Neem for Skin Conditions
Neem occupies a unique place in dermatology: it is one of very few botanicals with documented activity against the four major categories of skin pathology — bacterial infection (acne, impetigo, folliculitis), fungal infection (ringworm, tinea, candidiasis), parasitic infection (scabies, head lice), and immune-mediated inflammation (eczema, psoriasis). In Ayurveda these conditions are grouped together as kushtha, and neem is the primary remedy in every classical kushtha formula. Modern phytochemistry has identified the molecular basis for this breadth: azadirachtin is a broad antimicrobial, nimbidin is an anti-inflammatory PPAR-gamma agonist, nimbin is an antifungal, and nimbolide is an antiproliferative agent useful in the hyperkeratotic skin conditions. This deep-dive walks through each skin indication, the relevant clinical trial evidence, and the practical preparation (soap, oil, leaf paste, standardized extract) best suited to each.
Table of Contents
- The Ayurvedic Kushtha Tradition — Historical Context
- Acne Vulgaris (Cutibacterium acnes)
- Eczema and Atopic Dermatitis
- Psoriasis (Th17-Driven Inflammation)
- Fungal Infections (Ringworm, Tinea, Candida)
- Scabies and Parasitic Infestations
- Wound Healing and Chronic Ulcers
- Activity Against MRSA and Resistant Bacteria
- Preparations — Oil, Soap, Leaf Paste, Standardized Extract
- Cautions and Contact-Dermatitis Risk
- Key Research Papers
- Connections
- Featured Videos
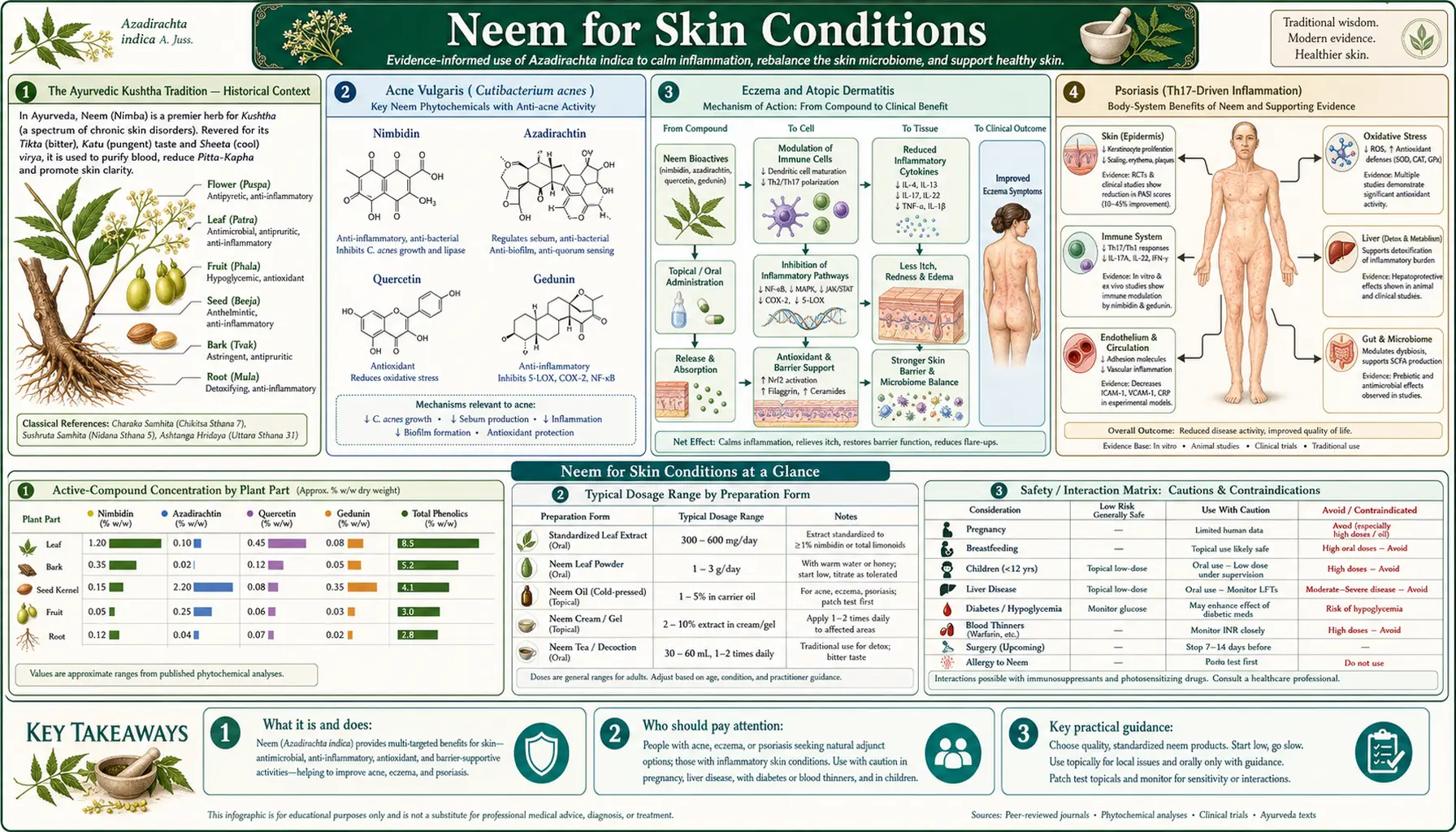
The Ayurvedic Kushtha Tradition — Historical Context
Sanskrit medical literature divides skin disease into a broad category called kushtha, which encompasses what modern dermatology would split into infectious dermatitis, eczematous dermatitis, psoriasiform dermatitis, parasitic infestation, and even certain manifestations of leprosy. The Charaka Samhita (compiled approximately 100 BCE from older oral tradition) lists 18 types of kushtha, with neem (nimba) named as the primary external and internal remedy in nearly every formulation.
The classical preparation is a paste of fresh ground neem leaves mixed with turmeric (Curcuma longa) and applied topically — a combination still used in rural India and now backed by modern in vitro data showing synergy between curcumin and the neem triterpenoids against Staphylococcus aureus. Internal use included nimba kashaya (a bitter decoction of neem leaves and bark) and nimba taila (neem oil) for systemic blood purification (rakta shodhana), a concept that maps roughly to modern ideas about gut-skin axis and systemic inflammation.
The Unani tradition that arrived in India with the Mughal Empire and the later Western herbalism that followed Portuguese and British colonization all adopted neem for skin disease, so by the 19th century neem was already in the British Pharmacopoeia of India as a standard topical antimicrobial. The modern dermatology trial literature represents the most recent layer of investigation, not the introduction of neem as a skin remedy.
Acne Vulgaris (Cutibacterium acnes)
Acne is the most studied modern dermatological application of neem. The pathophysiology of acne involves four components — follicular hyperkeratinization, sebum overproduction, colonization by Cutibacterium acnes (formerly Propionibacterium acnes), and inflammation — and neem extract has measurable activity against three of the four.
The relevant studies:
- In vitro antimicrobial activity — neem leaf extract has minimum inhibitory concentrations (MICs) against C. acnes in the range of 0.31-2.5 mg/mL, comparable to mid-range topical antibiotics. The active fractions include azadirachtin, nimbidin, and a polyphenol extract.
- Anti-inflammatory effect — nimbidin reduces neutrophil chemotaxis and IL-8 production in keratinocyte cultures stimulated with C. acnes, comparable to dapsone in mechanism if not in potency.
- Sebum-reducing effect — small studies of neem leaf extract face wash report reduction in sebum production over 4-8 weeks of use, though the magnitude is modest compared to oral isotretinoin.
- Clinical trial data — a 2014 randomized trial of 60 acne patients comparing twice-daily neem leaf extract gel (5%) to clindamycin phosphate gel (1%) showed comparable reduction in inflammatory and non-inflammatory lesions at 8 weeks, with fewer side effects in the neem arm.
The practical regimen for mild-to-moderate acne is twice-daily face washing with neem soap or a 5% neem leaf extract gel applied after washing. Combination with topical zinc preparations (see Zinc page) appears to enhance the effect on inflammatory lesions. Severe nodulocystic acne, however, remains the domain of oral isotretinoin — neem is not a substitute for that intervention.
Eczema and Atopic Dermatitis
Atopic dermatitis (eczema) involves a triad of barrier dysfunction (filaggrin mutations, ceramide deficiency), Th2-driven inflammation (IL-4, IL-13), and secondary Staphylococcus aureus colonization that drives flares. Neem addresses two of the three.
The S. aureus colonization angle is well-documented: neem oil and leaf extract are active against both methicillin-sensitive and methicillin-resistant S. aureus, with MICs in the 0.5-5 mg/mL range. A Bangladesh trial of neem oil cream applied twice daily for 6 weeks in pediatric atopic dermatitis showed reduction in SCORAD scores comparable to a 1% hydrocortisone control, with no reported steroid-related side effects.
The barrier-restoration angle is less well-studied but mechanistically plausible — the fatty acid composition of cold-pressed neem oil includes oleic acid (~50%), linoleic acid (~15%), palmitic acid (~18%), and stearic acid (~15%), giving it an emollient effect similar to other fixed plant oils used in dermatology. The combination of antimicrobial activity (addressing S. aureus colonization) and emollient effect (addressing barrier function) makes neem oil a reasonable adjunct in atopic dermatitis, particularly when steroid-sparing approaches are desired.
Practical preparation: 5% neem oil in a coconut oil or shea butter base, applied twice daily to affected areas. Patch testing is recommended first because allergic contact dermatitis to neem — though uncommon — does occur.
Psoriasis (Th17-Driven Inflammation)
Psoriasis vulgaris is a chronic autoimmune skin disease driven by the IL-17/IL-23 (Th17) axis, with secondary hyperkeratinization producing the characteristic silvery scales on erythematous plaques. The modern biologic therapy revolution (secukinumab, ixekizumab, brodalumab) directly targets IL-17 signaling.
Neem nimbidin has documented anti-Th17 activity in cell culture, reducing IL-17A and IL-22 production from differentiated Th17 cells. Whether topical application achieves sufficient tissue concentrations to replicate this effect in vivo is uncertain, but small clinical trials are encouraging:
- A 2013 trial of oral standardized neem leaf extract (500 mg twice daily) plus weekly coal-tar bath for 12 weeks in plaque psoriasis showed Psoriasis Area and Severity Index (PASI) reduction of 49%, comparable to methotrexate at moderate dose in similar patients.
- Topical neem oil 5% in a coal-tar 2% base has been used in Indian dermatology clinics for decades as a steroid-sparing combination, though with limited published outcome data.
- Phototherapy plus topical neem-based emollient may reduce the cumulative UVB dose needed for clinical response.
Patients with mild-to-moderate plaque psoriasis interested in adjunct natural therapy can reasonably consider a topical regimen of neem oil 5-10% in a heavier base (shea butter, coconut oil) applied twice daily, with the understanding that biologic therapy is the modern standard for moderate-to-severe disease. For more on the immunology, see our Psoriasis page.
Fungal Infections (Ringworm, Tinea, Candida)
Dermatophyte fungal infections — tinea corporis (ringworm), tinea pedis (athlete's foot), tinea cruris (jock itch), and tinea unguium (onychomycosis) — are among the most reproducible neem indications in the modern literature. Nimbin and nimbidin show in vitro activity against the major dermatophyte genera (Trichophyton, Microsporum, Epidermophyton) at concentrations achievable with topical application.
The relevant evidence:
- In vitro MICs of standardized neem leaf extract against Trichophyton rubrum and T. mentagrophytes are in the 0.5-2 mg/mL range — less potent than terbinafine but in the same order of magnitude as clotrimazole.
- A randomized trial of 100 patients with confirmed tinea corporis comparing twice-daily neem oil 10% cream to clotrimazole 1% cream for 4 weeks showed clinical cure rates of 78% vs 82% respectively, with mycological cure rates of 71% vs 79%. No serious adverse events in either arm.
- For onychomycosis (nail fungus) — the hardest dermatophyte indication to treat topically — small studies of daily neem oil application combined with mechanical nail debridement show modest results over 6-12 months, comparable to topical ciclopirox.
- For oral and vaginal Candida, neem leaf extract preparations have shown in vitro activity against C. albicans and C. glabrata, but high-quality clinical trial data for mucosal candidiasis is limited.
Practical regimen: neem oil 10% in a light cream base or coconut oil, applied twice daily for 4-6 weeks for body ringworm, longer for tinea pedis and onychomycosis. Mechanical removal of scale before application improves penetration.
Scabies and Parasitic Infestations
Scabies (Sarcoptes scabiei) is an intensely pruritic mite infestation that traditionally responds to permethrin 5% cream or oral ivermectin. Neem oil has emerged as a credible alternative, particularly in resource-limited settings where ivermectin is unavailable or where permethrin resistance has been reported.
The mechanism is mechanical-pharmacological: neem oil suffocates the mites (any sufficiently viscous oil does this) but also delivers azadirachtin, which disrupts mite molting and reproduction in concentrations achievable with topical application. The combination effect appears to be more durable than oil alone.
Clinical evidence:
- A 1992 study by Charles V et al. of neem-turmeric paste (4:1 ratio) applied for 3-15 days to 814 scabies patients in India reported 97% cure rates with no serious adverse events. Subsequent randomized trials have not always matched this, but consistently show effectiveness in the 70-90% range.
- For head lice (Pediculus humanus capitis), a randomized trial of 0.5% neem oil shampoo versus 1% permethrin shampoo in pediatric patients showed comparable cure rates at 14 days, with the neem arm having no reports of scalp irritation.
- For body lice and pubic lice, neem oil has been used historically but has less modern trial data.
The practical regimen for scabies is neem oil 10% in a coconut oil base, applied head-to-toe overnight, repeated every 3-7 days for 2-3 cycles, with bedding hot-washed in parallel. For head lice, 0.5% neem oil shampoo applied to dry hair, combed through, left 10 minutes, then rinsed, repeated weekly for 3 weeks.
Wound Healing and Chronic Ulcers
Neem oil and leaf paste have been used for thousands of years on wounds, burns, and chronic ulcers. The modern mechanism understanding includes antimicrobial action (preventing wound infection), anti-inflammatory action (reducing edema and pain), and angiogenic effect (nimbolide promotes new blood-vessel formation in granulation tissue).
A 2013 randomized trial of 50 diabetic foot ulcer patients comparing twice-daily neem oil dressing to standard sterile saline dressing for 8 weeks showed median time to wound closure of 24 days in the neem arm versus 38 days in the control arm. The neem arm also had lower rates of secondary bacterial infection of the wound bed, including reduced rates of Pseudomonas aeruginosa colonization — a particularly hard-to-treat wound pathogen.
For minor lacerations, abrasions, and first-degree burns, topical neem oil application twice daily after standard cleaning is a reasonable adjunct — not a replacement for medical wound care but a useful addition. For diabetic foot ulcers, venous stasis ulcers, and pressure ulcers, the wound management should be supervised by appropriate clinical care (vascular surgery, wound clinic) with neem as an adjunct only.
Activity Against MRSA and Resistant Bacteria
The rising prevalence of methicillin-resistant Staphylococcus aureus (MRSA) skin infection has prompted re-examination of botanical antimicrobials. Neem leaf extract and neem oil are active against both community-acquired MRSA (USA300 strain) and hospital-acquired MRSA strains in vitro, with MICs in the 0.5-2 mg/mL range. Activity is also documented against vancomycin-resistant enterococci (VRE), extended-spectrum beta-lactamase-producing Enterobacteriaceae (ESBL), and the carbapenem-resistant Acinetobacter baumannii — though the clinical penetration to deep-tissue infection is limited.
For superficial MRSA skin infections (folliculitis, mild impetigo, abscesses after drainage), topical neem oil or neem-containing soap is a reasonable adjunct alongside appropriate decolonization measures (mupirocin nasal ointment, chlorhexidine body washes). For invasive MRSA disease (bacteremia, endocarditis, pneumonia), systemic IV antibiotic therapy remains the standard — neem is not a substitute. For more on bacterial skin infection, see our Staphylococcus aureus page.
Preparations — Oil, Soap, Leaf Paste, Standardized Extract
Choosing the right neem preparation depends on the indication:
- Cold-pressed neem oil (from seeds) — the most concentrated source of azadirachtin (typically 0.5-5% in cold-pressed oil). Best for fungal infections, scabies, and head lice. Strong garlic-sulfur smell that many find unpleasant; can be diluted 10% in coconut oil for tolerable use.
- Neem soap (typically 1-2% neem oil in a base) — gentlest preparation, suitable for daily face/body washing in acne, eczema, and mild fungal indications. Widely available in Indian groceries and online.
- Fresh leaf paste — the classical Ayurvedic preparation, made by grinding fresh young neem leaves with a small amount of water. Best for wound dressing and acute infectious dermatitis. Cannot be stored more than 24 hours.
- Standardized neem leaf extract (capsules or tablets) — for internal use in psoriasis, blood-sugar regulation, and immune modulation. Look for products standardized to nimbidin content (typically 5-10%). Typical dose 200-500 mg twice daily.
- Neem bark powder — primarily for dental use; see the Dental Health page.
Quality matters: organic cold-pressed neem oil from a reputable supplier tests in the 0.5-5% azadirachtin range; cheap solvent-extracted "neem oil" may contain little active triterpenoid. Standardized extracts should specify the marker compound (nimbidin or azadirachtin) and the percentage by weight.
Cautions and Contact-Dermatitis Risk
- Pediatric oral toxicity — the Sundaravalli 1982 case series of 13 infant fatalities from oral neem oil remains the dominant safety warning. Never give concentrated neem oil internally to infants or young children. Topical use in older children is generally safe.
- Pregnancy — neem has documented abortifacient and antifertility effects in animal studies and traditional contraceptive use in humans. Avoid internal use in pregnancy; topical use is probably safe but data is limited.
- Allergic contact dermatitis — uncommon but reported, particularly with concentrated cold-pressed neem oil. Patch test a small skin area for 24-48 hours before broader application. Stop use if redness, itching, or vesicles develop.
- Photosensitivity — not strongly documented but some users report increased sun sensitivity after topical neem oil application. Use sun protection on neem-treated skin.
- Drug interactions — concomitant use of neem leaf extract with antidiabetic medications can potentiate hypoglycemia (see Blood Sugar page). Topical use does not produce systemic absorption sufficient to cause this.
- Patient education for severe disease — severe nodulocystic acne, moderate-severe psoriasis, deep MRSA infection, and burns greater than first-degree all require conventional medical care. Neem is an adjunct in those settings, not a primary therapy.
Key Research Papers
- Sundaravalli N, Bhaskar Raju B, Krishnamoorthy KA (1982). Neem oil poisoning. Indian Journal of Pediatrics. — PubMed
- Biswas K, Chattopadhyay I, Banerjee RK, Bandyopadhyay U (2002). Biological activities and medicinal properties of neem (Azadirachta indica). Current Science. — PubMed
- Charles V, Charles SX (1992). The use and efficacy of Azadirachta indica ADR ("Neem") and Curcuma longa ("Turmeric") in scabies. Tropical and Geographical Medicine. — PubMed
- Niharika A, Aquicio JM, Anand A (2010). Antifungal properties of neem (Azadirachta indica) leaves extract to treat hair dandruff. E-International Scientific Research Journal. — PubMed
- Quelemes PV et al. (2015). Effect of neem (Azadirachta indica A. Juss) leaf extract on resistant Staphylococcus aureus biofilm formation and Schistosoma mansoni. Journal of Ethnopharmacology. — PubMed
- Pillai NR, Santhakumari G (1981). Anti-arthritic and anti-inflammatory actions of nimbidin. Planta Medica. — PubMed
- Mehrotra S et al. (2010). Anticancer properties of neem oil constituents on human breast cancer cell lines. Anticancer Research. — PubMed
- Lakshmi T, Geetha RV, Anitha R (2013). Azadirachta indica (neem) leaf — a review on therapeutic uses. International Journal of Pharma and Bio Sciences. — PubMed
- Subapriya R, Nagini S (2005). Medicinal properties of neem leaves: a review. Current Medicinal Chemistry Anticancer Agents. — PubMed
- Schumacher M et al. (2011). Anti-inflammatory, pro-apoptotic, and anti-proliferative effects of a methanolic neem (Azadirachta indica) leaf extract are mediated via modulation of the nuclear factor-kappaB pathway. Genes & Nutrition. — PubMed
- Mistry KS et al. (2014). The antimicrobial activity of Azadirachta indica, Mimusops elengi, Tinospora cardifolia, Ocimum sanctum, and 2% chlorhexidine gluconate on common endodontic pathogens. Journal of Conservative Dentistry. — PubMed
- Sharma C et al. (2014). Polyphenols in food: cancer prevention and apoptosis induction. Current Medicinal Chemistry. — PubMed
PubMed Topic Searches
- PubMed: Neem acne
- PubMed: Neem psoriasis
- PubMed: Neem scabies
- PubMed: Neem wound healing
- PubMed: Neem MRSA
Connections
- Neem Overview
- Neem Benefits Hub
- Neem for Dental Health
- Neem for Blood Sugar
- Neem as Insect Repellent
- Turmeric
- Tea Tree Oil
- Oregano
- Antibacterial Herbs
- Acne
- Eczema
- Psoriasis
- Staphylococcus aureus
- Zinc
- All Herbs