters most for this test. In the right clinical setting it points to hemolysis — especially intravascular hemolysis, where the level is frequently unmeasurable. But remember the alternatives: advanced liver disease (reduced production), congenital anhaptoglobinemia, the newborn period, or dilution after large fluid or blood volumes can all lower it without hemolysis.
- Normal haptoglobin makes brisk intravascular hemolysis unlikely — but does not exclude slow extravascular hemolysis, and, critically, can be a falsely reassuring value when inflammation is simultaneously raising the level (the acute-phase catch above).
- High haptoglobin (above the reference range) usually reflects the acute-phase response — inflammation, infection, tissue injury, recent surgery, or some cancers. Doctors rarely order the test to look for a high value on its own, but a high result is a useful reminder that any coexisting mild hemolysis may be hidden.
Two special situations are worth calling out. First, newborns and young infants normally have very low or absent haptoglobin because the liver's production is still immature; a low level in the first few months of life is expected and does not, by itself, indicate a problem, which limits the test's usefulness in early infancy. Second, because haptoglobin can be pushed in opposite directions by hemolysis and inflammation at once, a single number is far less informative than the trend over time and the company it keeps — LDH, bilirubin, reticulocytes, and a look at the blood smear.
How the Test Is Done & How to Prepare
The haptoglobin test is straightforward. A technician draws a small sample of blood from a vein in your arm, and the sample is sent to the laboratory, where the haptoglobin concentration is measured — commonly by an immunoassay that detects the protein directly. There is nothing unusual or uncomfortable about the draw itself beyond the brief pinch of any blood test.
In most cases no special preparation is needed — you generally do not have to fast or change your routine. Still, a few things are worth mentioning to whoever orders or draws the test, because they can affect interpretation:
- Recent blood transfusions — they can shift haptoglobin levels and complicate the reading.
- Known liver disease or a known hemolytic condition — both change the baseline you are being measured against.
- Current infection, inflammation, or recent surgery — these raise haptoglobin as an acute-phase reactant and may mask hemolysis.
- Medications and supplements — some drugs can provoke hemolysis or influence the result; share your full list.
- Pregnancy or estrogen-containing medication — these can modestly affect protein levels.
Because haptoglobin answers only one part of the question, it is almost always ordered together with a panel of related tests — a complete blood count, LDH, bilirubin, a reticulocyte count, a peripheral smear, and often a direct antiglobulin (Coombs) test. Results are usually available within a day. If your haptoglobin comes back low, do not try to interpret it alone: the meaning depends entirely on the other results and on your clinical situation, which is a conversation to have with the clinician who ordered it.
Research Papers
- Shih AW, McFarlane A, Verhovsek M. Haptoglobin testing in hemolysis: measurement and interpretation. American Journal of Hematology. 2014;89(4):443–447. doi:10.1002/ajh.23623 — A practical review of how haptoglobin is measured and the pitfalls of reading it as a hemolysis marker, including the acute-phase confounder.
- Marchand A, Galen RS, Van Lente F. The predictive value of serum haptoglobin in hemolytic disease. JAMA. 1980;243(19):1909–1911. doi:10.1001/jama.1980.03300450023014 — The classic study establishing that a low haptoglobin is a strong, specific indicator of hemolysis, especially when paired with a raised LDH.
- Barcellini W, Fattizzo B. Clinical applications of hemolytic markers in the differential diagnosis and management of hemolytic anemia. Disease Markers. 2015;2015:635670. doi:10.1155/2015/635670 — Reviews how haptoglobin, LDH, bilirubin, and reticulocytes are combined to diagnose and follow hemolytic anemia.
- Körmöczi GF, Säemann MD, Buchta C, et al. Influence of clinical factors on the haemolysis marker haptoglobin. European Journal of Clinical Investigation. 2006;36(3):202–209. doi:10.1111/j.1365-2362.2006.01617.x — Shows how inflammation and other clinical factors distort haptoglobin, limiting its reliability when read in isolation.
- Gabay C, Kushner I. Acute-phase proteins and other systemic responses to inflammation. New England Journal of Medicine. 1999;340(6):448–454. doi:10.1056/NEJM199902113400607 — The standard reference explaining why haptoglobin rises with inflammation as a positive acute-phase protein — the mechanism behind the masking effect.
- Schaer DJ, Vinchi F, Ingoglia G, Tolosano E, Buehler PW. Haptoglobin, hemopexin, and related defense pathways—basic science, clinical perspectives, and drug development. Frontiers in Physiology. 2014;5:415. doi:10.3389/fphys.2014.00415 — An overview of how haptoglobin and its partner hemopexin protect the body from free hemoglobin and heme.
- Andersen CBF, Torvund-Jensen M, Nielsen MJ, et al. Structure of the haptoglobin–haemoglobin complex. Nature. 2012;489(7416):456–459. doi:10.1038/nature11369 — Solved the molecular structure that shows how haptoglobin clamps onto hemoglobin so tightly.
- Nielsen MJ, Moestrup SK. Receptor targeting of hemoglobin mediated by the haptoglobins: roles beyond heme scavenging. Blood. 2009;114(4):764–771. doi:10.1182/blood-2009-01-198309 — Describes how the CD163 macrophage receptor clears the haptoglobin–hemoglobin complex — the step that consumes haptoglobin during hemolysis.
- Langlois MR, Delanghe JR. Biological and clinical significance of haptoglobin polymorphism in humans. Clinical Chemistry. 1996;42(10):1589–1600. doi:10.1093/clinchem/42.10.1589 — The definitive review of the HP gene variants (Hp1-1, Hp2-1, Hp2-2) and congenital anhaptoglobinemia.
- Delanghe JR, Langlois MR. Hemopexin: a review of biological aspects and the role in laboratory medicine. Clinica Chimica Acta. 2001;312(1-2):13–23. doi:10.1016/s0009-8981(01)00586-1 — Covers hemopexin, haptoglobin's backup heme scavenger, which also falls in severe intravascular hemolysis.
Connections
- Reticulocyte Count
- Complete Blood Count
- LDH (Lactate Dehydrogenase)
- Liver Function Tests
- Iron Panel
- Ferritin
- hs-CRP (Inflammation)
- Anemia
- G6PD Deficiency
- Hereditary Spherocytosis
- Cold Agglutinin Disease
- Sickle Cell Disease
- Paroxysmal Nocturnal Hemoglobinuria
- All Lab Tests