St. John's Wort for Depression
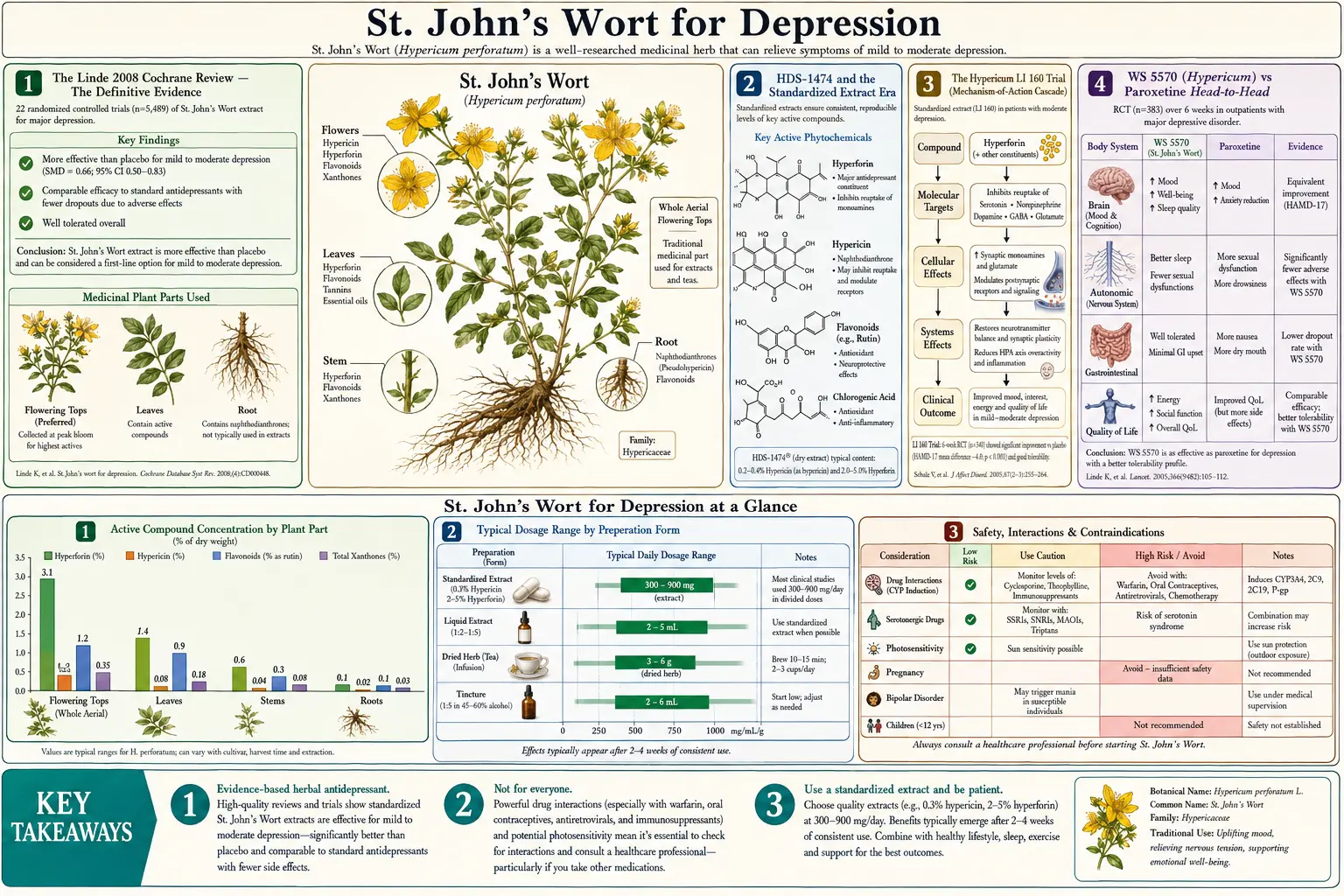
St. John's Wort is the single most rigorously studied herbal antidepressant in modern medicine. The 2008 Cochrane systematic review by Klaus Linde and colleagues pooled 29 randomized double-blind placebo-controlled trials covering 5,489 patients and concluded that standardized hypericum extracts were superior to placebo and statistically comparable to standard SSRI and tricyclic antidepressants for mild-to-moderate major depression — with a substantially lower side-effect burden. This deep-dive walks through the pivotal trials (Hypericum LI 160, WS 5570, HDS-1474), the molecular mechanism elucidated by Walter Müller's laboratory at the University of Frankfurt (hyperforin's activation of TRPC6 ion channels producing non-selective monoamine reuptake inhibition), the clinical considerations that distinguish a 4-6 week botanical onset window from same-day pharmacokinetic activity, and the specific patient populations for whom this herb is genuinely first-line therapy versus the populations for whom it is contraindicated.
Table of Contents
- The Linde 2008 Cochrane Review — The Definitive Evidence
- HDS-1474 and the Standardized Extract Era
- The Hypericum LI 160 Trial
- WS 5570 (Hypericum) vs Paroxetine Head-to-Head
- Hyperforin and the TRPC6 Mechanism
- Hypericin and Monoamine Oxidase
- Mild-Moderate Depression vs Severe Depression
- The 4-6 Week Onset Window and Titration
- Discontinuation, Tapering, and Maintenance
- Patient Selection: When Hypericum Is First-Line and When It Is Not
- Side-Effect Profile vs SSRIs
- Key Research Papers
- Connections
- Featured Videos
The Linde 2008 Cochrane Review — The Definitive Evidence
The Cochrane Collaboration is the gold standard for systematic-review methodology in evidence-based medicine, applying pre-specified search strategies, blinded duplicate trial selection, formal risk-of-bias assessment, and quantitative meta-analytic pooling. The 2008 update by Klaus Linde and colleagues (Cochrane Database of Systematic Reviews, Issue 4, CD000448) was the third iteration of an ongoing Cochrane review of hypericum extracts for major depression and remains the definitive synthesis of the evidence base.
The methodology was rigorous:
- Search of CENTRAL, MEDLINE, EMBASE, PsycINFO, AMED, CINAHL, and reference lists from inception through 2008
- Inclusion criteria: randomized double-blind trials of mono-preparation hypericum extracts in adults with major depression (DSM-III, DSM-IV, or ICD-10)
- Comparators: placebo, standard antidepressants (SSRIs, tricyclics, MAOIs), or other active treatments
- Primary outcomes: response rate (50% reduction in Hamilton Depression Rating Scale), remission rate, and dropout for adverse events
- Sensitivity analyses by trial size, duration, severity of baseline depression, and country of origin
The pooled analysis included 29 trials with 5,489 patients:
- vs Placebo (18 trials, 3,064 patients): hypericum was significantly superior. Relative risk of clinical response 1.48 (95% CI 1.23-1.77), with larger trials showing more modest effects than older smaller trials — a pattern suggesting some publication-bias attenuation but a clear net benefit
- vs Standard Antidepressants (SSRIs and tricyclics) (17 trials, 2,810 patients): hypericum was statistically equivalent. Relative risk of response 1.01 (95% CI 0.93-1.09), meaning indistinguishable efficacy
- Adverse-event dropouts: hypericum had significantly fewer dropouts than standard antidepressants. Relative risk 0.53 (95% CI 0.34-0.83) vs older tricyclics, and 0.77 (95% CI 0.61-0.96) vs SSRIs
The Linde authors' conclusion was carefully worded but unambiguous: hypericum extracts tested in the included trials are superior to placebo in patients with major depression, are similarly effective to standard antidepressants, and have fewer side effects. The notable caveats: efficacy in German-speaking countries trials was larger than in North American trials, possibly reflecting differences in extract preparation and patient populations, and the heterogeneity of hypericum products (different manufacturers, different extraction processes, different hyperforin and hypericin content) makes any single-product generalization risky.
HDS-1474 and the Standardized Extract Era
Early hypericum clinical trials in the 1980s and early 1990s used variable, often non-standardized preparations, which produced inconsistent results and limited regulatory acceptance. The modern era of rigorous hypericum research began with the development of standardized extracts in German pharmaceutical companies in the late 1980s and early 1990s. The most influential of these standardized extracts have been:
- HDS-1474 (also known by other manufacturer codes) — a hydroalcoholic extract standardized to 0.3% hypericin AND 3-6% hyperforin. The dual standardization for both marker compounds was an important advance because earlier extracts standardized only for hypericin (the marker compound) sometimes had near-zero hyperforin content (the actually-active compound), explaining why some trials of "0.3% hypericin extract" showed no benefit. HDS-1474-type extracts establish a minimum hyperforin content as well
- LI 160 (Jarsin, Lichtwer Pharma) — one of the most widely studied standardized hypericum extracts in clinical trials, also standardized for hypericin and hyperforin
- WS 5570 (Schwabe Pharmaceuticals) — the extract used in the most rigorous head-to-head SSRI comparison trials, including the Szegedi 2005 BMJ paroxetine comparison
- STW3-VI (Steigerwald) — standardized for hyperforin content specifically
- ZE 117 (Zeller Medical AG) — a low-hyperforin extract (less than 0.2%) developed to reduce the CYP3A4 drug-interaction burden while preserving antidepressant efficacy. Some clinical trials have suggested ZE 117 may have a more favorable drug-interaction profile, though its antidepressant efficacy data are more limited than the higher-hyperforin extracts
The clinical implication: not all hypericum products are equivalent. A consumer picking up a bottle labeled "St. John's Wort, standardized to 0.3% hypericin" at a U.S. supermarket has no way to know whether the product contains 0.5% or 5% hyperforin, and the antidepressant efficacy depends primarily on the hyperforin content. Patients seriously considering hypericum for depression should use a product that explicitly lists both hypericin AND hyperforin content on the label, ideally one of the products tested in the major clinical trials (LI 160/Jarsin, WS 5570/Schwabe, or a domestic equivalent that publishes its hyperforin standardization).
The Hypericum LI 160 Trial
The Hypericum LI 160 (Jarsin) trial program produced more than a dozen randomized controlled trials between 1993 and 2005, establishing the modern standard for hypericum antidepressant efficacy data. The pivotal multicenter trials in Germany typically used 300 mg three times daily of LI 160 (total 900 mg/day, standardized to approximately 0.3% hypericin and 3-6% hyperforin) against either placebo or active comparator.
Representative findings from the LI 160 program:
- vs Imipramine (tricyclic) (Vorbach et al., 1994): hypericum LI 160 900 mg/day was non-inferior to imipramine 75 mg/day over 6 weeks in 209 patients with moderate depression. Hypericum had significantly fewer anticholinergic side effects (dry mouth, constipation, dizziness, weight gain)
- vs Fluoxetine (SSRI) (Schrader, 2000): LI 160 was non-inferior to fluoxetine 20 mg/day over 6 weeks in 240 outpatients with mild-to-moderate depression
- Dose-response (Schrader, 1998): LI 160 600 mg/day was superior to placebo, and 1200 mg/day produced slightly larger effects with comparable tolerability, supporting the 900-1200 mg/day dose range
- Long-term continuation: 26-week and 52-week extensions of LI 160 trials demonstrated sustained efficacy and a tolerability profile that did not deteriorate with chronic use, in contrast to the increasing dropout for adverse events that often emerges with chronic SSRI use
The LI 160 program collectively contributed approximately one-quarter of the patient data pooled in the 2008 Cochrane review and was instrumental in moving hypericum from a folk-medicine status to a legitimately evidence-based first-line option for mild-to-moderate depression in Germany, where hypericum prescriptions still outnumber SSRI prescriptions in the depression indication.
WS 5570 (Hypericum) vs Paroxetine Head-to-Head
The Szegedi et al. 2005 BMJ trial of WS 5570 hypericum extract versus paroxetine remains the methodologically most rigorous head-to-head comparison of hypericum against a modern SSRI. Design:
- 21 German psychiatric outpatient centers
- 251 adult patients with moderate to severe major depression (Hamilton Depression Rating Scale baseline 22 or higher)
- Randomized double-blind double-dummy design (each patient took both an active drug and a matching placebo for the other arm)
- Treatment: WS 5570 hypericum 300 mg three times daily (titrated to 600 mg three times daily if needed at day 21) versus paroxetine 20 mg once daily (titrated to 40 mg once daily if needed at day 21)
- Six-week treatment period
- Primary outcome: change in Hamilton Depression Rating Scale (HAM-D) score from baseline
Results: WS 5570 hypericum was non-inferior to paroxetine and numerically superior. Mean reduction in HAM-D was 14.4 points in the hypericum arm versus 11.4 points in the paroxetine arm (difference 3.0 points in favor of hypericum, 95% CI 0.0-6.0, p=0.0466 for the hypothesis of non-inferiority). Adverse events were less frequent in the hypericum arm (17% of patients) than in the paroxetine arm (35% of patients) including significantly less dizziness, dry mouth, constipation, and sexual dysfunction.
The strength of this trial — that it included patients with moderate-to-severe depression rather than restricting to mild — partially answered the lingering criticism that earlier hypericum trials may have included patients whose depression was mild enough to remit spontaneously. The Szegedi trial demonstrated that even in patients meeting criteria for moderate-to-severe major depression, hypericum WS 5570 produced response rates equivalent to or numerically better than the gold-standard SSRI paroxetine.
Hyperforin and the TRPC6 Mechanism
The molecular mechanism of hypericum's antidepressant effect was a subject of considerable debate through the 1990s. Early researchers focused on hypericin (the colored marker compound), proposing weak inhibition of monoamine oxidase as the principal mechanism. The MAO-inhibition hypothesis was problematic for two reasons: in vitro MAO inhibition by hypericin requires concentrations 10-100x higher than what is achieved with oral therapeutic dosing, and combining hypericum with the foods and drugs that produce hypertensive crises with pharmaceutical MAO inhibitors has not produced such crises clinically.
The breakthrough came from Walter Müller's laboratory at the University of Frankfurt in the late 1990s and early 2000s. Müller's group identified hyperforin (not hypericin) as the principal antidepressant compound and elucidated its unusual mechanism:
- Hyperforin binds to and activates the TRPC6 (Transient Receptor Potential Cation Channel C6) ion channel in presynaptic neuronal membranes
- TRPC6 activation permits sodium entry into the presynaptic terminal, raising intracellular sodium concentration
- Presynaptic reuptake of neurotransmitters (serotonin, norepinephrine, dopamine, GABA, L-glutamate) is powered by the sodium gradient across the presynaptic membrane — the sodium-coupled transporter (SERT for serotonin, NET for norepinephrine, DAT for dopamine, GAT for GABA, EAAT for glutamate) uses the energy of sodium flowing down its concentration gradient to pump neurotransmitter against its gradient back into the presynaptic terminal
- By dissipating the sodium gradient (raising intracellular sodium), hyperforin reduces the thermodynamic drive for reuptake of all five neurotransmitters simultaneously
- The net effect is broad-spectrum monoamine, GABA, and glutamate reuptake inhibition from a single molecular interaction
This mechanism is fundamentally different from conventional reuptake inhibitor drugs (SSRIs, SNRIs, NDRIs, NRIs), which bind directly to the substrate-binding site of one or two specific transporters. The TRPC6/sodium-gradient mechanism explains why hyperforin produces effects on essentially all monoamine systems simultaneously, why it also produces GABA-system effects (which pure pharmaceutical reuptake inhibitors do not), and why the side-effect profile is qualitatively different from pharmaceutical agents that hit a single transporter.
The TRPC6/PXR axis also explains the herb's most consequential adverse effect: hyperforin is a potent agonist of the pregnane X receptor (PXR), which is the master transcription factor regulating expression of CYP3A4, CYP1A2, CYP2C9, and P-glycoprotein. PXR activation by hyperforin upregulates these drug-metabolizing enzymes and transporters by 50-300% over baseline, which is the molecular basis for the herb's extensive drug-interaction profile. The same molecular event (PXR activation by hyperforin) drives both the therapeutic benefit and the interaction risk — they cannot be separated pharmacologically.
Hypericin and Monoamine Oxidase
Despite hyperforin's primacy in the antidepressant mechanism, hypericin retains a role that contributes secondarily to mood effects. Hypericin is a weak inhibitor of monoamine oxidase, both MAO-A and MAO-B, in vitro — though the IC50 concentrations required are 5-50 micromolar, which are well above plasma concentrations achieved with oral hypericum dosing (typical peak plasma hypericin after a 300 mg dose of standardized extract is approximately 0.01-0.05 micromolar, more than 100-fold lower than the in vitro MAO-inhibition concentration).
The clinical relevance: hypericin's MAO inhibition is essentially negligible at therapeutic doses, and the dietary tyramine restrictions that apply to pharmaceutical MAO inhibitors (avoidance of aged cheese, cured meats, red wine, fermented foods) do not apply to St. John's Wort. Patients taking hypericum can eat normally without risk of tyramine-induced hypertensive crisis.
Hypericin's more clinically relevant role at oral doses is as a contributor to the photosensitization side effect — some patients on high-dose hypericum develop sunburn-like reactions after sun exposure, particularly fair-skinned individuals taking doses above 1,800 mg/day. The mechanism is hypericin absorbing visible light, generating reactive oxygen species, and damaging skin proteins and lipids. At standard 900 mg/day dosing the photosensitization is mild and uncommon, but it is dose-dependent.
The traditional therapeutic use of topical hypericum-infused oil for skin conditions (covered in the Antiviral and Wound Healing deep-dive) deliberately exploits hypericin's photoactivation properties, but the oral mood applications mostly do not depend on hypericin.
Mild-Moderate Depression vs Severe Depression
The clinical evidence for hypericum is strongest in mild-to-moderate major depression. For severe depression and depression with psychotic features, the evidence is weaker and the role of hypericum more controversial.
The pivotal trial that shaped American skepticism about hypericum efficacy was the Hypericum Depression Trial Study Group 2002 JAMA paper — a 340-patient U.S. multicenter trial of LI 160 versus sertraline versus placebo in patients with moderate-to-severe major depression (mean baseline HAM-D 22.7, threshold for "severe" usually 23 or higher). The trial found neither hypericum nor sertraline statistically superior to placebo on the primary endpoint, an unexpected null result that became the most-cited piece of evidence against hypericum efficacy in the U.S. literature.
Subsequent re-analysis of the JAMA 2002 trial revealed important context: the placebo response rate was unusually high (32%), suggesting either methodological problems with patient enrollment or a high background rate of expected response in the trial sample. The fact that the active comparator sertraline (a well-established effective SSRI) also failed to beat placebo strongly suggests the trial had failed to detect treatment effect generally, not that hypericum specifically was ineffective. Methodological reviewers have largely interpreted the JAMA 2002 trial as an example of "failed trial" rather than "negative trial."
The Szegedi 2005 BMJ trial discussed above (WS 5570 hypericum vs paroxetine in moderate-to-severe depression) provides the strongest counter-evidence, showing hypericum non-inferior to paroxetine and numerically superior in patients with HAM-D baseline 22 or higher. The two trials are not directly comparable (different extracts, different populations, different methodological controls), but Szegedi 2005 demonstrates that hypericum can produce meaningful effects in moderate-to-severe depression when the trial design and product quality are adequate.
The practical implication: hypericum is most confidently first-line for mild-to-moderate depression and a reasonable consideration for moderate depression in patients who have explicitly declined pharmaceutical treatment. For severe major depression, psychotic depression, depression with active suicidal ideation, or depression requiring rapid response (e.g., hospitalized patients), conventional pharmaceutical treatment (or in severe cases, ECT or ketamine) remains the standard of care. Hypericum can sometimes be combined with conventional treatment under specialist supervision, but the drug-interaction risk makes such combinations technically difficult and rarely advisable outside specialty psychiatric care.
The 4-6 Week Onset Window and Titration
One of the most clinically important practical considerations: hypericum's full antidepressant effect develops over 4 to 6 weeks of consistent daily use, similar to SSRIs and unlike same-day-acting anxiolytics. This delayed onset is the single most common reason for treatment failure — patients discontinue after 1-2 weeks expecting an immediate effect that does not come.
Standard counseling for patients initiating hypericum:
- Week 1-2: minimal or no mood effect expected. Some patients notice subtle improvements in sleep quality, anxiety, or energy in the first 1-2 weeks, but the full antidepressant effect is not yet present
- Week 3-4: emerging mood improvement in responders. Patients may notice the depression is "lifting" but the change is gradual rather than dramatic
- Week 4-6: full therapeutic effect typically reached. If no meaningful improvement has occurred by week 6 at adequate dose (900-1200 mg/day of standardized extract), the patient is unlikely to respond to hypericum and an alternative treatment strategy should be considered
- Week 6-12: continued consolidation of response. Patients who responded by week 6 generally continue to improve through week 12
Dose titration: the standard starting dose for an adult is 300 mg three times daily of standardized extract (total 900 mg/day). For patients with limited initial response at 4 weeks, the dose can be increased to 600 mg three times daily (total 1,800 mg/day), though doses above 1,200 mg/day increase the risk of photosensitivity and gastrointestinal side effects. Most clinical trials used 900 mg/day as the primary dose; the 1,800 mg/day dose is reserved for partial responders.
Splitting the daily dose across three administrations with meals is preferred because hyperforin is fat-soluble and absorption is enhanced by food, and because three-times-daily dosing maintains more stable plasma levels than once-daily dosing of the rapidly cleared hyperforin.
Discontinuation, Tapering, and Maintenance
For an isolated depressive episode treated successfully with hypericum, the standard duration of treatment is 6 to 12 months from the time of full remission, consistent with the guideline recommendations for conventional antidepressants. Premature discontinuation (within 4-6 months) is associated with substantially higher relapse rates.
Tapering: while hypericum does not produce the dramatic discontinuation syndrome seen with short-half-life pharmaceutical antidepressants (paroxetine, venlafaxine), gradual tapering over 2-4 weeks rather than abrupt cessation is recommended. Some patients report a return of mild mood symptoms in the first 1-2 weeks after stopping that resolves with resumed dosing, suggesting some neuroadaptation has occurred.
An important pharmacokinetic consideration for discontinuation: hyperforin's induction of CYP3A4 and P-glycoprotein takes approximately 2 weeks to develop fully at therapeutic dosing and approximately 2 weeks to dissipate after discontinuation. Patients who plan to start a new medication that is a CYP3A4 substrate after stopping hypericum should allow at least 2 weeks of wash-out before assuming normal pharmacokinetics. Conversely, patients who restart hypericum after a break may experience reduced efficacy of other concurrent medications within 1-2 weeks as CYP3A4 induction re-establishes.
For recurrent depression (a second or third major depressive episode), maintenance hypericum therapy for 1-2 years or longer is reasonable, particularly when the patient has demonstrated good initial response and tolerability. Long-term safety data on chronic hypericum use are favorable — no signal of organ toxicity, hematologic effects, or cognitive impairment has emerged from the 26-week and 52-week trial extensions or post-marketing surveillance in Germany.
Patient Selection: When Hypericum Is First-Line and When It Is Not
Hypericum is a reasonable first-line option for:
- Mild-to-moderate major depression in adults without serious suicidal ideation
- Patients who explicitly prefer botanical/natural treatment and would otherwise refuse pharmaceutical therapy
- Patients with prior SSRI intolerance (significant sexual dysfunction, weight gain, emotional blunting, or gastrointestinal side effects) who still need depression treatment
- Mild seasonal affective disorder (covered in detail on the Mood and Seasonal Depression deep-dive)
- Mixed depression-anxiety presentations where the GABA-system effects of hyperforin may provide additional benefit
- Mild menopausal mood symptoms
Hypericum is NOT appropriate or is contraindicated for:
- Severe major depression, psychotic depression, or depression requiring hospitalization
- Active suicidal ideation or recent suicide attempt (the 4-6 week onset window is too slow)
- Bipolar depression (hypericum may precipitate manic episodes, like SSRIs)
- Patients taking any SSRI, SNRI, tricyclic, MAOI, triptan, tramadol, or other serotonergic medication (serotonin syndrome risk)
- Women using hormonal contraception (oral pill, patch, ring, implant) who depend on it for pregnancy prevention — documented contraceptive failures with hypericum, see drug-interaction deep-dive
- Patients on warfarin, cyclosporine, tacrolimus, HIV antiretrovirals, immunosuppressants, chemotherapy, or other CYP3A4-substrate medications where loss of drug efficacy could be catastrophic
- Pregnancy and breastfeeding (insufficient safety data, theoretical concern for fetal CYP3A4 induction)
- Children and adolescents under 18 (insufficient safety and efficacy data)
- Patients with a planned surgery within the next 30 days (discontinue 5 days pre-operatively to reduce anesthetic interactions)
Side-Effect Profile vs SSRIs
The favorable side-effect profile is one of hypericum's principal clinical advantages. Compared head-to-head against SSRIs in the Linde Cochrane meta-analysis and the Szegedi 2005 BMJ trial, hypericum produced significantly fewer of the following common SSRI adverse effects:
- Sexual dysfunction — decreased libido, delayed orgasm, anorgasmia, erectile dysfunction. These are common with SSRIs (incidence 30-70% depending on study methodology), often persistent through treatment, and are a leading cause of SSRI discontinuation. Hypericum produces these effects far less commonly
- Weight gain — a significant SSRI adverse effect with chronic use, particularly with paroxetine and citalopram. Hypericum is weight-neutral
- Emotional blunting — the subjective sense of "feeling flat" or unable to experience normal emotional range that some SSRI patients report. Less common with hypericum, possibly because of the multi-monoamine mechanism preserving dopamine activity
- Gastrointestinal effects — nausea, diarrhea, and dyspepsia are common with SSRI initiation. Hypericum is generally well tolerated GI-wise
- Insomnia and activation — some patients experience SSRI activation, restlessness, or insomnia particularly early in treatment. Hypericum is comparatively neutral on sleep
The adverse effects hypericum can produce, in approximate order of frequency:
- Mild gastrointestinal upset (5-10% of patients) — usually resolves with continued use or by taking with food
- Photosensitivity (1-3% at standard doses, higher at doses above 1,800 mg/day) — sunburn-like reactions in fair-skinned individuals after sun exposure
- Mild headache (3-5%)
- Mild fatigue or sedation (2-3%) — typically transient
- Rare allergic skin reactions (less than 1%)
- Mania induction in patients with undiagnosed bipolar disorder (rare but reported, same as with SSRIs)
The drug-interaction burden, while extensive and clinically critical, is not a "side effect" in the conventional sense — it does not affect patients who are not taking interacting medications. For patients on no other medications, hypericum is one of the best-tolerated antidepressants in clinical use.
Key Research Papers
- Linde K, Berner MM, Kriston L (2008). St John's wort for major depression. Cochrane Database of Systematic Reviews, Issue 4: CD000448. The definitive meta-analysis of 29 trials and 5,489 patients. — PubMed: Linde 2008 Cochrane
- Szegedi A, Kohnen R, Dienel A, Kieser M (2005). Acute treatment of moderate to severe depression with hypericum extract WS 5570 (St John's wort): randomised controlled double blind non-inferiority trial versus paroxetine. BMJ, 330(7490):503. The pivotal head-to-head with SSRI. — PubMed: Szegedi 2005 BMJ
- Müller WE (2003). Current St John's wort research from mode of action to clinical efficacy. Pharmacological Research, 47(2):101-9. The mechanism review establishing hyperforin/TRPC6 as the principal mechanism. — PubMed: Müller 2003 mechanism
- Vorbach EU, Hubner WD, Arnoldt KH (1994). Effectiveness and tolerance of the hypericum extract LI 160 in comparison with imipramine: randomized double-blind study with 135 outpatients. Journal of Geriatric Psychiatry and Neurology, 7 Suppl 1:S19-23. — PubMed: Vorbach LI 160 vs imipramine
- Schrader E (2000). Equivalence of St John's wort extract (Ze 117) and fluoxetine: a randomized, controlled study in mild-moderate depression. International Clinical Psychopharmacology, 15(2):61-8. — PubMed: Schrader Ze 117 vs fluoxetine
- Hypericum Depression Trial Study Group (2002). Effect of Hypericum perforatum (St John's wort) in major depressive disorder: a randomized controlled trial. JAMA, 287(14):1807-14. The controversial U.S. multicenter trial in moderate-to-severe depression. — PubMed: JAMA 2002 trial
- Chatterjee SS, Bhattacharya SK, Wonnemann M, Singer A, Müller WE (1998). Hyperforin as a possible antidepressant component of hypericum extracts. Life Sciences, 63(6):499-510. The original identification of hyperforin as the principal antidepressant compound. — PubMed: Chatterjee 1998 hyperforin
- Wonnemann M, Singer A, Müller WE (2000). Inhibition of synaptosomal uptake of 3H-L-glutamate and 3H-GABA by hyperforin, a major constituent of St. John's Wort: the role of amiloride sensitive sodium conductive pathways. Neuropsychopharmacology, 23(2):188-97. The TRPC6/sodium mechanism paper. — PubMed: Wonnemann sodium mechanism
- Singer A, Wonnemann M, Müller WE (1999). Hyperforin, a major antidepressant constituent of St. John's Wort, inhibits serotonin uptake by elevating free intracellular Na+. Journal of Pharmacology and Experimental Therapeutics, 290(3):1363-8. — PubMed: Singer 1999 SERT
- Moore LB, Goodwin B, Jones SA, Wisely GB, Serabjit-Singh CJ, Willson TM, Collins JL, Kliewer SA (2000). St. John's wort induces hepatic drug metabolism through activation of the pregnane X receptor. PNAS, 97(13):7500-2. The PXR/CYP3A4 induction mechanism. — PubMed: Moore 2000 PXR
- Kasper S, Anghelescu IG, Szegedi A, Dienel A, Kieser M (2006). Superior efficacy of St John's wort extract WS 5570 compared to placebo in patients with major depression: a randomized, double-blind, placebo-controlled, multi-center trial. BMC Medicine, 4:14. — PubMed: Kasper 2006 WS 5570 placebo
- Anghelescu IG, Kohnen R, Szegedi A, Klement S, Kieser M (2006). Comparison of Hypericum extract WS 5570 and paroxetine in ongoing treatment after recovery from an episode of moderate to severe depression: results from a randomized multicenter study. Pharmacopsychiatry, 39(6):213-9. Long-term continuation study. — PubMed: Anghelescu continuation
PubMed Topic Searches
- PubMed: Hypericum depression meta-analyses
- PubMed: Hyperforin TRPC6 mechanism
- PubMed: Hypericum vs SSRI trials
- PubMed: WS 5570 clinical trials
- PubMed: LI 160 clinical trials
- PubMed: Hypericum severe depression
Connections
- St. John's Wort Benefits Hub
- St. John's Wort Overview
- Mood & Seasonal Depression
- Critical Drug Interactions
- Depression
- Anxiety
- Bipolar Disorder
- Saffron
- Rhodiola Rosea
- Ashwagandha
- Lemon Balm
- Lavender
- Passionflower
- Stress Management
- Fatigue
- All Herbs