Cardiac Troponin Test (Troponin I & T)
Cardiac troponin (cTnI and cTnT) is the gold-standard biomarker for diagnosing acute myocardial infarction. Released from cardiomyocytes when the cell membrane is disrupted, it combines high sensitivity — it detects even minor myocardial injury — with high cardiac specificity, because the cardiac isoforms are structurally distinct from skeletal muscle troponin. The arrival of high-sensitivity troponin (hs-cTn) assays transformed the emergency evaluation of chest pain, making 0h/1h and 0h/2h rapid rule-in / rule-out algorithms possible where earlier assays needed six hours or more.
Interactive Visualization The Heart & Circulation — watch a blood cell make the loop Trace a blood cell through all four chambers and both circuits, with a live ECG, chamber pressures, and an exercise mode. Launch →Table of Contents
- What the Cardiac Troponin Test Measures
- Biochemistry of the Troponin Complex
- Why Troponin Testing Is Ordered
- How the Test Is Performed
- Troponin I vs. Troponin T: Differences
- Reference Ranges and Result Interpretation
- The Troponin Rise-and-Fall Pattern
- Rapid Rule-In and Rule-Out Algorithms
- The HEART Score
- The Five Types of Myocardial Infarction
- Conditions That Elevate Troponin
- Non-Coronary Causes in Depth
- High-Sensitivity Troponin (hs-cTn)
- How to Reduce Cardiac Risk
- Limitations of Troponin Testing
- Key Research Papers
- Connections
- Featured Videos
What the Cardiac Troponin Test Measures
Cardiac troponin is a protein complex found exclusively in heart muscle cells (cardiomyocytes). It plays a central role in regulating the contraction of the heart by controlling the interaction between actin and myosin, the two proteins that generate the mechanical force of heartbeat. The troponin complex has three subunits: troponin C (which binds calcium), troponin I (which inhibits contraction in the resting state), and troponin T (which anchors the complex to tropomyosin on the actin filament).
In a healthy heart, troponin remains inside cardiomyocytes. When heart muscle cells are damaged or die -- as occurs during a myocardial infarction, myocarditis, or significant cardiac stress -- the cell membranes break down and troponin leaks into the bloodstream. Because cardiac troponin I (cTnI) and cardiac troponin T (cTnT) are structurally distinct from their skeletal muscle counterparts, laboratory assays can detect them with high cardiac specificity. Even tiny amounts of myocardial injury produce measurable troponin elevation well before symptoms escalate or electrocardiogram changes appear.
Troponin testing has become the gold-standard biomarker for diagnosing acute myocardial infarction (heart attack) and for risk-stratifying patients presenting with chest pain. The advent of high-sensitivity troponin (hs-cTn) assays in the 2010s further transformed cardiac emergency medicine by detecting injury at concentrations 10 to 100 times lower than conventional assays.
How Troponin Became the Standard
Troponin entered routine clinical use as a cardiac biomarker in the 1990s and rapidly displaced CK-MB (the MB isoform of creatine kinase), which had been the previous standard but was also present in skeletal muscle and therefore far less cardiac-specific. The 2000 ESC/ACC consensus document redefined myocardial infarction around the new marker: any troponin elevation above the 99th percentile of a healthy reference population, accompanied by a rise and/or fall pattern and evidence of ischemia. That document became the first "Universal Definition of Myocardial Infarction," and it has been revised three times since — in 2007, 2012, and 2018.
The two cardiac-specific isoforms measured in clinical practice are distinguished from their skeletal-muscle counterparts by structural features that the assay antibodies target directly:
- Cardiac troponin I (cTnI): the inhibitory subunit, roughly 31 kDa, carrying a unique 31-amino-acid N-terminal extension found in no skeletal muscle isoform at any stage of life.
- Cardiac troponin T (cTnT): the tropomyosin-binding subunit, roughly 36 kDa, with a cardiac-specific epitope in its N-terminal region. The Roche Elecsys hs-cTnT assay built on that epitope is the most extensively studied troponin platform in the world.
Both are measured with highly specific monoclonal antibodies that do not cross-react with skeletal muscle isoforms under normal conditions — which makes the test cardiac-specific, not merely cardiac-sensitive. It is worth being precise about what that specificity does and does not buy: troponin identifies myocardial cell injury or death, but it does not identify the cause of that injury. Coronary atherosclerosis, cardiomyopathy, myocarditis, pulmonary embolism, and sepsis all produce the same signal. Sorting out which one is in front of you requires clinical history, the ECG, echocardiography, and where appropriate coronary angiography.
Biochemistry of the Troponin Complex
The troponin complex is a trimeric regulatory protein embedded in the thin filament of striated muscle, sitting at the core of the calcium-regulated actin-myosin contraction cycle. Each of the three subunits has a distinct structural and functional role:
- Troponin T (TnT) — the tropomyosin-binding subunit. It anchors the entire complex to tropomyosin along the thin filament. Its elongated N-terminal tail extends along tropomyosin, while its globular C-terminal domain interacts with TnI and TnC.
- Troponin I (TnI) — the inhibitory subunit. At low intracellular calcium, TnI's inhibitory region binds actin, holding tropomyosin over the myosin-binding sites and preventing contraction. The cardiac-specific N-terminal extension (residues 1–31) is phosphorylated by protein kinase A in response to beta-adrenergic stimulation, which modulates the calcium sensitivity of contraction — part of how adrenaline makes the heart contract harder and relax faster.
- Troponin C (TnC) — the calcium-sensing subunit. It contains four EF-hand calcium-binding motifs. Sites III and IV at the C-terminal end are high-affinity structural sites that are permanently occupied; site II at the N-terminal end is the low-affinity regulatory site that binds calcium during depolarization and triggers the conformational cascade.
The Contraction Cycle
When intracellular calcium rises during an action potential, calcium binds TnC's regulatory site II. The resulting conformational change causes TnC to grab TnI's inhibitory domain, releasing TnI from actin. Tropomyosin then shifts and exposes the myosin-binding sites on actin, permitting cross-bridge cycling and contraction. When calcium is pumped back into the sarcoplasmic reticulum by SERCA, TnC releases its calcium, TnI rebinds actin, tropomyosin slides back over the myosin-binding sites, and the muscle relaxes.
Why Troponin Leaks in Two Phases
Ischemia lasting beyond roughly 20–40 minutes produces irreversible cardiomyocyte injury and disruption of the sarcolemmal membrane. Troponin then escapes in two distinct waves, and this is what gives the blood test its characteristic shape:
- The free cytoplasmic pool — a small unbound reservoir representing roughly 2–8% of the cell's total troponin — washes out first, producing the early rise in serum troponin within a few hours.
- The structurally bound complexes — the great majority of the protein, tethered to the thin filament — are degraded and released far more slowly over the following days, which is why troponin stays elevated long after the event.
That slow second phase is diagnostically valuable: a patient who presents days after an episode of chest pain may still have measurable troponin from the original event, allowing a subacute MI to be identified retrospectively.
Why Troponin Testing Is Ordered
Cardiac troponin testing is ordered in a wide range of clinical situations:
- Suspected acute myocardial infarction (AMI): Any patient presenting to an emergency department with chest pain, shortness of breath, arm or jaw pain, or other symptoms suggestive of a heart attack receives serial troponin measurements as part of the standard workup. A rising and falling pattern of troponin elevation is pathognomonic for AMI.
- Risk stratification in acute coronary syndromes (ACS): Patients with unstable angina or non-ST-elevation myocardial infarction (NSTEMI) are stratified by troponin level to guide urgency of intervention -- those with elevated troponin face higher short-term mortality risk and typically require earlier invasive evaluation.
- Post-cardiac surgery monitoring: Troponin is released during bypass surgery and other cardiac procedures; serial measurements help identify procedure-related myocardial injury.
- Suspected myocarditis or pericarditis: Inflammatory conditions of the heart muscle or pericardium can elevate troponin to varying degrees.
- Heart failure assessment: Chronically elevated low-level troponin in heart failure patients correlates with ongoing myocardial stress and adverse prognosis.
- Cardiotoxicity monitoring: Cancer patients receiving cardiotoxic chemotherapy agents (such as anthracyclines or trastuzumab) are monitored with serial troponin to detect early myocardial injury.
- Evaluation of other cardiac conditions: Pulmonary embolism, hypertensive emergencies, and sepsis can all cause secondary cardiac injury detectable by troponin elevation.
How the Test Is Performed
Cardiac troponin is measured from a standard venous blood draw. No fasting is required. The sample is sent to the clinical laboratory immediately -- troponin testing in emergency settings is typically processed as a STAT (urgent) order with results available within 30-60 minutes in most hospital laboratories running on-site analyzers.
Because troponin rises progressively after cardiac injury rather than instantly, serial sampling is essential for diagnosis. Most current rapid rule-in/rule-out protocols use either:
- 0h/3h protocol: Blood drawn at presentation and repeated 3 hours later. A significant rise or fall between the two samples confirms acute myocardial injury.
- 0h/1h protocol (high-sensitivity assays only): The faster kinetics of high-sensitivity assays allow meaningful risk stratification within just one hour of the first draw. This protocol is now standard in many European and some US emergency departments.
- 0h/2h protocol: An intermediate protocol used by some centers as a compromise between speed and diagnostic confidence.
Point-of-care (POC) troponin devices are also available for bedside testing in pre-hospital settings or resource-limited environments, though laboratory-based assays remain the gold standard for sensitivity and precision.
Troponin I vs. Troponin T: Differences
Both cardiac troponin I (cTnI) and cardiac troponin T (cTnT) are equally accepted as diagnostic markers for myocardial injury. They are structurally distinct proteins encoded by different genes, and their clinical performance characteristics differ slightly:
Cardiac Troponin I (cTnI):
- Encoded by the TNNI3 gene on chromosome 19.
- No skeletal muscle isoform at any developmental stage -- true cardiac specificity.
- Multiple manufacturers produce cTnI assays, but without standardization across platforms, reference ranges vary significantly between laboratories and cannot be directly compared.
- May remain elevated for 7-10 days after a large MI, providing a window to diagnose patients who present late.
Cardiac Troponin T (cTnT):
- Encoded by the TNNT2 gene on chromosome 1.
- A fetal skeletal muscle isoform of troponin T exists but is not expressed in healthy adult skeletal muscle. However, in patients with severe skeletal muscle disease (polymyositis, Duchenne muscular dystrophy), re-expression of the fetal isoform can cause false-positive cTnT elevation.
- Manufactured by a single company (Roche Diagnostics), meaning all cTnT results worldwide are generated on the same assay platform with standardized reference ranges.
- High-sensitivity cTnT (hs-cTnT, 5th generation) is the most widely implemented high-sensitivity cardiac troponin assay globally.
For practical purposes in non-skeletal-muscle-disease patients, cTnI and cTnT perform equivalently and either is acceptable for AMI diagnosis and risk stratification.
Reference Ranges and Result Interpretation
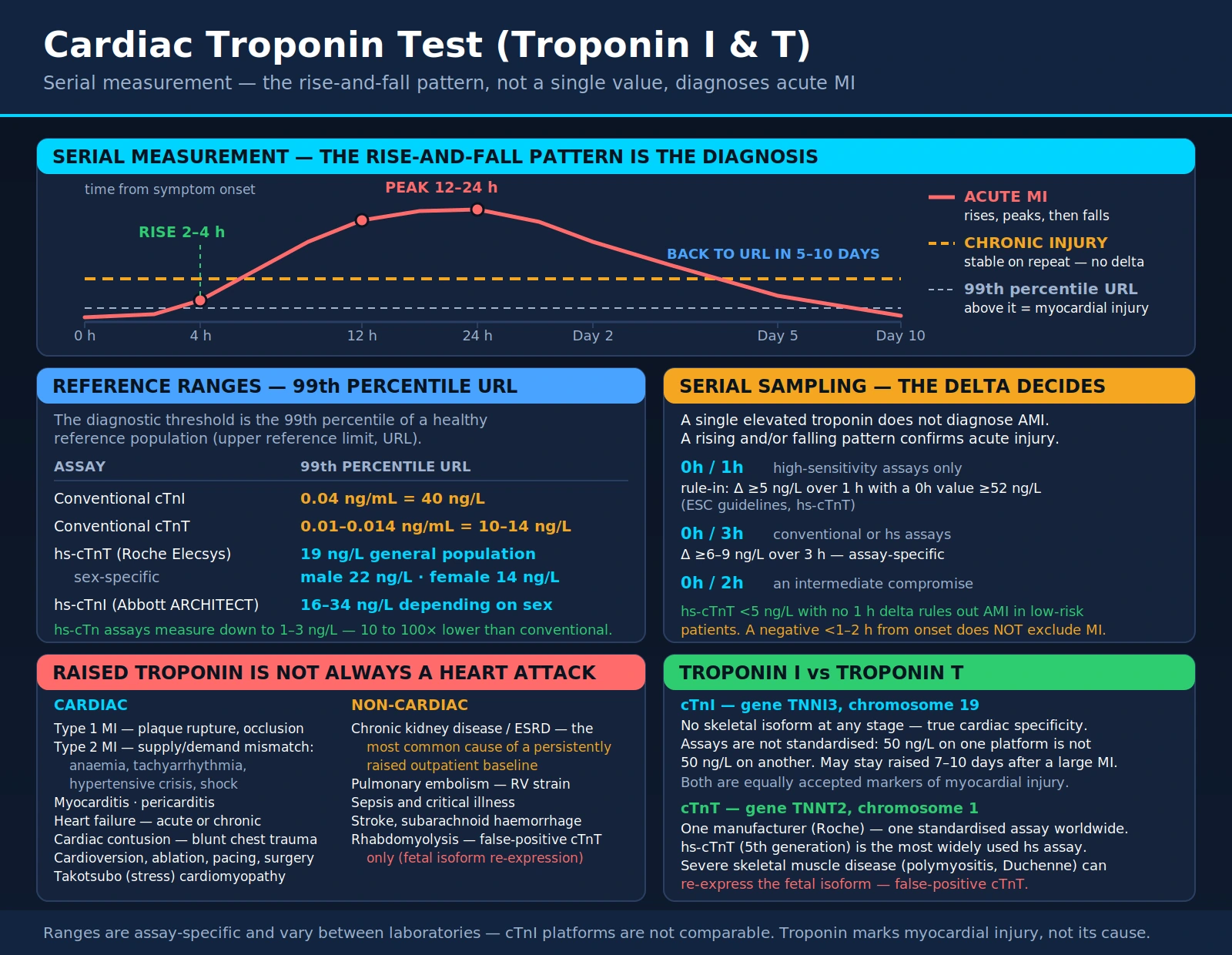
Troponin reference ranges are assay-specific and vary between laboratories. The universal diagnostic threshold for acute myocardial injury is the 99th percentile of a healthy reference population (also called the upper reference limit or URL). Any troponin elevation above the 99th percentile URL is considered abnormal and indicates myocardial injury.
Typical conventional troponin ranges (exact values differ by assay platform):
- Conventional cTnI: URL typically 0.04 ng/mL or 40 ng/L (varies widely by platform).
- Conventional cTnT: URL typically 0.01-0.014 ng/mL or 10-14 ng/L.
- High-sensitivity cTnT (hs-cTnT, Roche Elecsys): 99th percentile URL = 19 ng/L in the general population, with sex-specific thresholds (males 22 ng/L, females 14 ng/L). Results below 5 ng/L combined with no delta change over 1 hour can rule out AMI in low-risk patients.
- High-sensitivity cTnI (varies by manufacturer): Abbott ARCHITECT hs-cTnI 99th percentile = 16-34 ng/L depending on sex; Siemens Atellica hs-cTnI thresholds differ similarly.
A note on the hs-cTnT numbers above. The 19 / 22 / 14 ng/L set is the FDA-cleared US package-insert value for the fifth-generation Elecsys hs-cTnT assay. The same assay is sold outside the United States with a lower published set — approximately 14 ng/L overall, about 9 ng/L for women and about 15.5 ng/L for men — and the European rapid-triage algorithms described below were validated against those lower figures. Both sets are legitimate; they belong to different regulatory versions of one assay. The practical consequence is that a troponin result must be read against the reference limits printed on the report by the laboratory that ran it, never against a number remembered from elsewhere. The 99th percentile itself, despite periodic arguments for higher cutoffs, remains the best-established diagnostic threshold in the field.
Results must always be interpreted in clinical context:
- A single elevated troponin does not diagnose AMI -- serial measurements showing a rising and/or falling pattern (delta change) confirm acute myocardial injury.
- A stable chronically elevated troponin (same level on serial measurements hours apart) suggests a non-acute cause such as chronic kidney disease, heart failure, or myocarditis.
- Troponin below the URL does not rule out all cardiac pathology -- very early presentation (within 1-2 hours of symptom onset) may precede measurable troponin rise.
Why the Reference Range Differs by Sex
Women consistently have lower 99th percentile troponin concentrations than men, for both hs-cTnT and hs-cTnI. Applying a sex-specific URL rather than one combined number does two things at once:
- It raises sensitivity in women, who were historically under-diagnosed because they presented with lower absolute troponin values that fell below a sex-neutral threshold set largely by male physiology.
- It raises specificity in men, avoiding false-positive MI diagnoses driven by physiologically higher male baseline troponin.
The 2018 Fourth Universal Definition of Myocardial Infarction recommends sex-specific URLs wherever they have been validated for the assay in use. A laboratory that reports a single combined threshold is, in effect, reproducing the same under-diagnosis of women that existed before high-sensitivity assays arrived.
Why the Reference Range Rises With Age
The 99th percentile climbs substantially with age even among people considered healthy. This is not a laboratory artifact — it reflects genuine subclinical myocardial injury accumulating from hypertension, silent coronary disease, left ventricular hypertrophy, and early kidney impairment. Age-specific percentile tables have been published for some assays. Clinically, the implication is that an 82-year-old with an hs-cTnT of 20 ng/L may be sitting at a stable personal baseline rather than having an acute event, and only the rise-and-fall pattern across serial draws can tell the two apart.
The Rise/Fall (Delta) Criterion
A single value above the 99th percentile establishes myocardial injury. It does not establish acute myocardial infarction, which additionally requires a dynamic change indicating an evolving process. The key delta thresholds for hs-cTnT are:
- 0h/1h algorithm: an absolute 1-hour rise of ≥5 ng/L (read together with the 0h value) triggers rule-in; a very low baseline with a 1-hour change below 3 ng/L permits rule-out.
- 0h/3h algorithm: a significant change means a relative change of ≥20% and an absolute change exceeding the smallest difference the assay can reliably distinguish.
- Chronic stable elevation: no meaningful delta across serial draws, indicating ongoing but non-acute myocardial injury — heart failure, chronic kidney disease, or a stable cardiomyopathy.
The Troponin Rise-and-Fall Pattern
The characteristic biokinetic pattern of troponin in acute MI is a rise-and-fall curve that reflects the release and gradual clearance of troponin from damaged cardiomyocytes. Understanding this pattern is essential for interpreting serial results:
- Onset: Troponin begins to rise in the bloodstream approximately 2-4 hours after the onset of myocardial ischemia, as cell membrane integrity breaks down.
- Peak: Troponin typically peaks at 12-24 hours after symptom onset in most AMIs. With successful reperfusion (via thrombolysis or percutaneous coronary intervention), the peak may occur earlier and be followed by a more rapid decline -- a pattern called "washout" that indicates effective restoration of blood flow.
- Return to baseline: Conventional troponin returns to the URL within 5-10 days after a large MI. High-sensitivity troponin may normalize more quickly. The prolonged elevation window allows diagnosis of patients who present days after their event (subacute MI).
The delta change (absolute or relative change between serial measurements) is a critical diagnostic concept. Current European Society of Cardiology (ESC) guidelines define the following delta thresholds for hs-cTnT rule-in:
- 0h/1h protocol: Absolute delta of ≥5 ng/L over 1 hour (or an absolute 0h value ≥52 ng/L) is a rule-in criterion for AMI.
- 0h/3h protocol: Absolute delta of ≥6-9 ng/L over 3 hours (assay-specific) indicates acute myocardial injury.
Rapid Rule-In and Rule-Out Algorithms
The 2020 ESC guidelines for acute coronary syndromes without persistent ST-segment elevation define three validated high-sensitivity troponin algorithms for emergency chest-pain evaluation. All of them replace the old practice of holding a patient for six or more hours of serial draws before a decision could be made.
The 0h/1h Algorithm (Preferred)
Two hs-cTn measurements are taken: one at presentation and one exactly one hour later. Patients then fall into one of three zones. The figures below are for hs-cTnT on the Roche Elecsys platform, as validated in the TRAPID-AMI multicenter study of 1,282 patients:
- Rule out — 0h hs-cTnT below 12 ng/L and a 1-hour change below 3 ng/L. In TRAPID-AMI this captured 63.4% of all patients, with a negative predictive value of 99.1% (95% CI 98.2–99.7%) and sensitivity of 96.7%. The ESC algorithm adds a second rule-out route: a 0h value below 5 ng/L in a patient whose chest pain began more than three hours earlier can be ruled out on the single draw.
- Rule in — 0h hs-cTnT of 52 ng/L or above, or a 1-hour rise of 5 ng/L or more. This captured 14.4% of patients, with a positive predictive value of 77.2% and specificity of 96.1%. These patients need cardiology involvement and, in most cases, angiography.
- Observation zone — neither criterion met, covering the remaining 22.2%. The MI prevalence in this group was 22.5%, so it is genuinely indeterminate rather than reassuring: a 3-hour sample plus clinical reassessment is required.
The specific ng/L values are assay-dependent and are not transferable. The thresholds above apply to Roche Elecsys hs-cTnT; Abbott and Siemens hs-cTnI platforms have their own separately validated numbers, and using one assay's cut-points with another assay's results is a serious error.
The 0h/2h Algorithm
An alternative for departments where a precise one-hour re-draw is logistically difficult. Two samples are taken at presentation and two hours later. Rule-out requires both values below the assay-specific low threshold with a change below the absolute cut-point; rule-in requires a markedly elevated presenting value or a large 2-hour delta. Negative predictive value is comparable at roughly 99%, but rule-out efficiency is lower — about half of patients are dischargeable, versus roughly three in five with the 0h/1h approach.
The 0h/3h Algorithm
The original rapid algorithm, still used where one-hour logistics have not been established. It applies the fixed 99th percentile threshold plus a significant delta (a relative change above 20%, or an absolute change above the assay's minimum significant difference) across three hours. Negative predictive value is around 99%, but the patient occupies an emergency department bed three times as long as under the 0h/1h protocol.
The HEART Score
Troponin is one input, not the whole decision. The HEART score is a validated five-component clinical decision tool — History, ECG, Age, Risk factors, Troponin — that scores each element 0, 1, or 2 for a total of 0 to 10, and sorts chest-pain patients into three risk bands by their 30-day rate of major adverse cardiac events (MACE):
- Low risk (0–3): 30-day MACE rate under 2%. Combined with an hs-cTn below the 99th percentile at presentation, multiple validation studies support discharge without a full serial-troponin workup.
- Intermediate risk (4–6): observation with serial troponin, followed by stress testing or CT coronary angiography.
- High risk (7–10): cardiology consultation and, typically, invasive coronary angiography.
The original prospective validation across four Dutch hospitals confirmed that the score outperformed the older TIMI and GRACE scores for this specific question — which undifferentiated chest-pain patient can safely go home.
The Five Types of Myocardial Infarction
The Fourth Universal Definition of Myocardial Infarction classifies MI into five types by pathophysiology, not by troponin magnitude. Two patients can have identical troponin values and need completely different treatment, so this classification carries real therapeutic weight.
Type 1 — Atherosclerotic Plaque Event
Spontaneous MI caused by atherosclerotic plaque rupture, erosion, or fissuring with intraluminal thrombus formation, leading to acute coronary occlusion or sharply reduced coronary flow. This is the classic heart attack, presenting as either STEMI or NSTEMI. Treatment is urgent revascularization — percutaneous coronary intervention preferred — plus dual antiplatelet therapy, anticoagulation, a high-intensity statin, an ACE inhibitor or ARB, and a beta-blocker.
Type 2 — Supply-Demand Mismatch
Myocardial injury caused by something other than plaque disruption, in which oxygen demand outstrips supply. Troponin rises and falls as it does in Type 1, but coronary angiography reveals no culprit lesion. Common triggers include:
- Tachyarrhythmia — atrial fibrillation with rapid ventricular response, producing rate-related subendocardial ischemia.
- Hypotension and shock — hemorrhagic, distributive (sepsis), or cardiogenic, all reducing global coronary supply.
- Severe anemia — hemoglobin below roughly 7 g/dL sharply reduces oxygen-carrying capacity, and demand outruns supply in any territory served by a fixed coronary stenosis.
- Hypertensive emergency — extreme afterload driving subendocardial ischemia.
- Coronary vasospasm — Prinzmetal angina, and cocaine-induced spasm.
- Pulmonary embolism — acute right-heart pressure overload causing right ventricular free-wall ischemia.
Management of Type 2 MI centers on correcting the underlying condition. The benefit of antiplatelet and anticoagulant therapy here is much less well established than in Type 1, and reflexively treating a Type 2 event as though it were a Type 1 can do harm — particularly in a bleeding or septic patient.
Types 3, 4, and 5
- Type 3: sudden cardiac death with ischemic symptoms and new ECG changes, where the patient died before biomarkers could be drawn or before results returned.
- Type 4a: MI associated with percutaneous coronary intervention — defined as troponin elevation greater than 5× the URL within 48 hours of the procedure, together with ECG or imaging evidence of new ischemia.
- Type 4b: MI caused by stent thrombosis.
- Type 4c: MI related to in-stent restenosis.
- Type 5: MI associated with coronary artery bypass grafting — defined as troponin elevation greater than 10× the URL within 48 hours, together with new Q waves, new left bundle branch block, or imaging evidence of new loss of viable myocardium.
The higher multiples required for Types 4a and 5 exist because both procedures cause some myocardial injury by design; the threshold has to clear that expected background before a procedural infarction can be called.
Conditions That Elevate Troponin
While troponin elevation is most strongly associated with acute MI, it can also be elevated in a broad range of other conditions. Clinicians must consider these alternatives -- sometimes called "type 2 MI" or non-ischemic troponin elevation -- when evaluating a positive result:
Primary cardiac causes:
- Acute myocardial infarction (Type 1 MI): Plaque rupture causing coronary artery occlusion -- the classic heart attack.
- Type 2 MI: Myocardial ischemia due to supply-demand mismatch without plaque rupture (e.g., severe anemia, tachyarrhythmias, hypertensive crisis, shock).
- Myocarditis: Viral or autoimmune inflammation of the heart muscle can cause significant troponin elevation mimicking AMI.
- Heart failure (acute decompensated or chronic): Low-level troponin release is common in heart failure due to ongoing myocardial stretch and ischemia.
- Cardiac contusion: Blunt chest trauma can cause myocardial injury detectable by troponin elevation.
- Cardiac procedures: Cardioversion, ablation, pacemaker implantation, and cardiac surgery all cause procedural troponin release.
- Takotsubo (stress) cardiomyopathy: Transient apical ballooning syndrome caused by catecholamine surge, often after emotional or physical stress.
Non-cardiac causes (secondary myocardial injury):
- Pulmonary embolism: Right ventricular strain from massive PE causes troponin elevation proportional to the degree of hemodynamic compromise.
- Chronic kidney disease (CKD) and end-stage renal disease (ESRD): Reduced troponin clearance and chronic low-level myocardial injury commonly cause persistently elevated baseline troponin in CKD patients.
- Sepsis and critical illness: Systemic inflammation and microvascular injury in sepsis regularly cause troponin elevation as a marker of severity.
- Stroke and subarachnoid hemorrhage: Neurogenic cardiac injury from catecholamine surges caused by intracranial events elevates troponin.
- Rhabdomyolysis: Severe skeletal muscle breakdown -- with cTnT (not cTnI) showing false-positive elevation due to re-expression of fetal isoforms in diseased muscle.
Non-Coronary Causes in Depth
Any condition that injures cardiomyocytes will raise troponin, whether or not a coronary artery is involved. The list above is the quick reference; what follows is the detail that matters when a troponin comes back positive and the coronary arteries turn out to be clean.
Myocarditis
Inflammation of the myocardium arising from viral infection (coxsackievirus B, adenovirus, parvovirus B19, influenza, SARS-CoV-2), autoimmune processes (giant cell myocarditis, eosinophilic myocarditis), or toxic exposures (anthracyclines, immune checkpoint inhibitors). Troponin can be markedly elevated, and the ECG may show diffuse ST elevation that mimics a STEMI closely enough to send a patient to the catheterization laboratory. The angiogram shows normal or non-obstructive arteries. Cardiac MRI with late gadolinium enhancement is the key diagnostic tool, showing a patchy, often subepicardial pattern that does not follow a coronary territory.
Pulmonary Embolism
Acute massive or submassive pulmonary embolism causes abrupt right ventricular pressure overload. The RV free wall, which is normally perfused at low pressure and has little reserve, sustains subendocardial ischemia when intracavitary pressure rises suddenly. Troponin elevation in pulmonary embolism independently predicts 30-day mortality and is built into risk-stratification tools such as the PESI and simplified PESI scores. In a hemodynamically unstable patient, an elevated troponin is one of the findings that pushes toward systemic thrombolysis or catheter-directed therapy rather than anticoagulation alone.
Acute Decompensated Heart Failure
Both acute and chronic heart failure are associated with troponin elevation. During acute decompensation, cardiomyocyte injury comes from several directions at once: a raised left ventricular end-diastolic pressure compresses subendocardial perfusion, catecholamine excess drives demand up, and neurohormonal activation adds further stress. Chronic low-level troponin elevation is a powerful independent predictor of mortality in both HFrEF and HFpEF — serial hs-cTnT measurement in two large randomized heart-failure trial populations showed that both the baseline concentration and its change over time carried prognostic information beyond natriuretic peptides.
Takotsubo (Stress) Cardiomyopathy
Also called apical ballooning syndrome or broken heart syndrome. A massive catecholamine surge — emotional shock, severe physical stress, the post-surgical state — produces a transient wall-motion abnormality with ballooning of the left ventricular apex and preserved or hyperdynamic basal contraction, giving the characteristic "octopus pot" shape on ventriculography that named the syndrome. Troponin rises, though usually to a lower peak than an equivalent-territory STEMI would produce, and the disproportion between a modest troponin and a large wall-motion abnormality is itself a diagnostic clue. Coronary angiography shows no obstructive disease, and ejection fraction typically recovers within four to six weeks.
Sepsis-Induced Cardiomyopathy
Direct cardiomyocyte injury from circulating cytokines (TNF-alpha, IL-1beta, IL-6), endotoxin, reactive oxygen species, and nitric oxide produces a reversible myocardial depression in an estimated 10–50% of septic patients. Troponin elevation in sepsis is an independent predictor of ICU mortality. cTnI is generally the more interpretable marker in this setting, because cTnT tends to be disproportionately elevated when the acute kidney injury that so often accompanies sepsis alters its clearance.
Chronic Kidney Disease and Dialysis
Both cTnI and cTnT run chronically elevated in chronic kidney disease. The cause is a combination of reduced clearance, uremia-mediated cardiomyocyte injury, left ventricular hypertrophy, and a genuinely high prevalence of subclinical coronary disease — it is not simply a laboratory artifact, and the elevation carries real prognostic weight. cTnT tends to be proportionally more elevated than cTnI in this population. In dialysis patients the absolute number is nearly uninterpretable on its own; troponin must be measured serially (presentation and 3–6 hours) so that a dynamic change can be detected against the patient's own elevated baseline.
Skeletal Muscle Disease and Rhabdomyolysis
This is the one situation where the choice of assay changes the answer, and it is easy to get backwards. Severely diseased or regenerating skeletal muscle — Duchenne muscular dystrophy, polymyositis, rhabdomyolysis — re-expresses cardiac troponin T isoforms, producing genuinely elevated cTnT with no cardiac injury at all. cTnI does not share this behavior. In a patient with a myopathy and a raised cTnT but a normal ECG and no cardiac symptoms, measuring cTnI on a different platform is the fastest way to resolve the question.
Other Causes
- Cardiac contusion: blunt chest trauma from a motor vehicle collision, defibrillation, or a direct precordial blow. Troponin elevation correlates with injury severity and with arrhythmia risk, and is used to decide who needs cardiac monitoring.
- Ablation and cardioversion: iatrogenic myocardial injury from radiofrequency or electrical energy, expected rather than alarming.
- Chemotherapy: anthracyclines (doxorubicin, daunorubicin) cause dose-dependent cardiomyocyte injury; trastuzumab causes a distinct, more often reversible cardiomyopathy; immune checkpoint inhibitors can trigger fulminant myocarditis with massive troponin elevation and mortality above 50% if immunosuppression is not started promptly. This is why serial troponin is built into cardio-oncology monitoring protocols.
- Stroke and subarachnoid hemorrhage: neurogenic cardiac injury from a massive catecholamine release, presenting with troponin elevation, wall-motion abnormalities, and QTc prolongation that together can mimic an MI.
- Severe hypothyroidism: myxedema can raise troponin through a metabolic cardiomyopathy.
High-Sensitivity Troponin (hs-cTn)
High-sensitivity cardiac troponin (hs-cTn) assays represent a major technological advance over conventional troponin assays. The key differences:
- Lower detection limit: hs-cTn assays can measure troponin concentrations 10-100 times lower than conventional assays, detecting concentrations as low as 1-3 ng/L.
- Measurability in healthy individuals: A defining characteristic of hs-cTn assays is that they can measure troponin in at least 50% of a healthy reference population (many assays measure detectable concentrations in 95%+ of healthy adults). This is in contrast to conventional assays where most healthy individuals have undetectable levels.
- Faster rule-out: The superior sensitivity enables rapid 0h/1h rule-out protocols -- a patient with very low hs-cTn at presentation and a minimal delta at 1 hour has a negative predictive value exceeding 99% for AMI.
- Sex-specific thresholds: Women have lower baseline troponin levels than men. hs-cTn assays have established sex-specific 99th percentile URLs (e.g., hs-cTnT females 14 ng/L vs. males 22 ng/L), which improves detection of MI in women, who have historically been underdiagnosed.
- Population-based chronic disease monitoring: Because hs-cTn detects subclinical myocardial injury, it is increasingly studied as a chronic disease risk marker -- elevated hs-cTn in community-dwelling adults predicts future cardiovascular events, heart failure, and mortality even in the absence of acute symptoms.
The adoption of hs-cTn has increased the diagnosis of MI -- particularly in women and patients presenting atypically -- while simultaneously allowing many patients with chest pain to be safely discharged faster with a definitive rule-out rather than extended observation.
What Officially Makes an Assay "High-Sensitivity"
The generation of a troponin assay is not defined by a particular technology but by two analytical performance criteria set out by the International Federation of Clinical Chemistry (IFCC):
- Conventional (contemporary) assays: a coefficient of variation greater than 10% at the 99th percentile, and measurable troponin in fewer than 50% of healthy individuals. Older platforms such as the Abbott AxSYM cTnI and the first-generation Roche Elecsys cTnT fall here.
- High-sensitivity assays: a coefficient of variation of 10% or less at the 99th percentile and measurable troponin in more than 50% of healthy individuals — ideally more than 95%.
The imprecision criterion matters as much as the detection criterion. An assay that can technically report very low numbers but scatters them by 20% run to run cannot support a rule-out decision based on a 3 ng/L change; the whole 0h/1h approach depends on the assay being able to distinguish a small real change from its own noise. The second criterion produces the conceptual shift: because troponin is now measurable at physiological background levels in nearly everyone, clinicians can track a dynamic change from an individual's own baseline instead of waiting for a threshold to be crossed from "undetectable."
Major Validated Platforms
- hs-cTnT (Roche Elecsys): the most extensively studied assay in the world, and the one used in the validation studies behind the ESC 0h/1h and 0h/2h algorithms.
- hs-cTnI (Abbott): 99th percentile of roughly 16–34 ng/L depending on sex and manufacturer guidance; validated in the APACE and HIGH-US cohorts.
- hs-cTnI (Siemens): validated for 0h/1h use with its own absolute thresholds, which differ from Abbott's.
- Point-of-care hs-cTn devices are now available for settings where central laboratory turnaround exceeds 60 minutes, though laboratory analyzers remain the reference for precision.
Before high-sensitivity assays, troponin was undetectable at presentation in most NSTEMI patients, and confirming a rise took serial draws at 0, 3, and 6 hours. The 0h/1h algorithm compresses that to a decision inside two hours for roughly three in five patients — the single largest change in emergency chest-pain practice in thirty years. The corresponding hazard is that assay thresholds are not interchangeable: a hospital switching platforms must re-derive its cut-points, and published guidance exists specifically for institutions making that transition.
How to Reduce Cardiac Risk
For patients who have experienced a troponin-positive event or who are at elevated cardiovascular risk, the following evidence-based strategies reduce future myocardial injury and cardiac events:
Lifestyle Foundations
- Adopt a Mediterranean-style or whole-food anti-inflammatory diet: Emphasize vegetables, fruits, legumes, nuts, olive oil, and fatty fish. Reduce ultra-processed foods, refined carbohydrates, and trans fats. The PREDIMED trial demonstrated a 30% reduction in major cardiovascular events with Mediterranean diet adherence.
- Regular exercise: Moderate-intensity aerobic exercise (150+ minutes per week) reduces cardiovascular risk by improving endothelial function, lowering blood pressure, reducing inflammation, and improving lipid profiles. Cardiac rehabilitation programs after MI reduce mortality by approximately 25%.
- Smoking cessation: Smoking is a powerful independent risk factor for coronary artery disease and thrombosis. Cessation reduces MI risk substantially within 1-2 years.
- Optimize body weight: Obesity, particularly visceral adiposity, drives systemic inflammation, insulin resistance, hypertension, and dyslipidemia -- all contributors to coronary artery disease.
- Stress management: Acute psychological stress triggers catecholamine surges that can precipitate takotsubo cardiomyopathy and coronary spasm. Chronic stress promotes inflammation and unhealthy behaviors. Meditation, yoga, and stress reduction programs have measurable cardiovascular benefits.
Targeted Nutritional Support
- Omega-3 fatty acids: EPA and DHA reduce triglycerides, decrease inflammation, and have anti-arrhythmic properties. High-dose (4g/day) prescription EPA (icosapent ethyl, Vascepa) reduced cardiovascular events by 25% in the REDUCE-IT trial in high-risk patients.
- Magnesium: Magnesium deficiency is associated with arrhythmias, hypertension, and endothelial dysfunction. Adequate intake or supplementation with magnesium glycinate or malate (200-400 mg/day) supports cardiac function.
- Coenzyme Q10: CoQ10 is essential for mitochondrial energy production in cardiomyocytes. Supplementation (200-300 mg/day) may improve cardiac function in heart failure and reduce statin-related myopathy without compromising statin efficacy.
Medical Management After AMI
For patients who have had a confirmed MI with troponin elevation, guideline-directed medical therapy typically includes dual antiplatelet therapy, high-intensity statin therapy, ACE inhibitors or ARBs (especially with reduced ejection fraction), beta-blockers (in the acute setting and for reduced ejection fraction), and aldosterone antagonists when indicated. These medications have robust evidence for reducing recurrent MI, heart failure, and death.
Limitations of Troponin Testing
- Not synonymous with heart attack: Troponin elevation means myocardial injury, not necessarily coronary artery disease. The clinical context, ECG, symptoms, and imaging findings are all required for proper diagnosis.
- False positives in kidney disease: CKD is the most common cause of persistently elevated baseline troponin in the outpatient setting, making acute change (delta) -- not absolute value -- essential for AMI diagnosis in these patients.
- Early false negatives: If a patient presents within 1-2 hours of symptom onset, troponin may not yet have risen to detectable levels. A negative initial troponin in this early window does not exclude MI -- serial testing is mandatory.
- Assay non-standardization for cTnI: Unlike cTnT (single manufacturer), cTnI assays from different companies cannot be directly compared. A result of 50 ng/L on one cTnI platform does not equal 50 ng/L on another platform.
- Does not localize injury: Troponin indicates that cardiac injury occurred but does not identify which coronary territory is affected. ECG, echocardiography, and coronary angiography are required to localize and characterize the injury.
- Does not measure cardiac function: Troponin is a biomarker of injury, not of systolic or diastolic function. BNP/NT-proBNP are the preferred biomarkers for assessing heart failure severity and ventricular wall stress.
Key Research Papers
Every citation below was checked against the PubMed record on 25 July 2026; the title, journal, volume, and pages match the linked PMID.
Guidelines and Definitions
- Thygesen K, Alpert JS, Jaffe AS, et al. Fourth Universal Definition of Myocardial Infarction (2018). J Am Coll Cardiol. 2018;72(18):2231–2264. PMID: 30153967
- Collet JP, Thiele H, Barbato E, et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2021;42(14):1289–1367. PMID: 32860058
- Januzzi JL Jr, Mahler SA, Christenson RH, et al. Recommendations for Institutions Transitioning to High-Sensitivity Troponin Testing: JACC Scientific Expert Panel. J Am Coll Cardiol. 2019;73(9):1059–1077. PMID: 30798981
Rapid Rule-Out Algorithms and Early Diagnosis
- Mueller C, Giannitsis E, Christ M, et al. Multicenter Evaluation of a 0-Hour/1-Hour Algorithm in the Diagnosis of Myocardial Infarction With High-Sensitivity Cardiac Troponin T (TRAPID-AMI). Ann Emerg Med. 2016;68(1):76–87. PMID: 26794254
- Reichlin T, Hochholzer W, Bassetti S, et al. Early diagnosis of myocardial infarction with sensitive cardiac troponin assays. N Engl J Med. 2009;361(9):858–867. PMID: 19710484
- Keller T, Zeller T, Peetz D, et al. Sensitive troponin I assay in early diagnosis of acute myocardial infarction. N Engl J Med. 2009;361(9):868–877. PMID: 19710485
- Body R, Carley S, McDowell G, et al. Rapid exclusion of acute myocardial infarction in patients with undetectable troponin using a high-sensitivity assay. J Am Coll Cardiol. 2011;58(13):1332–1339. PMID: 21920261
- Shah AS, Anand A, Sandoval Y, et al. High-sensitivity cardiac troponin I at presentation in patients with suspected acute coronary syndrome: a cohort study. Lancet. 2015;386(10012):2481–2488. PMID: 26454362
- Backus BE, Six AJ, Kelder JC, et al. A prospective validation of the HEART score for chest pain patients at the emergency department. Int J Cardiol. 2013;168(3):2153–2158. PMID: 23465250
Assay Characteristics and Reference Limits
- Apple FS, Collinson PO; IFCC Task Force on Clinical Applications of Cardiac Biomarkers. Analytical characteristics of high-sensitivity cardiac troponin assays. Clin Chem. 2012;58(1):54–61. PMID: 21965555
- Giannitsis E, Kurz K, Hallermayer K, et al. Analytical validation of a high-sensitivity cardiac troponin T assay. Clin Chem. 2010;56(2):254–261. PMID: 19959623
- Sandoval Y, Apple FS, Saenger AK, et al. 99th Percentile Upper-Reference Limit of Cardiac Troponin and the Diagnosis of Acute Myocardial Infarction. Clin Chem. 2020;66(9):1167–1180. PMID: 32871000
- Hammarsten O, Fu ML, Sigurjonsdottir R, et al. Troponin T percentiles from a random population sample, emergency room patients and patients with myocardial infarction. Clin Chem. 2012;58(3):628–637. PMID: 22258764
Troponin Beyond Acute MI
- de Lemos JA, Drazner MH, Omland T, et al. Association of troponin T detected with a highly sensitive assay and cardiac structure and mortality risk in the general population. JAMA. 2010;304(22):2503–2512. PMID: 21139111
- Masson S, Anand I, Favero C, et al. Serial measurement of cardiac troponin T using a highly sensitive assay in patients with chronic heart failure: data from 2 large randomized clinical trials. Circulation. 2012;125(2):280–288. PMID: 22139751
- Jaffe AS, Vasile VC, Milone M, et al. Diseased skeletal muscle: a noncardiac source of increased circulating concentrations of cardiac troponin T. J Am Coll Cardiol. 2011;58(17):1819–1824. PMID: 21962825
Risk Reduction After a Troponin-Positive Event
- Bhatt DL, Steg PG, Miller M, et al. Cardiovascular Risk Reduction with Icosapent Ethyl for Hypertriglyceridemia (REDUCE-IT). N Engl J Med. 2019;380(1):11–22. PMID: 30415628
- Estruch R, Ros E, Salas-Salvadó J, et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts (PREDIMED). N Engl J Med. 2018;378(25):e34. PMID: 29897866
Live PubMed Searches
- High-sensitivity troponin and acute MI diagnosis
- 0h/1h troponin rule-out protocol (ESC guidelines)
- Troponin rapid rule-out algorithm in the emergency department
- Cardiac troponin I vs. T in acute coronary syndrome
- Non-cardiac causes of troponin elevation
- Type 2 myocardial infarction and supply-demand mismatch
- Sex-specific troponin thresholds and women's MI diagnosis
- Troponin elevation in chronic kidney disease
- hs-cTn as a community cardiovascular risk biomarker
- Troponin in myocarditis diagnosis and prognosis
- Fourth Universal Definition of MI and troponin
- HEART score and chest pain risk stratification
External Authoritative Resources
- MedlinePlus — Laboratory Tests Reference
- Lab Tests Online — Patient-Oriented Lab Test Reference (AACC)
- StatPearls / NCBI Bookshelf — Cardiac Troponin
Connections
- All Lab Tests
- The Heart & Circulation — interactive animation
- Inflammatory Markers
- Coronary Calcium Score
- Lipid Panel
- Apolipoprotein B (ApoB)
- Lipoprotein(a)
- BNP / NT-proBNP
- D-Dimer
- hs-CRP
- Creatine Kinase (CK and CK-MB)
- Complete Blood Count
- Ferritin Test
- Kidney Function
- Homocysteine
- Heart Disease
- Cardiovascular Disease
- Heart Attack
- Heart Failure
- Atrial Fibrillation
- Magnesium