St. John's Wort for Antiviral and Wound-Healing Applications
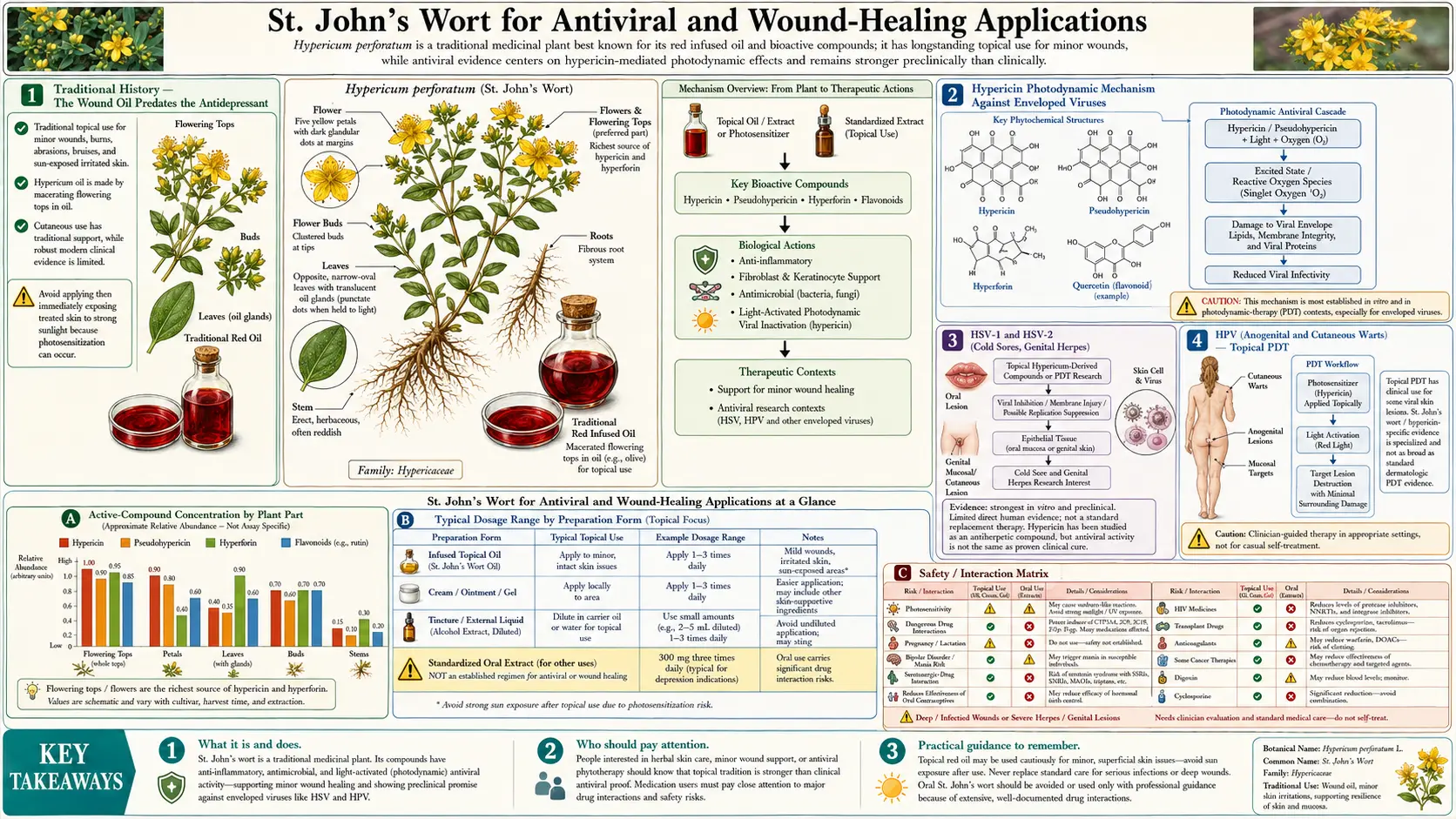
Long before St. John's Wort became famous as an antidepressant in the 1990s, the herb was renowned throughout European folk medicine as a wound-healing and nerve-soothing topical. The traditional preparation called Oleum Hyperici, "St. John's Oil," or "Red Oil" — fresh hypericum flowers infused in olive oil and sun-cured for several weeks until the oil turned deep crimson with extracted hypericin — was a staple of household medicine cabinets from medieval times through the 19th century. Modern research has substantially validated the traditional indications: hypericin is a potent photodynamic agent generating singlet oxygen under visible light that damages enveloped viral particles (HSV-1, HSV-2, HPV, influenza), hyperforin directly disrupts bacterial membranes including those of methicillin-resistant Staphylococcus aureus (MRSA), and the topical oil's combination of anti-inflammatory flavonoids, tannins, and tissue-regenerating activity produces measurably faster epithelialization in burns, bruises, abrasions, and surgical wounds. Hypericin photodynamic therapy (PDT) for HSV cold sores, anogenital HPV warts, and certain skin malignancies is an active area of contemporary translational research. This deep-dive explores the antiviral mechanisms, the traditional and modern topical applications, the nerve-pain indications (trigeminal neuralgia, post-herpetic neuralgia, sciatica), the bacterial-skin-infection applications including MRSA, and the home preparation of traditional infused oil.
Table of Contents
- Traditional History — The Wound Oil Predates the Antidepressant
- Hypericin Photodynamic Mechanism Against Enveloped Viruses
- HSV-1 and HSV-2 (Cold Sores, Genital Herpes)
- HPV (Anogenital and Cutaneous Warts) — Topical PDT
- Influenza, Hepatitis, and Other Enveloped Viruses
- Hyperforin Antibacterial — MRSA and Skin Pathogens
- Wound-Healing Mechanism (Flavonoids, Tannins, Tissue Regeneration)
- Burns, Bruises, and Minor Abrasions
- Surgical Wound Recovery
- Nerve-Pain Applications (Trigeminal Neuralgia, Post-Herpetic Neuralgia, Sciatica)
- Home Preparation of Traditional Infused Oil
- Topical Cautions and Photosensitivity
- Key Research Papers
- Connections
- Featured Videos
Traditional History — The Wound Oil Predates the Antidepressant
The modern association of Hypericum perforatum with mental health dates only to the late 20th century, but the herb's European medicinal history spans nearly two thousand years — and almost all of that history concerns its topical and wound-care use, not its psychological applications. The first-century Greek physician Dioscorides described hypericum in De Materia Medica as useful for "burns, sciatica, ulcers, and the bites of venomous beasts," recommending the freshly bruised herb applied directly to wounds. Pliny the Elder noted similar uses in his Natural History.
Through the medieval period, hypericum-infused oil (Oleum Hyperici) became a near-universal feature of European household medicine. The Benedictine and Franciscan monasteries cultivated the plant in apothecary gardens and prepared the red oil for treatment of:
- Burns from cooking fires, candles, and household accidents
- Bruises and contusions from manual labor and falls
- Open wounds, abrasions, and lacerations — often after suturing
- Nerve pain along defined anatomic distributions (what we now call neuralgia)
- Sciatica and back pain (massaged into affected areas)
- Skin ulcers and bedsores in immobilized patients
- Insect bites, stings, and the inflammatory reactions thereof
- Hemorrhoids (applied topically)
- Cracked nipples in nursing mothers
By the 17th-19th centuries, hypericum-infused oil was a routine entry in European pharmacopoeias and was carried in the medical kits of military surgeons. The British naval surgeon's manuals listed it for burns from gunpowder accidents and for shrapnel wound aftercare. The traditional knowledge encoded centuries of empirical observation: applied topically, this red oil predictably accelerated healing and reduced pain in a wide range of skin and soft-tissue injuries.
Modern mechanistic research has substantially validated the traditional use. The combination of hypericin (photodynamic antimicrobial and tissue-stimulating effects), hyperforin (anti-inflammatory, antibacterial including MRSA, and possibly tissue regenerative), flavonoids (antioxidant and anti-inflammatory), and tannins (astringent and antimicrobial) collectively produces the documented topical effects that European folk medicine had identified empirically over centuries.
Hypericin Photodynamic Mechanism Against Enveloped Viruses
Hypericin is the principal compound responsible for the antiviral activity of St. John's Wort. The mechanism is photodynamic: hypericin acts as a photosensitizer, absorbing visible light (peak absorption in the 540-610 nm green-yellow-orange range) and transferring that energy to molecular oxygen, generating singlet oxygen (a reactive electronically excited form of O2) and other reactive oxygen species (superoxide, hydroxyl radicals, peroxides).
These reactive oxygen species do not differentiate between host cells and pathogens, but the geometry of the photodynamic interaction strongly favors damage to enveloped viral particles because:
- Viral envelope lipids and proteins are particularly susceptible to singlet-oxygen-mediated peroxidation, disrupting the envelope and rendering the virus unable to bind target cells
- Viral genomic nucleic acids, once released from the damaged envelope, are degraded by reactive species
- The viral genome (a few thousand to a few hundred thousand bases) has many fewer redundant copies than a host cell genome, so any damage is much more functionally consequential
- Hypericin preferentially accumulates in the lipid envelope of viral particles due to its lipophilic nature
The result is selective destruction of enveloped viruses while topical host cells — with their robust DNA repair machinery, much larger genome, and antioxidant defenses — experience comparatively limited damage. The pattern is similar to other clinically used photodynamic photosensitizers (porphyrins, phthalocyanines) but with a substantially different photochemistry profile.
Hypericin photodynamic activity has been documented in vitro against a wide range of enveloped viruses including:
- Herpes simplex virus 1 (HSV-1) — oral cold sores
- Herpes simplex virus 2 (HSV-2) — genital herpes
- Varicella zoster virus (VZV) — chickenpox and shingles
- Cytomegalovirus (CMV)
- Epstein-Barr virus (EBV)
- Influenza A and B
- Hepatitis B and C viruses
- Human immunodeficiency virus (HIV)
- Vesicular stomatitis virus
- Murine cytomegalovirus
Non-enveloped viruses (adenovirus, rotavirus, poliovirus, papillomavirus) are generally less susceptible to hypericin photodynamic inactivation, with one important exception — topical photodynamic therapy with hypericin for HPV warts has shown clinical benefit, possibly through mechanisms beyond direct viral inactivation including immune-mediated wart-cell killing.
HSV-1 and HSV-2 (Cold Sores, Genital Herpes)
Herpes simplex virus is the textbook example of an enveloped virus susceptible to hypericin photodynamic inactivation. Topical hypericum-infused oil and modern hypericin photodynamic preparations have been investigated for:
- HSV-1 oral cold sores (also called fever blisters or herpes labialis): traditional and modern application of hypericum oil directly to the lesion 3-4 times daily, ideally beginning at the prodromal tingle phase before the vesicle has formed. Anecdotal reports and small clinical observations suggest reduced lesion duration and severity compared to no treatment
- HSV-2 genital herpes lesions: similar topical application with the same caveats. Clinical evidence is more limited than for cold sores due to the practical difficulty of randomized trials in genital herpes
- Recurrent HSV prophylaxis: an interesting hypothesis (not yet well-tested clinically) is that oral hypericum's mood-stabilizing effects might reduce HSV recurrence frequency by reducing stress-mediated immunosuppression, which is a known HSV reactivation trigger. The hypothesis has biological plausibility but lacks rigorous trial evidence
Practical topical HSV protocol with traditional hypericum oil:
- Apply traditional sun-cured hypericum oil (deep red color, prepared as described in the home-preparation section below) to affected lesion or prodromal site 3-4 times daily
- Use a cotton swab to avoid finger contact with the lesion (HSV is highly transmissible)
- Continue until lesion crusts over and resolves (typically 5-10 days for cold sores)
- Avoid sun exposure to the treated area while oil is being applied (the same photosensitization that gives the oil its antiviral effect also makes treated skin sensitive to sunburn)
- Discontinue oil application once the lesion has fully healed; do not use continuously between outbreaks
Modern hypericin photodynamic therapy (PDT) protocols in dermatology research extend the traditional oil application to a more controlled clinical context: a standardized hypericin preparation is applied topically to the lesion, allowed to penetrate for 30-60 minutes, then activated by exposure to a controlled visible light source (typically broad-spectrum visible or specific 590-610 nm wavelength). This produces a more intense and controlled photodynamic effect than ambient-light activation of traditional oil application.
The most established conventional treatments for HSV remain oral antivirals (acyclovir, valacyclovir, famciclovir), which are highly effective and well-tolerated. Hypericum topical use is reasonable as an adjunct or for patients who cannot tolerate or do not have access to conventional antiviral therapy, but it is not first-line for severe or frequent HSV recurrences. For more on the relevant disease, see our Shingles page (varicella zoster, related to HSV but a distinct virus with its own treatment considerations).
HPV (Anogenital and Cutaneous Warts) — Topical PDT
Human papillomavirus (HPV) is a non-enveloped virus, and direct hypericin photodynamic inactivation of viral particles is less efficient than for enveloped viruses. Despite this, hypericin topical PDT has shown clinical benefit for HPV-related warts through a different mechanism — selective destruction of the wart cells themselves rather than direct viral inactivation. The mechanism: hypericin preferentially accumulates in proliferating wart-cell tissue, photodynamic activation destroys the wart cells, and the immune system clears the resulting cellular debris and any persistent viral particles.
Clinical investigations have explored hypericin PDT for:
- Anogenital warts (condylomata acuminata): topical hypericin application followed by light activation has shown clearance rates broadly comparable to conventional treatments like imiquimod, podophyllotoxin, or cryotherapy, with possibly less local irritation
- Common cutaneous warts (verruca vulgaris): traditional hypericum oil application has been used in folk medicine for warts on hands, feet, and face. Clinical evidence is mostly anecdotal but the mechanism is biologically plausible
- Plantar warts: similar to common warts, with the practical limitation that the thick plantar skin reduces penetration of topical preparations
- Cervical intraepithelial neoplasia (CIN): experimental hypericin PDT has been investigated for HPV-associated cervical dysplasia in early-stage research, with some encouraging preliminary results but not yet established as clinical practice
For routine HPV wart management, conventional treatments (cryotherapy, imiquimod 5% cream, podophyllotoxin, salicylic acid for common warts, sinecatechin/Veregen for genital warts) remain the standard of care. Hypericum topical preparations are reasonable as an alternative for patients who decline or have failed conventional therapy, or as an adjunct in supportive care.
Influenza, Hepatitis, and Other Enveloped Viruses
The in vitro photodynamic activity of hypericin against influenza, hepatitis B, hepatitis C, and HIV has been documented in laboratory research but has not translated into established clinical antiviral applications for these systemic infections. The fundamental problem is that effective in vivo systemic antiviral activity would require both adequate hypericin plasma concentrations and adequate light penetration to the tissues where viral replication occurs — and visible light does not penetrate deep tissues effectively. Hypericin photodynamic activity is therefore practically limited to topical and superficial applications where light can reach the infected tissue.
Two niches where hypericin antiviral activity may have practical application:
- Blood-product decontamination: hypericin can be added to blood products (plasma, platelet concentrates, packed red cells) and the product then exposed to light to inactivate any contaminating enveloped viruses (HIV, hepatitis B and C, CMV, EBV) before transfusion. This is an extracorporeal application where light penetration is achievable and viral inactivation is selective. Hypericin and related compounds have been investigated for this application though current commercial blood-decontamination systems use other photosensitizers (riboflavin, amotosalen)
- Topical influenza/respiratory infections: speculative application of hypericin nasal spray or throat spray for prophylaxis or early treatment of upper respiratory enveloped viruses has been proposed but is not well-tested clinically
For systemic antiviral applications, conventional antivirals (oseltamivir for influenza, direct-acting antivirals for hepatitis C, combination antiretroviral therapy for HIV) are highly effective and remain the standard of care. Hypericum oral supplementation does not provide meaningful systemic antiviral activity, and may in fact be contraindicated in HIV due to its CYP3A4 induction that reduces antiretroviral drug levels by 50% or more.
Hyperforin Antibacterial — MRSA and Skin Pathogens
Beyond the hypericin photodynamic antiviral activity, hypericum extracts contain hyperforin, which has demonstrated direct antibacterial activity through a different mechanism: hyperforin disrupts bacterial cell membranes by inserting into the lipid bilayer and dissipating the membrane proton gradient that bacteria require for ATP synthesis. The activity is most pronounced against Gram-positive bacteria.
The most clinically interesting finding: hyperforin shows potent activity against methicillin-resistant Staphylococcus aureus (MRSA) in vitro, with minimum inhibitory concentrations in the low-micromolar range and bactericidal (not just bacteriostatic) effect. Schempp et al. (1999) and subsequent investigators have characterized this activity in detail. The mechanism is membrane-disruptive rather than target-protein-binding, which is why MRSA resistance (mediated by altered penicillin-binding protein PBP2a that confers beta-lactam resistance) does not confer cross-resistance to hyperforin.
Documented hyperforin antibacterial spectrum includes:
- Staphylococcus aureus, including MRSA and vancomycin-intermediate isolates
- Staphylococcus epidermidis (common cause of catheter and prosthesis infections)
- Streptococcus species including group A streptococcus
- Enterococcus species including some vancomycin-resistant isolates
- Corynebacterium species
- Limited activity against Gram-negatives (E. coli, Klebsiella, Pseudomonas typically not inhibited at clinically achievable concentrations)
- Anti-mycobacterial activity against M. tuberculosis documented in vitro at high concentrations
Clinical translation of hyperforin antibacterial activity has focused primarily on topical applications:
- Atopic dermatitis colonized with S. aureus: hypericum cream containing standardized hyperforin has been investigated for atopic dermatitis patients with secondary S. aureus colonization, showing reduced bacterial counts and clinical improvement in eczema severity in small randomized trials
- Wound infection prevention: traditional hypericum oil application to clean wounds (as part of the broader wound-healing protocol) may contribute antibacterial activity that reduces infection rate, though this is difficult to separate from the oil's other wound-healing mechanisms in clinical studies
- Acne: topical hypericum preparations have been investigated for acne, where the antibacterial activity against Cutibacterium acnes (formerly Propionibacterium acnes) combined with the anti-inflammatory effect could be relevant. Clinical evidence is preliminary
For serious systemic bacterial infection, oral hypericum is not adequate antibacterial therapy and conventional antibiotic treatment is required. The topical hyperforin antibacterial activity is best understood as a complementary mechanism to the oil's broader wound-healing effects rather than a standalone antibacterial treatment.
Wound-Healing Mechanism (Flavonoids, Tannins, Tissue Regeneration)
The wound-healing properties of hypericum-infused oil arise from the combined action of multiple compound classes:
- Flavonoids (quercetin, rutin, hyperoside, isoquercitrin) — provide antioxidant activity that reduces oxidative damage in the wound environment, and anti-inflammatory effects through NF-kB inhibition that limits excessive inflammation that can delay healing
- Tannins — have astringent properties that promote tissue contraction at wound edges and antimicrobial activity that reduces bacterial colonization of the wound surface
- Hyperforin — provides direct antibacterial activity (especially against gram-positive skin flora including S. aureus and MRSA as noted above) and possibly direct tissue-regenerative effects through stimulation of keratinocyte and fibroblast proliferation
- Hypericin — provides photodynamic antibacterial and antiviral activity that reduces pathogen burden in the wound, and may directly stimulate angiogenesis and tissue regeneration
- Essential oils and other lipophilic compounds — provide additional anti-inflammatory and antimicrobial activity
- The olive oil carrier — provides occlusive moisturizing effect that maintains wound hydration, supports re-epithelialization, and reduces scarring
The net effect, documented in multiple clinical studies of standardized hypericum oil preparations, is accelerated wound healing characterized by:
- Faster epithelialization (the migration of keratinocytes across the wound surface to form new epidermis)
- Reduced inflammation and edema at the wound margin
- Lower bacterial colonization and infection rates
- Reduced pain at the wound site
- Reduced scar formation, particularly in burns and surgical wounds
- Improved healing in chronic wounds (pressure ulcers, venous stasis ulcers, diabetic foot ulcers) that have failed conventional treatment
Burns, Bruises, and Minor Abrasions
Burns: hypericum oil applied to first-degree (superficial epidermal) and minor second-degree (partial-thickness) burns has documented benefit in clinical studies. The oil is typically applied directly to the burn surface 2-3 times daily after initial cooling and gentle cleansing. Effects include:
- Faster re-epithelialization (5-10 days for superficial burns versus 7-14 days with petroleum-based dressings)
- Reduced pain during the healing process
- Lower infection rate (relevant for partial-thickness burns that have lost the epidermal barrier)
- Reduced scarring
For severe burns (deep partial-thickness, full-thickness, electrical burns, chemical burns, burns of greater than 10% body surface area, or burns of face/hands/genitalia/major joints), conventional emergency burn care is essential and hypericum oil is not appropriate first-line treatment. For minor home-care burns (small kitchen burns, sunburn, friction burns), hypericum oil is a reasonable household remedy.
Bruises and contusions: traditional and modern use of hypericum oil for bruises involves topical massage of the oil into intact skin overlying the contusion. The anti-inflammatory and circulatory-stimulating effects help resolve the bruise more rapidly. The combination of hypericum oil with Arnica (another classic herbal bruise remedy) in topical preparations is common in European phytotherapy. Apply 2-3 times daily until resolved.
Minor abrasions and shallow lacerations: after gentle cleansing with water (no vigorous scrubbing, no hydrogen peroxide which damages healing tissue), apply hypericum oil to the wound surface 2-3 times daily until epithelialized. Cover with a non-stick dressing if needed to prevent contamination, particularly for wounds in high-friction or contaminated areas.
Sunburn: a notable paradox in topical use. While oral hypericum can cause photosensitivity reactions, topical hypericum oil applied to sunburned skin has soothing effects, reducing redness and pain and promoting healing. The mechanism likely involves the anti-inflammatory flavonoids dominating over any minor photodynamic effect at the local site. Apply to sunburned skin 2-3 times daily after the initial burn has set, but avoid applying before further sun exposure (the oil itself, while soothing on already-sunburned skin, would theoretically increase photosensitivity on healthy skin).
Surgical Wound Recovery
Several European clinical investigations have examined hypericum oil for postoperative wound care, with the most rigorous evidence in:
- Cesarean section incisions: A 2010 randomized trial (Samadi et al.) of 144 postpartum women undergoing cesarean section randomized to topical hypericum oil 3 times daily versus placebo for 16 days postoperatively. The hypericum group showed significantly reduced pain (visual analog scale scores), faster wound healing as assessed by REEDA scale (Redness, Edema, Ecchymosis, Discharge, Approximation), and less scar formation at 8-week follow-up
- Episiotomy wounds: similar topical postpartum use has been investigated with broadly comparable findings — reduced pain, faster healing, less scarring
- Hemorrhoidectomy wounds: traditional and modern application for postoperative hemorrhoidectomy pain and healing has shown benefit in small clinical studies
- Mastectomy and breast reconstruction wounds: limited data but some clinical use exists in European surgical practice
Practical considerations for surgical wound use:
- Apply only after the initial wound has been sealed and any sutures are dry (typically 24-48 hours postoperatively for clean surgical wounds; longer if there is concern for wound dehiscence)
- Use a clean cotton-tipped applicator rather than fingers to maintain sterility
- Apply 2-3 times daily until the wound is fully healed
- Discontinue if any signs of infection appear (increased redness, warmth, drainage, fever) and seek conventional medical evaluation
- Do NOT apply to internal surgical sites (the topical use is for skin surface only)
- Coordinate with the surgical team — some surgical teams have preferences about topical applications during the early postoperative period
Nerve-Pain Applications (Trigeminal Neuralgia, Post-Herpetic Neuralgia, Sciatica)
Traditional herbalists classify St. John's Wort as a nervine — an herb that nourishes and restores the nervous system — and have used both topical and oral preparations for various nerve-pain conditions for centuries. Modern research suggests hypericin and hyperforin do have analgesic and neuroprotective effects, though the strength of clinical evidence varies by condition.
Trigeminal neuralgia: severe lancinating facial pain along the trigeminal nerve distribution. Conventional first-line treatment is carbamazepine (an anticonvulsant), with surgical decompression for refractory cases. Topical hypericum oil massaged along the affected facial nerve distribution has been used adjunctively in European phytotherapy, with anecdotal reports of pain reduction. Rigorous trial evidence is limited.
Post-herpetic neuralgia (PHN): persistent nerve pain after a shingles outbreak (varicella zoster reactivation). Topical hypericum oil application along the affected dermatome has been used both for acute shingles lesions and for the resulting post-herpetic neuralgia. The combination of antiviral activity (during the acute outbreak) and anti-inflammatory/analgesic activity (for both acute pain and PHN) is biologically appealing. Conventional first-line treatments for PHN include topical lidocaine, capsaicin, gabapentin/pregabalin, and tricyclic antidepressants. See our Shingles page for more on this condition.
Sciatica and back pain: massaging hypericum oil into the lumbar region and along the sciatic distribution down the affected leg has been a traditional European remedy for sciatic pain. The combination of anti-inflammatory effect (reducing nerve root inflammation), analgesic effect (modulating nociceptive signaling), and muscular relaxant effect from the massage itself may contribute to reported benefit. Not a substitute for evaluation of underlying causes (disc herniation, spinal stenosis, etc.).
Diabetic peripheral neuropathy: small studies and case reports of topical hypericum for the burning, tingling, and pain of diabetic peripheral neuropathy in feet and hands. Apply 2-3 times daily, with massage to enhance penetration. Combination with conventional treatments (alpha-lipoic acid, acetyl-L-carnitine, and where appropriate gabapentin/pregabalin or duloxetine) is reasonable.
Intercostal neuralgia: nerve pain along an intercostal nerve distribution, often from rib injury, surgical scar, or shingles reactivation in a thoracic dermatome. Topical hypericum oil application along the painful nerve distribution has been documented in European phytotherapy.
Oral hypericum for neuropathic pain: hyperforin's effects on serotonin and norepinephrine reuptake parallel the mechanism of duloxetine, an SNRI with established efficacy for diabetic peripheral neuropathy and fibromyalgia. Theoretically, oral hypericum could produce similar analgesic effects, though dedicated trials in neuropathic pain are limited. The drug-interaction profile of oral hypericum (see Critical Drug Interactions deep-dive) often precludes its use in patients on conventional pain medications, gabapentin, pregabalin, or tricyclics.
Home Preparation of Traditional Infused Oil
The traditional Oleum Hyperici can be prepared at home from fresh hypericum flowers if you have access to a clean source (cultivated in your garden or wildcrafted from an unpolluted area). The classic recipe:
- Harvest: collect fresh hypericum flower buds and just-opened flowers around the summer solstice (late June to mid-July in the northern hemisphere, when bloom is at peak). Pick flowers in mid-morning after dew has dried but before peak afternoon sun. Aim for approximately 1 cup of fresh flower material per pint of finished oil
- Prepare: gently rinse the flowers to remove any insects or debris, then spread on a clean cloth to dry for 1-2 hours (do not dry completely — you want flowers wilted but still containing their volatile oils)
- Crush lightly: gently crush the flowers in a mortar or with the back of a spoon to release the oil glands. The flowers should release a small amount of red juice when crushed — this is the hypericin
- Infuse: place the crushed flowers in a clean glass jar (mason jar or similar) and cover with cold-pressed extra-virgin olive oil to about 1 inch above the plant material. Stir gently to release any trapped air bubbles. Cover with cheesecloth or a clean paper towel secured with a rubber band (not a tight lid — you need some air exchange for the photodynamic processes to occur)
- Sun-cure: place the jar in a warm, sunny location (a south-facing windowsill in the northern hemisphere works well) for 4 to 6 weeks. The oil will gradually develop the characteristic deep red color as hypericin is extracted into the oil and undergoes photoactivation. Stir or invert the jar every few days to redistribute the flowers
- Strain and bottle: after 4-6 weeks, strain the oil through fine cheesecloth or a coffee filter into clean amber glass bottles (the amber glass protects the finished oil from continued light exposure, which would otherwise degrade the active compounds). Squeeze the spent flowers thoroughly to extract all infused oil. Store in a cool, dark place
- Shelf life: properly prepared and stored, the oil keeps for 1-2 years. Discard if it develops a rancid smell, mold, or off color
The finished oil should be a deep, clear crimson-red color — a properly cured oil is dramatically darker than commercial preparations that have not been sun-cured. The intense color is the visible signature of high hypericin content.
For those who do not want to prepare their own, high-quality commercial hypericum oil is available from European herbal companies (particularly German and Italian brands with long traditions in the preparation). Choose preparations that are sun-cured rather than heat-extracted, that have the characteristic deep red color, and that are packaged in amber glass.
Topical Cautions and Photosensitivity
Topical hypericum is generally well-tolerated, but several cautions apply:
- Photosensitivity: skin to which hypericum oil has been applied may be more sensitive to sun-induced burning. Apply primarily in the evening or to skin that will not be sun-exposed in the next 24 hours, and use sunscreen on treated areas if sun exposure is unavoidable. This is particularly important for fair-skinned individuals
- Allergic contact dermatitis: rare but reported reactions to topical hypericum. If redness, itching, or rash develops at the application site, discontinue and consider alternative therapy
- Open wound concerns: while hypericum oil is appropriate for clean superficial wounds, it is NOT appropriate for deep puncture wounds (puncture wounds need to drain and remain open for infection clearance), severe burns (consult emergency care), bites from animals (need antimicrobial coverage and possibly rabies prophylaxis), or any wound with signs of infection (increasing redness, drainage, fever)
- Eye contact: do not apply to or near the eyes. The oil can cause irritation, and hypericin may be a retinal photosensitizer at high concentrations
- Pregnancy and breastfeeding: topical application to localized small areas is unlikely to produce systemic exposure of concern, but large-area application or chronic use is best avoided in pregnancy and breastfeeding due to general caution with hypericum
- Drug interactions from topical use: topical hypericum application produces minimal systemic absorption and does not generally produce the CYP3A4 induction associated with oral hypericum. However, large-area applications or chronic use over many weeks could theoretically produce some systemic effect. The drug-interaction concerns for oral hypericum do not typically apply to occasional topical use of small amounts of oil
Key Research Papers
- Schempp CM, Pelz K, Wittmer A, Schöpf E, Simon JC (1999). Antibacterial activity of hyperforin from St John's wort, against multiresistant Staphylococcus aureus and gram-positive bacteria. The Lancet, 353(9170):2129. The seminal hyperforin/MRSA paper. — PubMed: Schempp hyperforin MRSA
- Meruelo D, Lavie G, Lavie D (1988). Therapeutic agents with dramatic antiretroviral activity and little toxicity at effective doses: aromatic polycyclic diones hypericin and pseudohypericin. PNAS, 85(14):5230-4. The original hypericin antiviral discovery paper. — PubMed: Meruelo 1988 hypericin
- Lavie G et al. (1989). Studies of the mechanisms of action of the antiretroviral agents hypericin and pseudohypericin. PNAS, 86(15):5963-7. Hypericin antiviral mechanism elucidation. — PubMed: Lavie 1989 mechanism
- Wood S, Huffman J, Weber N, Andersen D, North J, Murray B, Sidwell R, Hughes B (1990). Antiviral activity of naturally occurring anthraquinones and anthraquinone derivatives. Planta Medica, 56(6):651-2. Hypericin antiviral spectrum. — PubMed: Wood antiviral spectrum
- Samadi S et al. (2010). The effect of Hypericum perforatum on the wound healing and scar of cesarean. Journal of Alternative and Complementary Medicine, 16(1):113-7. Postoperative cesarean wound trial. — PubMed: Samadi cesarean trial
- Reichling J, Weseler A, Saller R (2001). A current review of the antimicrobial activity of Hypericum perforatum L. Pharmacopsychiatry, 34 Suppl 1:S116-8. Antimicrobial activity review. — PubMed: Reichling antimicrobial review
- Schempp CM, Windeck T, Hezel S, Simon JC (2003). Topical treatment of atopic dermatitis with St. John's wort cream — a randomized, placebo controlled, double blind half-side comparison. Phytomedicine, 10 Suppl 4:31-7. Atopic dermatitis topical trial. — PubMed: Schempp atopic dermatitis
- Süntar IP, Küpeli Akkol E, Yalçin FN, Koca U, Keles H, Yesilada E (2010). Wound healing potential of Sambucus ebulus L. leaves and isolation of an active component, quercetin 3-O-glucoside. Journal of Ethnopharmacology, 129(1):106-14. (Related wound-healing flavonoid research.) — PubMed: Süntar wound healing flavonoids
- Birt DF, Widrlechner MP, Hammer KD, Hillwig ML, Wei J, Kraus GA, Murphy PA, McCoy JA, Wurtele ES, Neighbors JD, Wiemer DF, Maury WJ, Price JP (2009). Hypericum in infection: identification of anti-viral and anti-inflammatory constituents. Pharmaceutical Biology, 47(8):774-782. Comprehensive antiviral/anti-inflammatory review. — PubMed: Birt hypericum infection
- Saddiqe Z, Naeem I, Maimoona A (2010). A review of the antibacterial activity of Hypericum perforatum L. Journal of Ethnopharmacology, 131(3):511-21. Antibacterial review. — PubMed: Saddiqe antibacterial review
- Kacerovská D et al. (2008). Photodynamic therapy of nonmelanoma skin cancer with topical hypericum perforatum extract: a pilot study. Photochemistry and Photobiology, 84(3):779-85. Hypericum PDT for skin cancer pilot. — PubMed: Kacerovská PDT pilot
- Mishenkova EL, Derbentseva NA, Garagulya AD, Litvin LN (1975). Antiviral properties of St. John's wort and preparations produced from it. Trudy Sezda Mikrobiologov, 4:222. Early Soviet hypericum antiviral research. — PubMed: Mishenkova antiviral
PubMed Topic Searches
- PubMed: Hypericum topical wound healing
- PubMed: Hypericin photodynamic therapy
- PubMed: Hyperforin antibacterial
- PubMed: Hypericum HSV
- PubMed: Hypericum burns
- PubMed: Hypericin HPV warts
Connections
- St. John's Wort Benefits Hub
- St. John's Wort Overview
- St. John's Wort for Depression
- Mood & Seasonal Depression
- Critical Drug Interactions
- Shingles (HSV/VZV)
- Chronic Pain
- Arnica (Bruise Synergy)
- Calendula
- Comfrey
- Aloe Vera
- Topical Wound Care
- MRSA
- Staphylococcus aureus
- All Herbs