St. John's Wort — Critical Drug Interactions
⚠ CRITICAL SAFETY WARNING
St. John's Wort has the most extensive and clinically significant drug-interaction profile of any commonly used medicinal herb. Documented cases include unintended pregnancies in women taking oral contraceptives, acute organ rejection in transplant patients, HIV antiretroviral treatment failure with viral resistance, warfarin anticoagulation failure with thrombotic events, and life-threatening serotonin syndrome from combination with SSRIs. The FDA, European Medicines Agency, Health Canada, the UK Medicines and Healthcare products Regulatory Agency, and Australia's Therapeutic Goods Administration have all issued formal regulatory warnings. Before starting St. John's Wort, review every prescription, over-the-counter, and herbal supplement you take with a qualified pharmacist or physician. Before starting any new medication while on St. John's Wort, disclose its use to the prescriber. Discontinue at least 5 days before any planned surgery.
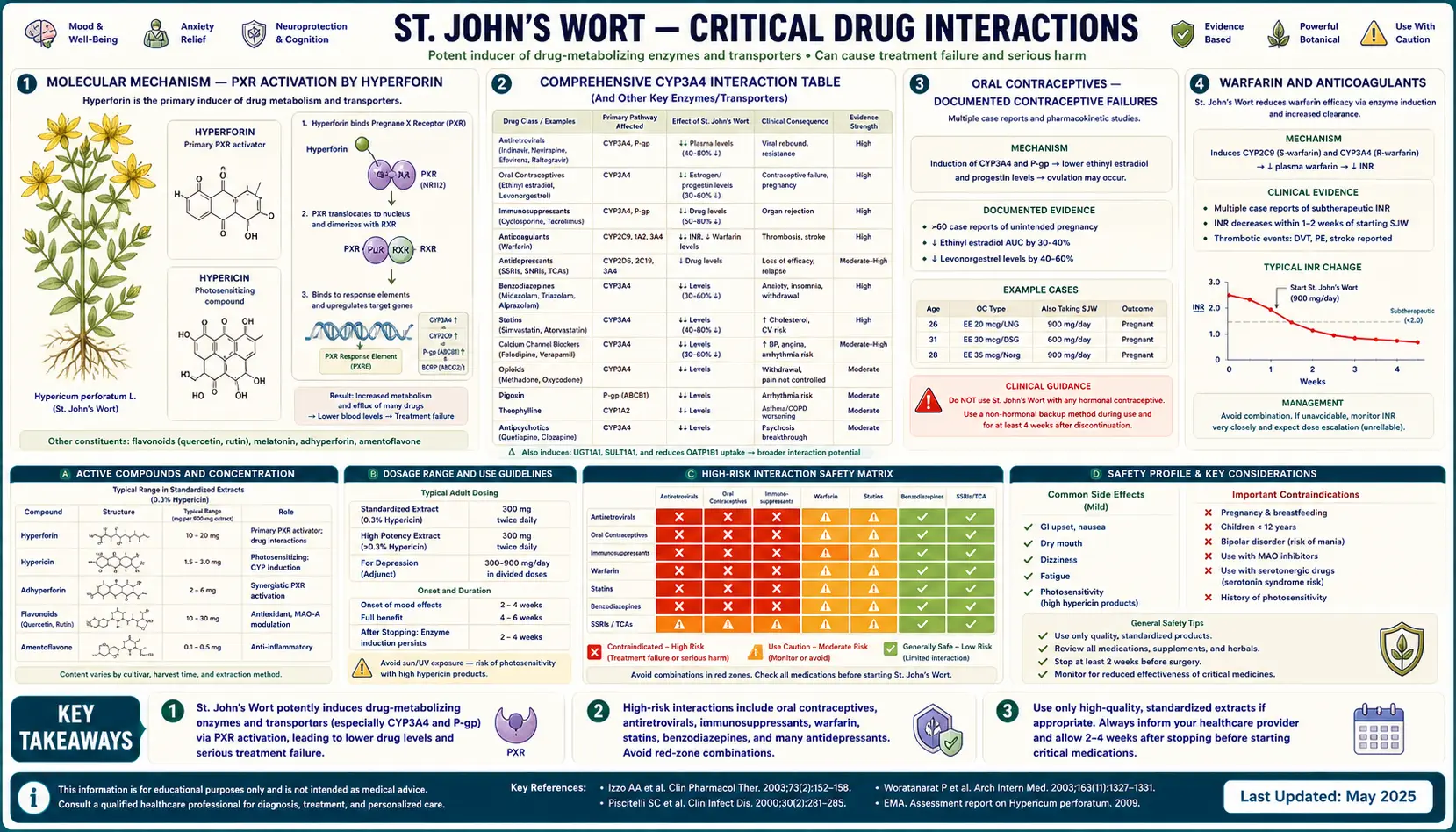
The same hyperforin molecule that drives St. John's Wort's antidepressant efficacy also produces its catastrophic drug-interaction profile. Hyperforin is a potent agonist of the pregnane X receptor (PXR), which is the master transcription factor controlling expression of the CYP3A4, CYP1A2, CYP2C9, and CYP2C19 cytochrome P450 enzymes and the P-glycoprotein drug efflux transporter. PXR activation by hyperforin upregulates these drug-metabolizing systems by 50-300% over baseline, dramatically accelerating the clearance of any drug that is a substrate. More than half of all prescription drugs in clinical use are metabolized by CYP3A4 alone — including oral contraceptives, anticoagulants, immunosuppressants, HIV antiretrovirals, cardiac drugs, chemotherapy, statins, anticonvulsants, and many psychiatric medications. The clinical consequences range from contraceptive failure (with documented unintended pregnancies) to organ-rejection cases in transplant patients to antiretroviral treatment failure with viral resistance to anticoagulation failure with thrombotic events. Separately, the herb's pharmacodynamic interaction with serotonergic drugs (SSRIs, SNRIs, triptans, tramadol, MAOIs) can produce potentially fatal serotonin syndrome. This deep-dive walks through the molecular mechanism, the comprehensive interaction tables, the FDA and international regulatory warning history, and the practical clinical-decision framework for any patient considering or already taking St. John's Wort.
Table of Contents
- Molecular Mechanism — PXR Activation by Hyperforin
- Comprehensive CYP3A4 Interaction Table
- Oral Contraceptives — Documented Contraceptive Failures
- Warfarin and Anticoagulants
- Immunosuppressants — Organ Rejection Cases
- HIV Antiretrovirals — Absolute Contraindication
- Serotonin Syndrome with SSRIs/SNRIs/Triptans
- Cardiac Drugs (Digoxin, Statins, Antiarrhythmics)
- Chemotherapy and Targeted Cancer Therapies
- Anticonvulsants and Psychiatric Medications
- FDA, EMA, and Health Canada Warning History
- Surgical and Anesthetic Considerations
- Clinical Decision Framework
- Key Research Papers
- Connections
- Featured Videos
Molecular Mechanism — PXR Activation by Hyperforin
The pharmacological root of St. John's Wort's drug-interaction profile is the activation of the pregnane X receptor (PXR) by hyperforin, the herb's principal antidepressant constituent. PXR (also known as NR1I2 or the steroid and xenobiotic receptor SXR) is a nuclear hormone receptor that functions as the master transcription factor controlling expression of the body's xenobiotic metabolism and elimination machinery.
When PXR is activated by an agonist (endogenous bile acids, hyperforin, the antibiotic rifampin, the antifungal clotrimazole, and various other xenobiotics), it translocates to the nucleus, heterodimerizes with the retinoid X receptor (RXR), and binds to PXR response elements (DR3 motifs) in the promoter regions of target genes including:
- CYP3A4 — the cytochrome P450 enzyme responsible for the metabolism of approximately 50% of all prescription drugs. CYP3A4 induction by hyperforin is the single most important driver of the herb's drug-interaction profile
- CYP1A2 — metabolizes caffeine, theophylline, clozapine, olanzapine, mirtazapine, and certain other drugs. Hyperforin induces CYP1A2 modestly
- CYP2C9 — metabolizes warfarin (S-enantiomer), phenytoin, several NSAIDs, and other drugs. Hyperforin induces CYP2C9 partially
- CYP2C19 — metabolizes omeprazole, clopidogrel, certain anticonvulsants, voriconazole. Hyperforin has modest induction effect
- P-glycoprotein (P-gp, MDR1, ABCB1) — an ATP-driven drug efflux transporter located in intestinal epithelium (limiting drug absorption), hepatocytes (promoting drug elimination into bile), and the blood-brain barrier (limiting CNS drug penetration). P-gp induction by hyperforin reduces oral bioavailability and CNS penetration of P-gp substrates
- UGT (UDP-glucuronosyltransferase) enzymes — Phase II conjugation enzymes that glucuronidate drugs for elimination. UGT1A1 and UGT2B7 are induced by hyperforin
The induction kinetics matter clinically:
- CYP3A4 induction begins within 3-7 days of starting hypericum at therapeutic dosing
- Maximum induction is reached at approximately 14 days, with CYP3A4 activity increased by 100-300% over baseline (i.e., enzyme activity 2-4 times normal)
- P-glycoprotein induction follows a similar timeline
- After hypericum discontinuation, induction takes 2-3 weeks to dissipate as the induced enzyme protein is degraded
- The induction is dose-dependent — doses of hyperforin above approximately 1 mg/day (achieved with standardized extracts containing 1-5% hyperforin at 300-900 mg/day total dose) reliably produce clinically significant CYP3A4 induction. Lower-hyperforin extracts (like ZE 117) produce less induction
The clinical consequence: any drug whose effective plasma concentration depends on CYP3A4, CYP1A2, CYP2C9, CYP2C19, P-gp, or UGT metabolism will have reduced plasma levels and reduced clinical effect when hypericum is co-administered. The magnitude of the interaction varies by drug (some have plasma level reductions of 25%, others of 75% or more), but the direction is consistent: hypericum reduces drug exposure.
Separately, hyperforin's monoamine reuptake inhibition (the mechanism behind its antidepressant effect) creates a pharmacodynamic interaction with other serotonergic, noradrenergic, and dopaminergic drugs — the effects of those drugs are additive or synergistic with hypericum's. The most clinically dangerous example is serotonin syndrome with SSRI/SNRI/triptan/MAOI combinations.
Comprehensive CYP3A4 Interaction Table
The following table summarizes the most clinically significant CYP3A4-mediated and pharmacodynamic interactions with St. John's Wort. Categories of severity:
- ABSOLUTELY CONTRAINDICATED — co-administration must not occur under any circumstance
- STRONGLY DISCOURAGED — co-administration only under specialist supervision with intensive monitoring
- SIGNIFICANT INTERACTION — dose adjustment and monitoring required; many clinicians avoid co-administration
- MODERATE INTERACTION — monitor for reduced effect or breakthrough symptoms; dose adjustment may be needed
Hormonal Contraceptives
- Combined oral contraceptive pills (ethinyl estradiol + progestin: e.g., Yasmin, Ortho Tri-Cyclen, Loestrin) — SIGNIFICANT INTERACTION. Reduced estrogen and progestin levels with documented contraceptive failure including unintended pregnancies. Use additional non-hormonal contraception or different birth control method during and for 2 weeks after hypericum use
- Progestin-only pills (norethindrone "mini-pill") — SIGNIFICANT INTERACTION, same management as combined pills
- Contraceptive patch (Xulane, Twirla) — SIGNIFICANT INTERACTION, same management
- Vaginal contraceptive ring (NuvaRing, Annovera) — SIGNIFICANT INTERACTION, same management
- Etonogestrel implant (Nexplanon) — SIGNIFICANT INTERACTION; the implant's contraceptive efficacy may be reduced
- Levonorgestrel emergency contraception (Plan B, ella) — reduced efficacy; consider copper IUD insertion or other emergency contraception strategy if hypericum has been used recently
- Levonorgestrel IUD (Mirena, Liletta, Kyleena) — LOWER INTERACTION RISK because local hormone release does not depend on systemic CYP3A4 metabolism, but breakthrough bleeding may occur. Generally considered acceptable with hypericum
- Copper IUD (Paragard) — NO INTERACTION; preferred non-hormonal option for women requiring contraception during hypericum use
Anticoagulants and Antiplatelets
- Warfarin (Coumadin) — SIGNIFICANT INTERACTION. Reduced anticoagulant effect, with documented thromboembolic events including stroke and pulmonary embolism. INR can drop by 30-50%. If co-administration is unavoidable, INR monitoring every 3-7 days with warfarin dose adjustment is required
- Direct oral anticoagulants (DOACs): apixaban (Eliquis), rivaroxaban (Xarelto), edoxaban (Savaysa) are CYP3A4 and P-gp substrates — SIGNIFICANT INTERACTION. Dabigatran (Pradaxa) is primarily P-gp substrate — MODERATE INTERACTION. All DOACs may have reduced anticoagulant effect; co-administration generally discouraged
- Clopidogrel (Plavix) — MODERATE INTERACTION. Clopidogrel is a prodrug requiring CYP2C19 activation; the net effect of hypericum on active metabolite levels is complex and may either reduce or paradoxically increase antiplatelet effect. Monitor clinically
Immunosuppressants (Organ Transplant)
- Cyclosporine — ABSOLUTELY CONTRAINDICATED. Cyclosporine levels drop by 50-70% with documented cases of acute kidney, liver, and heart allograft rejection
- Tacrolimus (Prograf) — ABSOLUTELY CONTRAINDICATED. Tacrolimus levels drop dramatically; rejection cases reported
- Sirolimus (Rapamune) — ABSOLUTELY CONTRAINDICATED. Same mechanism, same rejection risk
- Mycophenolate (CellCept, Myfortic) — SIGNIFICANT INTERACTION via UGT induction
- Corticosteroids (prednisone, methylprednisolone, dexamethasone) — MODERATE INTERACTION; reduced efficacy possible but generally manageable
HIV Antiretrovirals
- Protease inhibitors (indinavir, ritonavir, atazanavir, darunavir, lopinavir, saquinavir, etc.) — ABSOLUTELY CONTRAINDICATED. Plasma levels reduced by 50-80% with treatment failure and emergence of viral resistance. The Piscitelli 2000 Lancet study of indinavir + hypericum showing 57% reduction in indinavir AUC was the trigger for FDA's first formal hypericum warning
- Non-nucleoside reverse transcriptase inhibitors (NNRTIs): efavirenz (Sustiva), nevirapine (Viramune), etravirine (Intelence), rilpivirine (Edurant) — ABSOLUTELY CONTRAINDICATED. Same mechanism, same risk
- Integrase inhibitors: dolutegravir (Tivicay), elvitegravir, raltegravir (Isentress), bictegravir — SIGNIFICANT INTERACTION; co-administration not recommended
- Pharmacokinetic boosters: cobicistat (Tybost), ritonavir as boosting agent — ABSOLUTELY CONTRAINDICATED
- Nucleoside reverse transcriptase inhibitors (tenofovir, emtricitabine, lamivudine, abacavir, zidovudine) — LOWER INTERACTION RISK because these are not primarily CYP3A4 metabolized
Cardiovascular Medications
- Digoxin — SIGNIFICANT INTERACTION via P-gp induction. Reduced digoxin levels with risk of loss of rate control or heart failure decompensation
- Statins: simvastatin (Zocor), atorvastatin (Lipitor), lovastatin — MODERATE INTERACTION via CYP3A4. Pravastatin, rosuvastatin, fluvastatin, pitavastatin have lower CYP3A4 dependence and lower interaction risk
- Calcium channel blockers: amlodipine, diltiazem, verapamil, nifedipine — MODERATE INTERACTION via CYP3A4. Reduced antihypertensive effect possible
- Beta-blockers: metoprolol, propranolol — LOWER INTERACTION RISK
- Antiarrhythmics: amiodarone, quinidine, dronedarone — SIGNIFICANT INTERACTION via CYP3A4
- Ivabradine (Corlanor) — SIGNIFICANT INTERACTION via CYP3A4
Psychiatric Medications (Pharmacodynamic Serotonin Syndrome Risk)
- SSRIs: fluoxetine (Prozac), sertraline (Zoloft), paroxetine (Paxil), citalopram (Celexa), escitalopram (Lexapro), fluvoxamine (Luvox) — STRONGLY DISCOURAGED. Serotonin syndrome risk (potentially fatal hyperthermic crisis with agitation, confusion, neuromuscular hyperactivity, autonomic instability). Combination should not be initiated; if a patient is on SSRI and considers hypericum, the SSRI must be discontinued and washed out first
- SNRIs: venlafaxine (Effexor), duloxetine (Cymbalta), desvenlafaxine (Pristiq), levomilnacipran (Fetzima) — STRONGLY DISCOURAGED. Same serotonin syndrome risk
- MAO Inhibitors: phenelzine (Nardil), tranylcypromine (Parnate), isocarboxazid (Marplan), selegiline (Eldepryl, Emsam) — ABSOLUTELY CONTRAINDICATED. Highest serotonin syndrome and hypertensive crisis risk
- Tricyclic antidepressants: amitriptyline, nortriptyline, imipramine, clomipramine — STRONGLY DISCOURAGED. Serotonin syndrome risk plus tricyclic levels may be reduced via CYP induction
- Triptans: sumatriptan (Imitrex), rizatriptan (Maxalt), zolmitriptan (Zomig), eletriptan (Relpax), etc. — SIGNIFICANT INTERACTION. Serotonin syndrome risk; FDA black-box-style warning
- Tramadol — SIGNIFICANT INTERACTION. Both serotonin syndrome risk and reduced tramadol active metabolite levels
- Dextromethorphan (in cough syrups) — SIGNIFICANT INTERACTION. Serotonin syndrome reports
- Lithium — MODERATE INTERACTION. Possible serotonergic potentiation
- Bupropion (Wellbutrin) — MODERATE INTERACTION via CYP2B6. Reduced bupropion levels possible
- Antipsychotics: olanzapine, clozapine, quetiapine, aripiprazole, risperidone — SIGNIFICANT INTERACTION via CYP3A4 and/or CYP1A2. Reduced antipsychotic levels with risk of psychotic decompensation
- Benzodiazepines: alprazolam (Xanax), midazolam (Versed), triazolam — SIGNIFICANT INTERACTION via CYP3A4. Reduced sedative effect. Diazepam, lorazepam, oxazepam have lower interaction risk
Chemotherapy and Targeted Cancer Therapies
- Tyrosine kinase inhibitors: imatinib (Gleevec), dasatinib, nilotinib, erlotinib, gefitinib, sorafenib, sunitinib — SIGNIFICANT INTERACTION via CYP3A4. Reduced anticancer drug levels
- Irinotecan — SIGNIFICANT INTERACTION. Reduced active metabolite SN-38 levels
- Docetaxel, paclitaxel — SIGNIFICANT INTERACTION
- Etoposide, vinca alkaloids — SIGNIFICANT INTERACTION
- Tamoxifen — MODERATE INTERACTION. Tamoxifen requires CYP2D6 activation; the net effect on the active endoxifen metabolite is complex
- General principle: any patient on active chemotherapy or targeted cancer therapy must avoid hypericum unless specifically cleared by their oncologist
Anticonvulsants
- Carbamazepine (Tegretol) — SIGNIFICANT INTERACTION via mutual CYP3A4 induction (both drugs induce CYP3A4). Carbamazepine levels may decrease with seizure breakthrough
- Phenytoin (Dilantin) — SIGNIFICANT INTERACTION via CYP3A4 and CYP2C9 induction
- Phenobarbital — SIGNIFICANT INTERACTION (both drugs induce CYP3A4)
- Lamotrigine (Lamictal) — MODERATE INTERACTION via UGT induction
- Valproate — MODERATE INTERACTION
- Levetiracetam (Keppra), topiramate, gabapentin, pregabalin — LOWER INTERACTION RISK (not primarily CYP metabolized)
Other Important Interactions
- Methadone — SIGNIFICANT INTERACTION via CYP3A4 and CYP2B6. Reduced methadone levels with risk of withdrawal and treatment failure in opioid use disorder management or pain management
- Oxycodone, fentanyl — SIGNIFICANT INTERACTION via CYP3A4. Reduced analgesic effect
- Sildenafil (Viagra), tadalafil (Cialis), vardenafil — MODERATE INTERACTION via CYP3A4
- Theophylline — SIGNIFICANT INTERACTION via CYP1A2
- Cyclophosphamide — SIGNIFICANT INTERACTION (complex effects on active metabolite formation)
- Voriconazole — SIGNIFICANT INTERACTION via CYP3A4 and CYP2C19
- Omeprazole, lansoprazole, esomeprazole, pantoprazole — MODERATE INTERACTION via CYP2C19; reduced acid suppression possible
- Atorvastatin/simvastatin + ezetimibe — the statin component has CYP3A4 interaction as noted above
- Caffeine — MODERATE INTERACTION via CYP1A2 induction; caffeine clearance accelerated, may need higher doses for same effect
Oral Contraceptives — Documented Contraceptive Failures
The hypericum-contraceptive interaction is among the most consequential because the failure mode is a permanent life-altering event (unintended pregnancy) that often occurs without warning — the woman has no way to know contraceptive efficacy is reduced until breakthrough bleeding occurs or, worse, until pregnancy is confirmed.
The mechanism: combined oral contraceptive pills contain ethinyl estradiol (or in newer formulations, estetrol or estradiol valerate) plus a progestin (levonorgestrel, norethindrone, drospirenone, etc.). Both estrogen and progestin components undergo CYP3A4 metabolism in the gut wall and liver, and both undergo intestinal P-glycoprotein efflux. Hyperforin's induction of CYP3A4 and P-gp accelerates the metabolism and reduces the absorption of both components.
The clinical consequences:
- Reduced peak and trough estrogen and progestin plasma levels (typically 30-50% reduction)
- Loss of ovulation suppression (the principal contraceptive mechanism)
- Breakthrough bleeding and spotting (often the first clinical sign)
- Contraceptive failure with unintended pregnancy
The literature includes multiple case reports and case series of pregnancies in women who became pregnant despite consistent oral contraceptive use after starting hypericum. The German pharmacovigilance database accumulated several documented cases in the late 1990s and early 2000s, which contributed to European Medicines Agency safety communications. The UK Medicines and Healthcare products Regulatory Agency issued a formal warning in 2000. The U.S. FDA followed in 2000 with its first formal hypericum-interaction advisory.
Practical guidance for women on hormonal contraception who are considering hypericum:
- If pregnancy prevention is essential, do not use hypericum with combined oral contraceptive pills, progestin-only pills, the patch, the ring, or the etonogestrel implant. Use an alternative depression treatment
- If hypericum is essential and the woman is on hormonal contraception, switch to a non-hormonal method (copper IUD) or a method with lower interaction risk (levonorgestrel IUD) before starting hypericum, and continue the alternative method for at least 2 weeks after stopping hypericum
- For women currently on the combination who cannot or will not change either treatment, use barrier contraception (condoms) consistently as backup. Counseling about the increased pregnancy risk and the option of post-coital emergency contraception (with awareness that even emergency contraception efficacy may be reduced)
- The 2-week washout period: CYP3A4 induction takes approximately 2-3 weeks to dissipate after hypericum discontinuation. Contraceptive efficacy may not return to normal for several weeks after stopping hypericum, even if the contraceptive method has not been changed
Warfarin and Anticoagulants
Warfarin is a vitamin-K-antagonist anticoagulant used for stroke prevention in atrial fibrillation, treatment of venous thromboembolism (deep vein thrombosis and pulmonary embolism), and prevention of clot formation in mechanical heart valves. Therapeutic warfarin dosing requires a delicate balance between adequate anticoagulation (typically targeting an INR of 2.0-3.0, or 2.5-3.5 for mechanical valves) and excessive anticoagulation (with bleeding risk).
Hypericum interaction with warfarin:
- Mechanism: warfarin is metabolized primarily by CYP2C9 (S-warfarin enantiomer, the more potent form) and CYP1A2/CYP3A4 (R-warfarin enantiomer). Hyperforin induces CYP2C9, CYP1A2, and CYP3A4, accelerating warfarin clearance
- Magnitude: INR typically drops by 30-50% within 1-2 weeks of starting hypericum at therapeutic dosing
- Clinical consequences: documented cases of thromboembolic events (ischemic stroke, recurrent DVT/PE, mechanical valve thrombosis) in patients who became sub-therapeutic after starting hypericum
- Reverse effect after hypericum discontinuation: when hypericum is stopped, CYP induction dissipates over 2-3 weeks and warfarin clearance returns to baseline. The INR may rise unpredictably during this transition, with bleeding risk if the warfarin dose was increased to compensate for the induction
Management:
- Avoid hypericum-warfarin co-administration when possible
- If unavoidable, monitor INR weekly during hypericum initiation and dose-titration period, and again weekly during hypericum discontinuation and washout. Adjust warfarin dose to maintain target INR throughout
- Communicate clearly with the patient about the increased monitoring requirement and the importance of not stopping hypericum abruptly without notifying the anticoagulation clinic
Direct oral anticoagulants (DOACs):
- Apixaban, rivaroxaban, edoxaban are CYP3A4 and P-glycoprotein substrates — substantial interaction with hypericum expected, with reduced anticoagulant effect
- Dabigatran is primarily P-glycoprotein substrate (minimal CYP metabolism) — modest interaction with hypericum, but still potentially clinically significant
- Unlike warfarin, DOACs do not have a routine monitoring parameter (no INR equivalent), so detecting reduced anticoagulant effect is difficult clinically. Co-administration of hypericum with DOACs is generally discouraged
Immunosuppressants — Organ Rejection Cases
Solid organ transplant recipients (kidney, liver, heart, lung, pancreas, small bowel) require lifelong immunosuppression to prevent allograft rejection. Standard regimens typically include a calcineurin inhibitor (cyclosporine or tacrolimus), often combined with mycophenolate and corticosteroids, with maintenance dosing carefully titrated based on therapeutic drug monitoring to keep trough levels within narrow target ranges.
The hypericum-immunosuppressant interaction is among the most catastrophic:
- Cyclosporine: hyperforin induction of CYP3A4 and P-gp reduces cyclosporine trough levels by 50-70%. Documented case series include acute kidney transplant rejection, liver transplant rejection requiring re-transplantation, and heart transplant rejection with hemodynamic compromise
- Tacrolimus: similar magnitude of reduction in trough levels with comparable rejection risk. Trough levels can drop from therapeutic 8-12 ng/mL to subtherapeutic 2-4 ng/mL within 1-2 weeks of hypericum initiation
- Sirolimus: same mechanism, same rejection risk
- Mycophenolate: less affected by CYP induction but UGT induction by hyperforin can modestly reduce active mycophenolic acid levels
- Reverse effect: when hypericum is discontinued, CYP induction dissipates over 2-3 weeks and calcineurin inhibitor levels rise. The post-hypericum-discontinuation period carries risk of supra-therapeutic levels with nephrotoxicity, neurotoxicity, or other immunosuppressant-specific toxicity
The clinical recommendation is unambiguous: hypericum is ABSOLUTELY CONTRAINDICATED in solid organ transplant recipients. The interaction has caused documented allograft loss and is not manageable with even intensive therapeutic drug monitoring. Patients with depression after transplantation should use conventional pharmaceutical antidepressants with known interaction profiles (avoiding strong CYP3A4 substrates or inhibitors) or non-pharmaceutical interventions (CBT, exercise, light therapy if seasonal).
Stem cell transplant and hematopoietic cell transplant recipients on immunosuppression for graft-versus-host disease prophylaxis or treatment face the same restrictions.
Patients on biologic immunomodulators (TNF inhibitors, JAK inhibitors, IL-17 inhibitors, IL-23 inhibitors) for autoimmune disease generally have lower interaction risk because most biologics are not CYP-metabolized, though specific interactions should be reviewed for each agent.
HIV Antiretrovirals — Absolute Contraindication
The hypericum-HIV antiretroviral interaction was the trigger for the first formal FDA warning about hypericum in February 2000. The seminal study was Piscitelli et al. (Lancet, February 2000), which examined the effect of 14 days of hypericum administration on indinavir pharmacokinetics in healthy volunteers. The results were dramatic:
- Indinavir AUC (area under the plasma concentration curve) was reduced by 57%
- Indinavir trough plasma concentration was reduced by 81%
- The magnitude of interaction was more than sufficient to push indinavir levels below the minimum effective concentration for HIV suppression
The clinical consequence: patients on indinavir who add hypericum will experience loss of viral suppression, viral load rebound, and emergence of HIV protease resistance mutations that may compromise future treatment options. The same magnitude of interaction has been documented with other protease inhibitors and with non-nucleoside reverse transcriptase inhibitors (NNRTIs) including efavirenz and nevirapine.
Integrase strand transfer inhibitors (INSTIs) such as dolutegravir, elvitegravir/cobicistat, raltegravir, and bictegravir are increasingly the first-line antiretroviral class, but they are also significantly affected by hypericum (dolutegravir and bictegravir are UGT substrates that may be affected; cobicistat-boosted regimens lose pharmacokinetic boosting).
The FDA, Health Canada, and European Medicines Agency all maintain warnings that hypericum is contraindicated for use with HIV antiretroviral medications. This applies to all currently marketed antiretroviral classes:
- Protease inhibitors — ABSOLUTELY CONTRAINDICATED
- NNRTIs — ABSOLUTELY CONTRAINDICATED
- INSTIs — CONTRAINDICATED
- Pharmacokinetic boosters (cobicistat, ritonavir as booster) — ABSOLUTELY CONTRAINDICATED
- Long-acting injectables (cabotegravir, rilpivirine) — CONTRAINDICATED
- Nucleoside RT inhibitors (tenofovir, emtricitabine, lamivudine, abacavir) — lower interaction risk but combination regimens always include a third agent from one of the contraindicated classes
HIV-positive patients with depression should be referred to HIV specialty care for selection of an antidepressant compatible with their antiretroviral regimen. Common options include bupropion, mirtazapine, or specific SSRIs known to have lower CYP3A4 interaction (e.g., citalopram or escitalopram, with caution for QT prolongation when combined with certain antiretrovirals).
Serotonin Syndrome with SSRIs/SNRIs/Triptans
Beyond the pharmacokinetic CYP-induction interactions discussed above, hypericum produces a clinically critical pharmacodynamic interaction with other serotonergic drugs. The mechanism: hyperforin's inhibition of serotonin reuptake (via the TRPC6/sodium-gradient mechanism) adds to the serotonergic effect of pharmaceutical SSRIs and SNRIs. When combined with other drugs that increase serotonergic signaling (triptans, tramadol, dextromethorphan, MAO inhibitors), the additive effect can produce serotonin syndrome — a potentially fatal hyperthermic crisis.
The clinical features of serotonin syndrome are classified into the Hunter Criteria (the modern diagnostic standard) and include:
- Mental status changes: agitation, confusion, restlessness, anxiety, hypomanic features
- Autonomic hyperactivity: tachycardia, hypertension (or sometimes hypotension), hyperthermia, diaphoresis (sweating), mydriasis (dilated pupils), tachypnea
- Neuromuscular hyperactivity: clonus (particularly inducible clonus in the lower extremities, or spontaneous clonus in severe cases), hyperreflexia, tremor, muscle rigidity, ocular clonus
- Severe cases: hyperthermia greater than 41 degrees C (106 degrees F), rhabdomyolysis, disseminated intravascular coagulation, seizures, multi-organ failure, death
Onset is typically within hours to days of adding a second serotonergic agent. The severity ranges from mild (agitation, mild tachycardia, modest tremor) to life-threatening (severe hyperthermia, rigidity, seizures).
Drugs that produce serotonin syndrome risk in combination with hypericum:
- All SSRIs and SNRIs
- MAO inhibitors (highest risk; combination is absolutely contraindicated)
- Tricyclic antidepressants (particularly clomipramine which is highly serotonergic)
- Triptans (sumatriptan, rizatriptan, etc.)
- Tramadol
- Tapentadol
- Meperidine (Demerol)
- Dextromethorphan (in cough syrups; both prescription and OTC formulations)
- Linezolid (a weak MAOI antibiotic)
- Methylene blue (a weak MAOI used in certain medical/surgical contexts)
- St. John's Wort + 5-HTP, L-tryptophan supplements, or SAM-e supplements
Management of suspected serotonin syndrome:
- Discontinue all serotonergic agents immediately
- Supportive care: IV fluids, cooling for hyperthermia, benzodiazepines (lorazepam) for agitation and tremor
- Severe cases: ICU admission, cyproheptadine (a serotonin 5-HT2A antagonist that may be used as antidote), aggressive cooling, intubation if needed
- Most cases resolve within 24-72 hours of stopping serotonergic agents
Prevention is far better than treatment: do not combine hypericum with any other serotonergic medication. Transitions between hypericum and pharmaceutical SSRIs should include a washout period of at least 2 weeks in either direction (longer for fluoxetine which has a very long half-life). For more on the cluster of related conditions, see our Depression page.
Cardiac Drugs (Digoxin, Statins, Antiarrhythmics)
Digoxin: digoxin is a positive inotrope used in heart failure and rate control in atrial fibrillation. It has a narrow therapeutic index (target trough 0.5-2.0 ng/mL) and is primarily a P-glycoprotein substrate (not CYP-metabolized). Hypericum's P-gp induction can reduce digoxin levels by 25-30%, with risk of loss of rate control in atrial fibrillation or worsening heart failure. Co-administration generally avoided; if necessary, digoxin levels monitored closely.
Statins: cholesterol-lowering HMG-CoA reductase inhibitors. Susceptibility to hypericum interaction varies by specific statin:
- Simvastatin — predominantly CYP3A4 metabolized; significant reduction in plasma levels with hypericum, with reduced LDL-lowering effect
- Atorvastatin — CYP3A4 metabolized; moderate interaction
- Lovastatin — CYP3A4 metabolized; similar to simvastatin
- Pravastatin, rosuvastatin, pitavastatin, fluvastatin — minimal CYP3A4 dependence; lower interaction risk. Preferred statins for patients on hypericum if statin therapy is essential
Calcium channel blockers: most CCBs (amlodipine, nifedipine, felodipine, diltiazem, verapamil) are CYP3A4 substrates with reduced antihypertensive effect possible with hypericum co-administration. Monitor blood pressure if combination is used.
Antiarrhythmics: amiodarone, quinidine, and dronedarone are CYP3A4 substrates with reduced antiarrhythmic effect possible. Amiodarone is particularly problematic because its long half-life means CYP induction effects persist for weeks after hypericum discontinuation.
Ivabradine: a sinus-node funny-current (If) inhibitor used in heart failure; significant CYP3A4 substrate with reduced efficacy with hypericum co-administration. Co-administration discouraged.
Beta-blockers: most beta-blockers have lower CYP3A4 dependence and lower interaction risk with hypericum. Carvedilol has some CYP2D6 metabolism but is less affected than CYP3A4 substrates.
Aspirin and NSAIDs: low interaction risk pharmacokinetically, but combination with hypericum theoretically increases bleeding risk via additive antiplatelet and platelet-function effects (hypericum has weak antiplatelet effect via several mechanisms). Monitor for bleeding if combination is used.
Chemotherapy and Targeted Cancer Therapies
Patients on active cancer treatment face particular risk from hypericum interactions because many chemotherapy agents and most targeted molecular therapies are CYP3A4 substrates with narrow therapeutic indices. Reduced plasma levels of chemotherapy mean reduced anticancer effect, potentially compromising treatment success.
Specific concerns:
- Tyrosine kinase inhibitors (imatinib for CML, sunitinib for renal cell carcinoma, erlotinib for non-small-cell lung cancer, sorafenib, dasatinib, nilotinib, gefitinib, and many others) — nearly all are CYP3A4 substrates with significant reduction in plasma levels expected with hypericum co-administration
- Irinotecan: hypericum reduces the AUC of the active metabolite SN-38 by approximately 40% with corresponding reduction in anticancer effect
- Cyclophosphamide: complex interaction; hypericum may either reduce or increase active metabolite formation depending on metabolic pathway dynamics
- Tamoxifen: complex interaction. Tamoxifen requires CYP2D6 activation to the more potent endoxifen metabolite. Hypericum's effects on CYP2D6 are weak, but the parallel CYP3A4 induction affects tamoxifen disposition in complex ways. Net clinical effect on tamoxifen efficacy uncertain but caution warranted in breast cancer patients
- Docetaxel, paclitaxel: CYP3A4 substrates with reduced plasma levels and reduced anticancer effect expected
- Etoposide: CYP3A4 substrate with reduced levels
- Vinca alkaloids (vincristine, vinblastine, vinorelbine): CYP3A4 substrates with reduced levels
- Immune checkpoint inhibitors (pembrolizumab, nivolumab, atezolizumab, etc.): low interaction risk pharmacokinetically (these are monoclonal antibodies not CYP-metabolized), but caution still warranted given the importance of cancer treatment efficacy
The general principle for cancer patients: do not start hypericum during active anticancer treatment. For depression management in cancer patients, conventional antidepressants (citalopram, escitalopram, mirtazapine, bupropion) with known interaction profiles are preferred. Cancer patients in survivorship who are stable on adjuvant therapy or surveillance should consult their oncology team before starting hypericum.
Anticonvulsants and Psychiatric Medications
Anticonvulsants used both for seizure disorders and increasingly for mood stabilization (bipolar disorder), neuropathic pain, and migraine prophylaxis have complex interactions with hypericum:
- Carbamazepine and oxcarbazepine: both are CYP3A4 inducers themselves; co-administration with hypericum produces mutual induction with reduced levels of both drugs and possibly seizure breakthrough. Combination not recommended
- Phenytoin: CYP3A4 and CYP2C9 substrate; reduced levels with hypericum and possibly seizure breakthrough
- Phenobarbital: itself a CYP3A4 inducer; mutual induction with hypericum
- Lamotrigine: primarily UGT1A4 metabolized; UGT induction by hyperforin reduces lamotrigine levels modestly, with possible reduced mood stabilization or seizure breakthrough
- Valproate: complex interaction; reduced free valproate levels possible
- Levetiracetam (Keppra): predominantly renal elimination; minimal interaction with hypericum. One of the safest anticonvulsant choices in a patient also on hypericum
- Topiramate: partial CYP3A4 metabolism; modest interaction
- Gabapentin and pregabalin: renal elimination; minimal interaction with hypericum. Safe combinations
The combination of hypericum with anticonvulsants used for mood stabilization in bipolar disorder is doubly problematic: (1) the pharmacokinetic interaction reduces mood stabilizer effectiveness, and (2) hypericum itself, like other antidepressants, can precipitate manic episodes in bipolar patients. Hypericum is generally contraindicated in bipolar disorder.
Antipsychotic medications:
- Clozapine: primarily CYP1A2 substrate; reduced levels with hypericum induction. Clozapine has a narrow therapeutic window and reduced levels may produce psychotic decompensation
- Olanzapine: CYP1A2 and CYP2D6 substrate; modest interaction
- Quetiapine, aripiprazole, risperidone, ziprasidone: predominantly CYP3A4 metabolized; reduced levels with hypericum
- Lurasidone, iloperidone, brexpiprazole: CYP3A4 substrates; reduced levels
The recommendation for any patient on antipsychotic therapy for schizophrenia, schizoaffective disorder, or bipolar disorder is to avoid hypericum. The risk of psychiatric decompensation from sub-therapeutic antipsychotic levels is high and not easily monitored clinically.
FDA, EMA, and Health Canada Warning History
The international regulatory response to hypericum drug interactions provides important context:
- February 2000 — US FDA Public Health Advisory: triggered by Piscitelli et al. (Lancet, February 12, 2000) demonstrating 57% reduction in indinavir AUC with hypericum co-administration. The FDA issued a Public Health Advisory warning healthcare professionals and patients of the risk of significant drug interactions with St. John's Wort, particularly the contraindication with HIV protease inhibitors. The FDA also recommended that healthcare providers ask all patients about St. John's Wort use, that pharmacists counsel patients about interactions, and that patients disclose use to all prescribers
- 2000 — UK MHRA Warning: the UK Medicines and Healthcare products Regulatory Agency (then known as MCA) issued warnings about St. John's Wort interactions with multiple drug classes including oral contraceptives, warfarin, cyclosporine, digoxin, and HIV antiretrovirals
- 2002 — Health Canada Advisory: Health Canada issued an advisory on St. John's Wort drug interactions covering similar classes
- 2002 — Therapeutic Goods Administration (Australia) Bulletin: Australian TGA published guidance on hypericum interactions
- 2004 — European Medicines Agency Reflection Paper: EMA issued comprehensive guidance on hypericum interactions, recommending that any prescription medicine label include a warning about possible interactions with hypericum if the drug is metabolized by CYP3A4 or transported by P-gp
- 2007 — UK Drug Safety Update: MHRA reiterated warnings and noted ongoing reports of contraceptive failure and other interactions in the Yellow Card pharmacovigilance database
- Current Status (2025): All major international drug regulators maintain ongoing warnings about hypericum interactions. In the EU, St. John's Wort is regulated as a herbal medicinal product with mandatory package-insert warnings about specific drug interactions. In the US, OTC St. John's Wort products typically carry voluntary warning labels but regulation is less strict than for prescription products
The regulatory warnings have been consistent in their message: any patient taking prescription medications should consult a healthcare provider before starting St. John's Wort, and any healthcare provider seeing a patient on St. John's Wort should review all concurrent medications for potential interactions before continuing or prescribing additional therapy.
Surgical and Anesthetic Considerations
St. John's Wort interactions with anesthetic and surgical medications create specific perioperative concerns:
- Anesthetic agents: many inhaled and IV anesthetics are CYP3A4 substrates; reduced plasma levels may produce inadequate anesthesia or unpredictable recovery profile
- Opioid analgesics: fentanyl, alfentanil, sufentanil, remifentanil, methadone, oxycodone are CYP3A4 substrates with reduced analgesic effect possible
- Muscle relaxants: some neuromuscular blockers are P-gp substrates with altered duration of action
- Antiarrhythmic agents: used intraoperatively or in ICU; CYP3A4 substrate interactions
- Bleeding risk: hypericum has weak antiplatelet activity that may increase surgical bleeding risk
- Postoperative drug-induced delirium: hypericum's effects on multiple neurotransmitter systems may interact unpredictably with anesthetic emergence and postoperative analgesia
- Postoperative wound healing: ironic concern given hypericum's topical wound-healing applications — oral hypericum may have systemic effects that affect wound healing differently than topical application
The standard recommendation from the American Society of Anesthesiologists and most surgical societies is to discontinue St. John's Wort at least 5 days, ideally 2 weeks, before any planned surgery. The 5-day minimum allows substantial reversal of hyperforin-mediated TRPC6/monoamine effects and partial reversal of CYP3A4 induction. The 2-week ideal allows more complete reversal of CYP3A4 induction.
For emergency surgery in patients on hypericum, the surgical and anesthetic team should be informed so that drug doses and choices can be adjusted accordingly.
Postoperative resumption of hypericum: can typically be resumed once the patient has stabilized postoperatively (1-2 weeks), is off most acute pain medications, and is not on any of the contraindicated postoperative drugs (e.g., warfarin for DVT prophylaxis, certain antibiotics, certain analgesics).
Clinical Decision Framework
For any patient considering St. John's Wort, the following decision framework applies:
- Comprehensive medication review: list every prescription medication, every over-the-counter medication, every herbal supplement, every vitamin, and every recreational substance the patient uses. Bring this list to a pharmacist or physician for drug-interaction review. Many drug-interaction databases (Lexi-Interact, Micromedex, Stockley's Drug Interactions) include hypericum and will flag potential interactions
- Identify any ABSOLUTELY CONTRAINDICATED combinations: HIV antiretrovirals, immunosuppressants in transplant patients, MAO inhibitors, active chemotherapy. If any of these are present, hypericum cannot be used — consider alternative depression treatment
- Identify STRONGLY DISCOURAGED combinations: SSRIs, SNRIs, tricyclics, triptans, tramadol, warfarin (and other anticoagulants), hormonal contraception in women who depend on it for pregnancy prevention. If any of these are present, consider whether the patient can transition off the problematic medication or whether alternative depression treatment is preferable
- Identify SIGNIFICANT INTERACTIONS: cardiac medications, statins, anticonvulsants, antipsychotics, calcium channel blockers, theophylline, methadone, sildenafil, etc. These are often manageable with awareness and monitoring, but require informed decision-making
- Counsel the patient: explain that the herb has more drug interactions than any other commonly used supplement; that the interactions are real and clinically consequential, not theoretical; that the patient must disclose use to every healthcare provider, dentist, and pharmacist they encounter; that any new medication added during hypericum use requires prescriber awareness; that surgery requires 5-day pre-operative discontinuation; that the 2-week onset window applies (cannot expect immediate effect)
- Plan monitoring: for patients on warfarin, INR every 1-2 weeks initially; for transplant patients (where hypericum should not be used at all), trough drug levels; for HIV patients (where hypericum is contraindicated), viral load monitoring
- Plan discontinuation strategy: how long is the patient planning to take hypericum? What new medications might be needed during that time? What if the patient gets sick and needs antibiotic therapy or other acute drug treatment? Build the discontinuation plan into the initiation plan
For the prudent patient, the decision tree often comes down to: if any of the absolutely-contraindicated or strongly-discouraged medications are present, do not use hypericum — choose another treatment. The clinical efficacy of hypericum for mild-moderate depression is real, but it is not so dramatically superior to other options (conventional pharmaceuticals, other herbal antidepressants like Saffron, lifestyle interventions, CBT, exercise) that it justifies high-risk drug interactions.
For patients on no other medications, hypericum at standard 900 mg/day dosing of a quality standardized extract is well-tolerated and effective for mild-to-moderate depression, mood symptoms, mild seasonal affective disorder, and menopausal mood symptoms. The interaction profile becomes relevant only when other medications enter the picture.
Key Research Papers
- Piscitelli SC, Burstein AH, Chaitt D, Alfaro RM, Falloon J (2000). Indinavir concentrations and St John's wort. The Lancet, 355(9203):547-8. The pivotal indinavir interaction paper that triggered the FDA warning. — PubMed: Piscitelli 2000 indinavir
- Moore LB, Goodwin B, Jones SA, Wisely GB, Serabjit-Singh CJ, Willson TM, Collins JL, Kliewer SA (2000). St. John's wort induces hepatic drug metabolism through activation of the pregnane X receptor. PNAS, 97(13):7500-2. The PXR/CYP3A4 mechanism paper. — PubMed: Moore PXR 2000
- Markowitz JS, Donovan JL, DeVane CL, Taylor RM, Ruan Y, Wang JS, Chavin KD (2003). Effect of St John's wort on drug metabolism by induction of cytochrome P450 3A4 enzyme. JAMA, 290(11):1500-4. JAMA mechanism paper. — PubMed: Markowitz JAMA 2003
- Henderson L, Yue QY, Bergquist C, Gerden B, Arlett P (2002). St John's wort (Hypericum perforatum): drug interactions and clinical outcomes. British Journal of Clinical Pharmacology, 54(4):349-56. Comprehensive interaction review. — PubMed: Henderson BJCP review
- Mannel M (2004). Drug interactions with St John's wort: mechanisms and clinical implications. Drug Safety, 27(11):773-97. Drug Safety review. — PubMed: Mannel Drug Safety 2004
- Schwarz UI, Buschel B, Kirch W (2003). Unwanted pregnancy on self-medication with St John's wort despite hormonal contraception. British Journal of Clinical Pharmacology, 55(1):112-3. Documented contraceptive failure case. — PubMed: Schwarz contraceptive failure
- Ruschitzka F, Meier PJ, Turina M, Lüscher TF, Noll G (2000). Acute heart transplant rejection due to Saint John's wort. The Lancet, 355(9203):548-9. Documented heart transplant rejection. — PubMed: Ruschitzka heart rejection
- Yue QY, Bergquist C, Gerden B (2000). Safety of St John's wort (Hypericum perforatum). The Lancet, 355(9203):576-7. Swedish pharmacovigilance experience with warfarin and other interactions. — PubMed: Yue 2000 safety
- Lantz MS, Buchalter E, Giambanco V (1999). St. John's wort and antidepressant drug interactions in the elderly. Journal of Geriatric Psychiatry and Neurology, 12(1):7-10. Serotonin syndrome case series. — PubMed: Lantz serotonin syndrome
- Hall SD, Wang Z, Huang SM, Hamman MA, Vasavada N, Adigun AQ, Hilligoss JK, Miller M, Gorski JC (2003). The interaction between St John's wort and an oral contraceptive. Clinical Pharmacology and Therapeutics, 74(6):525-35. Detailed pharmacokinetic study of OC interaction. — PubMed: Hall OC interaction
- Johne A, Brockmöller J, Bauer S, Maurer A, Langheinrich M, Roots I (1999). Pharmacokinetic interaction of digoxin with an herbal extract from St John's wort (Hypericum perforatum). Clinical Pharmacology and Therapeutics, 66(4):338-45. Digoxin interaction characterization. — PubMed: Johne digoxin
- Mai I, Bauer S, Störmer E, Kuchler A, Mueller-Oerlinghausen B, Roots I (2004). Hyperforin content determines the magnitude of the St John's wort-cyclosporine drug interaction. Clinical Pharmacology and Therapeutics, 76(4):330-40. Hyperforin dose-response in cyclosporine interaction. — PubMed: Mai cyclosporine
PubMed Topic Searches
- PubMed: Hypericum CYP3A4 induction
- PubMed: Hypericum oral contraceptive failure
- PubMed: Hypericum warfarin INR
- PubMed: Hypericum transplant rejection
- PubMed: Hypericum serotonin syndrome
- PubMed: Hyperforin PXR mechanism
- PubMed: Hypericum HIV antiretroviral
Connections
- St. John's Wort Benefits Hub
- St. John's Wort Overview
- St. John's Wort for Depression
- Mood & Seasonal Depression
- Antiviral & Wound Healing
- Depression
- Bipolar Disorder
- Atrial Fibrillation (Warfarin)
- Heart Failure (Digoxin)
- Endocrinology (Hormonal Contraception)
- Infectious Disease (HIV)
- INR Monitoring
- Saffron (Alternative Antidepressant)
- Rhodiola Rosea (Alternative)
- Ashwagandha
- Stress Management
- All Herbs