St. John's Wort for Mood and Seasonal Depression
Of all medicinal herbs, St. John's Wort carries the most poetically appropriate connection to seasonal mood: its bright yellow flowers traditionally bloom around the summer solstice (the Feast of St. John the Baptist on June 24), and its red-pigmented hypericin compound — the same molecule that turns the traditional infused oil deep crimson — is a photoreceptor that requires visible light to exert its full activity. Wheatley's pivotal 1999 trial (Current Medical Research and Opinion) was the first rigorous randomized investigation of hypericum specifically for Seasonal Affective Disorder (SAD), and subsequent research has explored the herb's utility in the broader category of mild winter mood symptoms, sub-syndromal winter blues that fall short of full DSM SAD criteria, and the question of whether hypericum works synergistically with bright-light therapy (10,000 lux) or is best used as an alternative for patients who cannot tolerate or arrange for light therapy. This deep-dive walks through the SAD literature, the hypericin photoreceptor hypothesis, the curious therapeutic paradox of a midsummer-blooming herb being clinically useful for winter depression, and the practical protocols for autumn-initiation prophylaxis.
Table of Contents
- Seasonal Affective Disorder — Clinical Definition and Epidemiology
- The Wheatley 1999 SAD Trial
- The Hypericin Photoreceptor Mood Hypothesis
- The Summer Solstice Paradox
- Hypericum vs Bright Light Therapy
- Combination Protocols: Hypericum + Light Therapy
- Sub-Syndromal SAD and Mild Winter Mood Symptoms
- Autumn-Initiation Prophylaxis Protocols
- Menopausal Mood Symptoms
- Premenstrual Syndrome (PMS) Applications
- Key Research Papers
- Connections
- Featured Videos
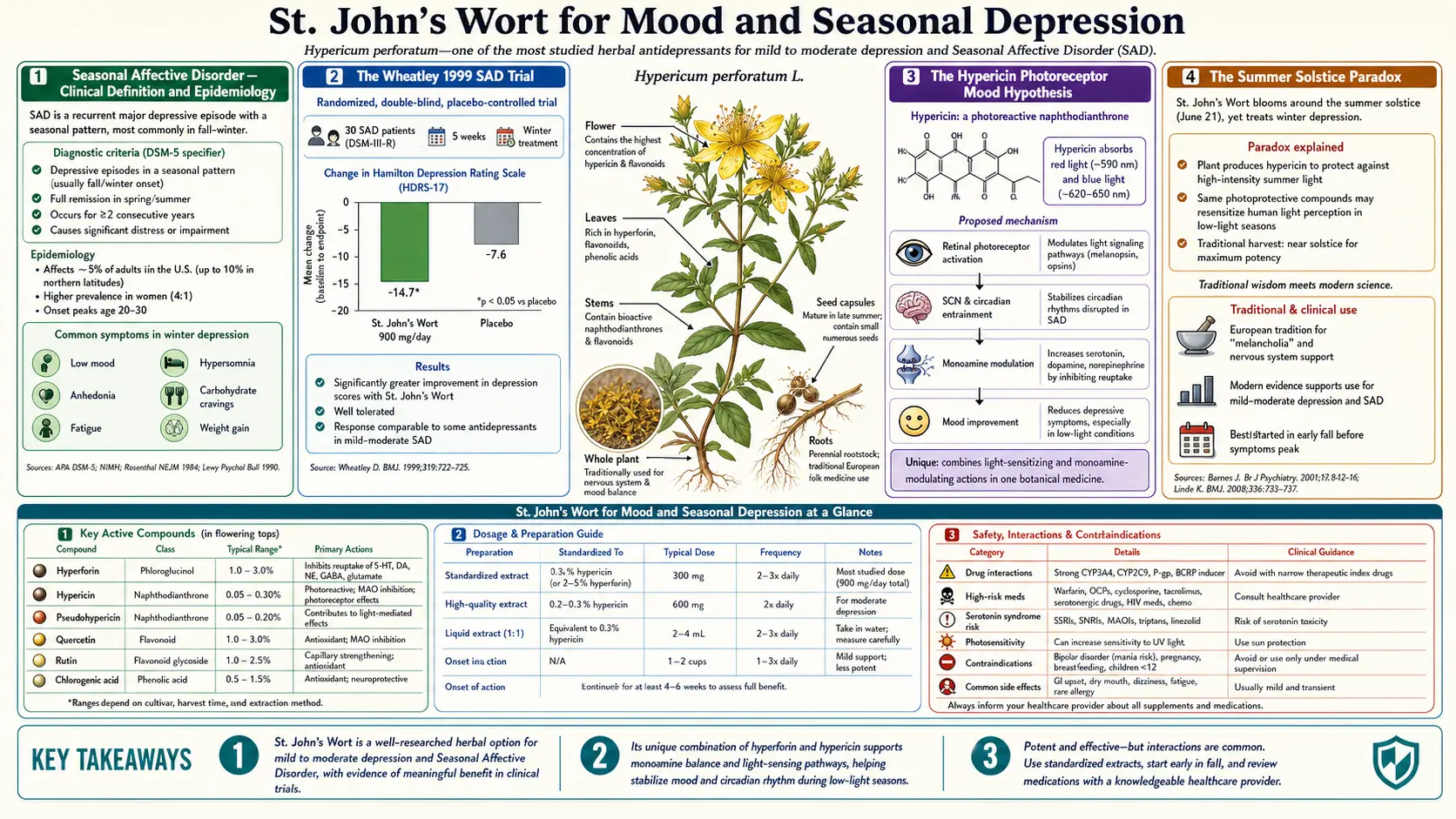
Seasonal Affective Disorder — Clinical Definition and Epidemiology
Seasonal Affective Disorder (SAD) is a recurrent form of major depressive disorder with a seasonal pattern, formally classified in the DSM-5 as "Major Depressive Disorder, Recurrent, with Seasonal Pattern." The full diagnostic criteria require:
- A regular temporal relationship between the onset of major depressive episodes and a specific time of year (typically autumn-onset, winter-pattern depression)
- Full remissions or shift to mania/hypomania at a characteristic time (typically spring)
- This seasonal pattern in the past two years with no non-seasonal episodes in the same period
- Seasonal episodes substantially outnumber non-seasonal episodes over the patient's lifetime
The most common SAD presentation is the autumn-winter pattern: depression onset in October-November, peak symptoms in December-February, remission in March-April. The atypical depression features distinguish SAD from non-seasonal major depression — SAD patients more often present with hypersomnia (oversleeping rather than insomnia), increased appetite with carbohydrate craving (rather than decreased appetite), weight gain (rather than weight loss), leaden paralysis (heavy-feeling limbs and fatigue), and social withdrawal.
Epidemiology: SAD prevalence varies strongly with latitude. In the northern United States and Canada, full SAD affects approximately 1-10% of the adult population, with sub-syndromal SAD (winter blues that fall short of full diagnostic criteria but cause meaningful impairment) affecting an additional 10-20%. Women are affected approximately 4 times more often than men. Onset is most common in young adulthood (20s-30s) with often a decades-long course of seasonal recurrence.
Standard treatments include bright light therapy (10,000 lux for 30 minutes daily, ideally morning), pharmaceutical antidepressants (SSRIs are first-line in DSM-aligned American practice, bupropion-XL extended release has an FDA indication specifically for SAD prevention with autumn initiation), cognitive behavioral therapy (CBT) adapted for SAD (CBT-SAD), and increasingly — in patients who decline or cannot tolerate pharmaceutical treatment — St. John's Wort.
The Wheatley 1999 SAD Trial
David Wheatley's 1999 study (published in Current Medical Research and Opinion) was the first rigorous randomized investigation of hypericum specifically for SAD. The trial design and findings:
- Population: 301 patients with established SAD (DSM-IV criteria) recruited across multiple UK general practices
- Intervention: hypericum standardized extract 900 mg/day (300 mg three times daily, standardized to 0.3% hypericin)
- Comparator arms: hypericum alone vs hypericum plus bright light therapy (3,000 lux for 2 hours daily) vs hypericum plus dim light (control light therapy at 300 lux)
- Duration: 8 weeks during the winter (November through February)
- Primary outcome: Hamilton Depression Rating Scale change from baseline
Results: All three arms showed significant improvement in depression scores. Mean HAM-D reduction was approximately 50% from baseline across arms, with bright-light combination showing modestly greater effect than hypericum alone, and dim-light combination showing intermediate results. Hypericum monotherapy produced a clinically meaningful improvement in SAD symptoms, with response rates comparable to those reported for pharmaceutical antidepressant trials in SAD.
The trial established two important points: (1) hypericum is efficacious as monotherapy for SAD, with effects in the same range as pharmaceutical SSRIs in SAD trials; and (2) the addition of bright light therapy to hypericum provides additional benefit, suggesting the two modalities work through complementary rather than redundant mechanisms. The Wheatley 1999 trial has been the foundation for hypericum's recommendation in European naturopathic guidelines for SAD ever since.
The Hypericin Photoreceptor Mood Hypothesis
One of the more intriguing speculative hypotheses about hypericum's mechanism in SAD specifically (as opposed to its general antidepressant mechanism via hyperforin) is the hypericin photoreceptor hypothesis. The starting observation: hypericin is a powerful photoactive molecule. Its absorption spectrum peaks in the visible blue-green range (around 590-610 nm and 540-560 nm), and when activated by visible light, it generates singlet oxygen and reactive oxygen species through Type I and Type II photodynamic mechanisms.
The speculative hypothesis — first articulated in the 1990s and elaborated by several investigators — proposes that hypericin in skin, retinal tissue, or possibly even circulating in plasma could act as a supplementary photoreceptor, "amplifying" the effect of ambient light on circadian rhythms and mood-regulating neural circuits. The mechanism would parallel the established melanopsin photoreceptor system in retinal ganglion cells that drives circadian entrainment, but with hypericin providing additional photic input particularly in the low-light conditions of winter.
The hypericin photoreceptor hypothesis has supporting and undermining evidence:
- Supporting: hypericin clearly is photoactive in vitro and in skin (photosensitization is the dose-limiting side effect of high-dose hypericum). The seasonal pattern of SAD is unambiguously tied to ambient light deprivation. Hypericum's effect in SAD trials is at least as good as in non-seasonal depression trials, possibly suggesting some seasonal-specific mechanism in addition to general antidepressant action
- Undermining: the plasma concentrations of hypericin achieved with oral hypericum dosing are very low (nanomolar range), arguably below the threshold for meaningful photodynamic activity. The hyperforin TRPC6/monoamine mechanism is sufficient to explain general antidepressant effects without invoking a photoreceptor mechanism. No definitive in vivo demonstration of hypericin-mediated photic input to circadian or mood circuits has been published
The current consensus is that the hypericin photoreceptor hypothesis is intriguing but unproven, and that hypericum's efficacy in SAD is most parsimoniously explained by the same hyperforin-mediated monoamine mechanism that operates in non-seasonal depression. But the hypothesis persists in the literature because it would elegantly explain why a midsummer-blooming herb so traditionally tied to the solstice would be clinically useful for winter depression.
The Summer Solstice Paradox
Here is the cultural and pharmacological paradox worth contemplating: Hypericum perforatum is the medicinal plant most strongly tied to the summer solstice in European tradition. Its common name derives from St. John the Baptist (feast day June 24, three days after the solstice). It is harvested traditionally on Midsummer's Eve. Medieval herbalists associated it with sun-energy, light, and the protective power of bright midsummer brilliance. It blooms in the longest, sunniest days of the year. Its hypericin is photoactive. Its traditional infused oil requires sun-curing for weeks to develop its full red color and potency.
And yet, its most distinctive modern clinical indication is for winter seasonal affective disorder — the depression of the shortest, darkest days. The plant that captures and concentrates summer light is therapeutically deployed against the depression caused by winter light deprivation.
This is either pure poetic accident, a "doctrine of signatures" coincidence with no mechanistic underpinning, or it reflects something the medieval herbalists intuited about the relationship between the plant and seasonal light biology that modern pharmacology has not yet fully articulated. The hypericin photoreceptor hypothesis, if validated, would be the molecular mechanism behind the poetic appropriateness — the herb literally storing summer light in chemical form (hypericin biosynthesis is itself light-dependent during plant growth) and releasing it as supplementary photic input when administered during the dark winter months.
From a clinician's perspective: even if the photoreceptor hypothesis is not validated, the empirical efficacy is real. The Wheatley 1999 SAD trial and subsequent studies establish that hypericum monotherapy at 900 mg/day produces clinically meaningful improvement in winter SAD symptoms in approximately 50-70% of patients. Whether the mechanism is photo-receptive or purely monoaminergic does not affect the practical clinical question of whether to recommend the herb.
Hypericum vs Bright Light Therapy
The gold-standard non-pharmaceutical treatment for SAD is bright light therapy: typically a 10,000 lux full-spectrum white light box positioned at eye level, used for 30 minutes each morning shortly after waking, throughout the symptomatic winter months. Bright light therapy has been studied since the 1980s and has strong evidence for efficacy in SAD, with response rates in the 60-80% range in well-designed trials.
Direct head-to-head comparisons of hypericum monotherapy versus bright light therapy monotherapy are limited but suggest broadly comparable efficacy. In Wheatley 1999 and subsequent open-label investigations, hypericum 900 mg/day alone produced HAM-D improvement in roughly the same range as 10,000 lux light therapy alone. Both treatments require several weeks to reach full effect (4-6 weeks for hypericum, 2-4 weeks for light therapy).
Practical considerations for choosing between hypericum and light therapy:
- Light therapy advantages: no drug-interaction concerns, no systemic side effects, also useful for circadian rhythm disorders beyond SAD, can be combined with other treatments freely, evidence base is broader and more rigorous
- Light therapy disadvantages: requires daily 30-minute commitment that not all patients can accommodate (early morning schedules, light box must be in proper position, eyes open and facing roughly toward the light), one-time equipment cost of $100-300 for a quality medical-grade light box, must be used consistently throughout the winter season
- Hypericum advantages: simple oral dosing (three capsules daily with meals), can be used by patients who cannot accommodate light therapy schedule, no equipment required, also addresses non-seasonal depressive features, broader mood and anxiolytic effect
- Hypericum disadvantages: drug-interaction burden is significant (see Critical Drug Interactions deep-dive), 4-6 week onset window, photosensitivity risk at higher doses, contraindicated in many common clinical situations
The decision often comes down to patient circumstances: light therapy for patients who can commit to the daily protocol and have no medication interaction concerns versus hypericum for patients who cannot use light therapy, prefer oral medication, or who have non-seasonal mood symptoms alongside their seasonal pattern. Combination treatment is reasonable for patients with severe SAD who can accommodate both modalities.
Combination Protocols: Hypericum + Light Therapy
The Wheatley 1999 trial specifically investigated combination treatment and found that hypericum plus bright light therapy produced numerically greater improvement than hypericum alone (or, by implication, light therapy alone). Subsequent open-label observations have supported the combination approach for patients with moderate-to-severe SAD.
Practical combination protocol (autumn-initiation preferred):
- September-early October: begin hypericum standardized extract 300 mg three times daily (900 mg/day total)
- Mid-October to November: hypericum is now at therapeutic plasma levels; light therapy can be initiated as symptoms begin to emerge or anticipatory based on prior years' patterns. Begin with 10,000 lux for 20-30 minutes within 1 hour of awakening, ideally between 7-9 AM
- December-February: continue both. Adjust light therapy timing if early-morning use disrupts sleep onset the following night. Some patients tolerate brighter (20,000 lux for 10 minutes) or dimmer (5,000 lux for 60 minutes) regimens better than the standard
- March-April: as symptoms remit and daylight increases, light therapy can be discontinued first (typically late March). Hypericum can be continued through April-May before tapering
- May-August: hypericum can be held during the summer months in patients with classic seasonal pattern. Restart in September the following year
Some patients with severe recurrent SAD benefit from year-round hypericum maintenance rather than seasonal start-stop, particularly if they experience residual mood symptoms in spring/summer. The drug-interaction profile of hypericum does not change with seasonal versus continuous dosing — the same precautions apply whenever the herb is in use.
Sub-Syndromal SAD and Mild Winter Mood Symptoms
Full DSM SAD affects perhaps 1-10% of the population in northern latitudes, but a much larger group — perhaps 10-20% of adults in northern climates — experiences sub-syndromal SAD or "winter blues": mild but real winter mood symptoms that do not meet full diagnostic criteria for major depressive episode with seasonal pattern, but that still cause meaningful impairment in mood, energy, motivation, social engagement, and productivity during the December-February months.
Sub-syndromal winter blues is particularly common in:
- Adults living above 40 degrees North or below 40 degrees South (northern U.S., Canada, northern Europe, southern Australia/New Zealand)
- Adults with limited daytime outdoor exposure (office workers, night-shift workers, indoor-occupation workers)
- Adults with darker skin pigmentation in northern latitudes (the same melanin that reduces UVB-mediated Vitamin D synthesis may also affect circadian photic input)
- Women in their reproductive years (the female:male ratio for SAD is approximately 4:1, and the same ratio applies to sub-syndromal presentations)
- Adults with prior history of major depression, currently in remission
For sub-syndromal winter blues that does not meet full SAD criteria, hypericum is a particularly reasonable option because the symptoms are by definition mild-to-moderate and the patient may not require — or may not be willing to consider — pharmaceutical antidepressant therapy. Other reasonable options for mild winter mood symptoms include: Vitamin D3 supplementation (winter levels typically drop in northern climates and the relationship between low Vitamin D and mood is well-documented), morning bright light exposure (either via light box or via outdoor walking shortly after sunrise), and behavioral activation strategies (scheduled pleasant activities, exercise, social engagement).
The combination of moderate-dose hypericum (300-600 mg/day rather than the full 900 mg/day antidepressant dose), 2000-5000 IU/day Vitamin D3, and morning outdoor light exposure or a bright light box represents a reasonable comprehensive naturopathic approach to mild winter mood symptoms that is well-tolerated and avoids pharmaceutical drug-interaction concerns.
Autumn-Initiation Prophylaxis Protocols
The most important practical concept for SAD management with hypericum is autumn initiation for prophylaxis. Because hypericum requires 4-6 weeks to reach full therapeutic effect, waiting until December or January symptoms are already severe is too late — the herb cannot rescue an already-established winter depression as quickly as the patient needs.
For patients with established recurrent SAD, the protocol is to begin hypericum in early-to-mid September, before symptoms have begun, so that therapeutic plasma levels and full receptor effects are present by mid-October when daylight hours have noticeably shortened. This anticipatory dosing is analogous to the bupropion-XL FDA-approved SAD prophylaxis indication that uses the same autumn-initiation principle.
Practical autumn-initiation timeline:
- Late August - early September: review prior years' pattern. If reliable seasonal recurrence with mid-October to mid-March symptomatic period, begin hypericum 300 mg twice daily (600 mg/day)
- Mid-September: increase to 300 mg three times daily (900 mg/day standard dose)
- October-March: continue 900 mg/day. Consider increasing to 1,200 mg/day in late November/December if mood symptoms are emerging despite prophylaxis
- April: as natural daylight returns and symptoms remit, can begin tapering by reducing one dose at a time (e.g., 900 → 600 → 300 → off over 4-6 weeks)
- May-August: hypericum can typically be held during summer if seasonal pattern is reliable
Patients with year-round subclinical mood symptoms (e.g., persistent mild dysthymia that worsens seasonally) may benefit from continuous low-dose hypericum (600 mg/day) year-round rather than the seasonal stop-start. The decision should be individualized based on symptom pattern, drug-interaction concerns, and patient preference.
Menopausal Mood Symptoms
St. John's Wort has accumulated meaningful evidence for the mood symptoms of perimenopause and menopause — the irritability, mood lability, anxiety, depressed mood, and emotional reactivity that affect a substantial fraction of women through the menopausal transition. Several randomized trials have demonstrated significant improvement in menopausal mood measures with hypericum 900 mg/day over 8-12 weeks, with response rates comparable to those seen in non-menopausal depression trials.
The combination of hypericum with black cohosh (Actaea racemosa, formerly Cimicifuga racemosa) has been particularly well studied for menopausal symptoms, with the combination addressing both mood (hypericum) and vasomotor symptoms like hot flashes (black cohosh) more effectively than either herb alone. The Uebelhack et al. 2006 trial demonstrated that hypericum-plus-black-cohosh produced significantly greater improvement in both menopausal-specific mood symptoms and overall depression than placebo over 16 weeks in 301 women.
Practical considerations for menopausal mood use:
- Hypericum dose for menopausal mood is the standard 900 mg/day (300 mg three times daily of standardized extract)
- Black cohosh is typically dosed at 40 mg/day of standardized extract (Remifemin or equivalent)
- The combination is taken for 8-16 weeks and re-evaluated. Many women continue indefinitely through the perimenopausal years
- Drug-interaction concerns are the same as for non-menopausal hypericum use — menopausal women are often on multiple medications (cholesterol, blood pressure, osteoporosis, sometimes thyroid) and the interaction profile must be carefully reviewed before initiation
- Hypericum is generally avoided in women taking black cohosh for vasomotor symptoms who are simultaneously on hormone replacement therapy with estrogen + progesterone, because hypericum can reduce the effectiveness of the HRT
Premenstrual Syndrome (PMS) Applications
Several small clinical trials and one larger randomized investigation have examined hypericum for the mood symptoms of premenstrual syndrome (PMS) and the more severe premenstrual dysphoric disorder (PMDD). The rationale: PMS/PMDD mood symptoms are believed to reflect cyclical serotonergic dysregulation in response to ovarian hormone fluctuations, and SSRIs (used either continuously or in the luteal phase only) are first-line pharmaceutical treatment for PMDD. Hypericum's monoamine reuptake inhibition could plausibly produce similar effects through similar mechanisms.
The available trials suggest hypericum produces clinically meaningful improvement in PMS mood symptoms (irritability, mood swings, depressed mood, anxiety) when dosed continuously at 900 mg/day across multiple menstrual cycles. The effect is generally smaller than in major depression trials, possibly reflecting the inherently cyclical nature of PMS symptoms or the smaller effect size needed for clinically meaningful PMS improvement.
Practical considerations for PMS use:
- Standard dose 900 mg/day of standardized extract
- Continuous dosing (not luteal-phase only) for at least 3-4 menstrual cycles before assessing response
- The drug-interaction with hormonal contraception is critical — women on oral contraceptive pills, patches, rings, or implants cannot safely use hypericum without alternative contraception, as documented breakthrough bleeding and unintended pregnancies have occurred
- The combination of hypericum and pyridoxine (Vitamin B6, 50-100 mg/day) and magnesium (200-400 mg/day) is a well-tolerated naturopathic protocol for PMS mood symptoms
Key Research Papers
- Wheatley D (1999). Hypericum in seasonal affective disorder (SAD). Current Medical Research and Opinion, 15(1):33-7. The pivotal SAD trial. — PubMed: Wheatley 1999 SAD
- Martinez B, Kasper S, Ruhrmann S, Möller HJ (1994). Hypericum in the treatment of seasonal affective disorders. Journal of Geriatric Psychiatry and Neurology, 7 Suppl 1:S29-33. Early SAD investigation. — PubMed: Martinez SAD 1994
- Kasper S (1997). Treatment of seasonal affective disorder (SAD) with hypericum extract. Pharmacopsychiatry, 30 Suppl 2:89-93. Pharmacopsychiatry SAD review. — PubMed: Kasper SAD 1997
- Wirz-Justice A, Bucheli C, Graw P, Kielholz P, Fisch HU, Woggon B (1986). Light treatment of seasonal affective disorder in Switzerland. Acta Psychiatrica Scandinavica, 74(2):193-204. The foundational European light therapy trial that established the SAD treatment framework into which hypericum was later added. — PubMed: Wirz-Justice 1986 light
- Lam RW et al. (2006). The Can-SAD study: a randomized controlled trial of the effectiveness of light therapy and fluoxetine in patients with winter seasonal affective disorder. American Journal of Psychiatry, 163(5):805-12. The pivotal head-to-head of light therapy vs SSRI in SAD that establishes the comparator framework. — PubMed: Can-SAD 2006
- Modell JG, Rosenthal NE, Harriett AE, Krishen A, Asgharian A, Foster VJ, Metz A, Rockett CB, Wightman DS (2005). Seasonal affective disorder and its prevention by anticipatory treatment with bupropion XL. Biological Psychiatry, 58(8):658-67. The bupropion-XL FDA-approved SAD prophylaxis trial that establishes the autumn-initiation framework. — PubMed: Bupropion SAD prophylaxis
- Uebelhack R, Blohmer JU, Graubaum HJ, Busch R, Gruenwald J, Wernecke KD (2006). Black cohosh and St. John's wort for climacteric complaints: a randomized trial. Obstetrics & Gynecology, 107(2 Pt 1):247-55. Hypericum + black cohosh for menopausal mood. — PubMed: Uebelhack menopausal
- Grube B, Walper A, Wheatley D (1999). St. John's Wort extract: efficacy for menopausal symptoms of psychological origin. Advances in Therapy, 16(4):177-86. The original menopausal-mood hypericum trial. — PubMed: Grube menopausal 1999
- Stevinson C, Ernst E (2000). A pilot study of Hypericum perforatum for the treatment of premenstrual syndrome. BJOG, 107(7):870-6. PMS pilot study. — PubMed: Stevinson PMS 2000
- Canning S et al. (2010). The efficacy of Hypericum perforatum (St John's Wort) for the treatment of premenstrual syndrome: a randomized, double-blind, placebo-controlled trial. CNS Drugs, 24(3):207-25. Larger randomized PMS trial. — PubMed: Canning PMS 2010
- Wirz-Justice A (2003). Chronobiological strategies for unmet needs in the treatment of depression. Medicographia, 25:131-138. The conceptual framework for circadian/photic therapies in SAD and depression. — PubMed: Wirz-Justice chronobiology
- Rosenthal NE et al. (1984). Seasonal affective disorder. A description of the syndrome and preliminary findings with light therapy. Archives of General Psychiatry, 41(1):72-80. The original Rosenthal description of SAD syndrome and light therapy. — PubMed: Rosenthal 1984 original SAD
PubMed Topic Searches
- PubMed: Hypericum SAD
- PubMed: Hypericin photosensitizer mechanism
- PubMed: Hypericum menopausal
- PubMed: Hypericum PMS
- PubMed: Bright light therapy SAD
- PubMed: Hypericum anxiety
Connections
- St. John's Wort Benefits Hub
- St. John's Wort Overview
- St. John's Wort for Depression
- Critical Drug Interactions
- Depression
- Anxiety
- Vitamin D3 (Winter Deficiency)
- Black Cohosh (Menopausal Combo)
- Saffron
- Rhodiola Rosea
- Ashwagandha
- Lemon Balm
- Lavender
- Stress Management
- Fatigue
- All Herbs