Neem for Blood Sugar Regulation
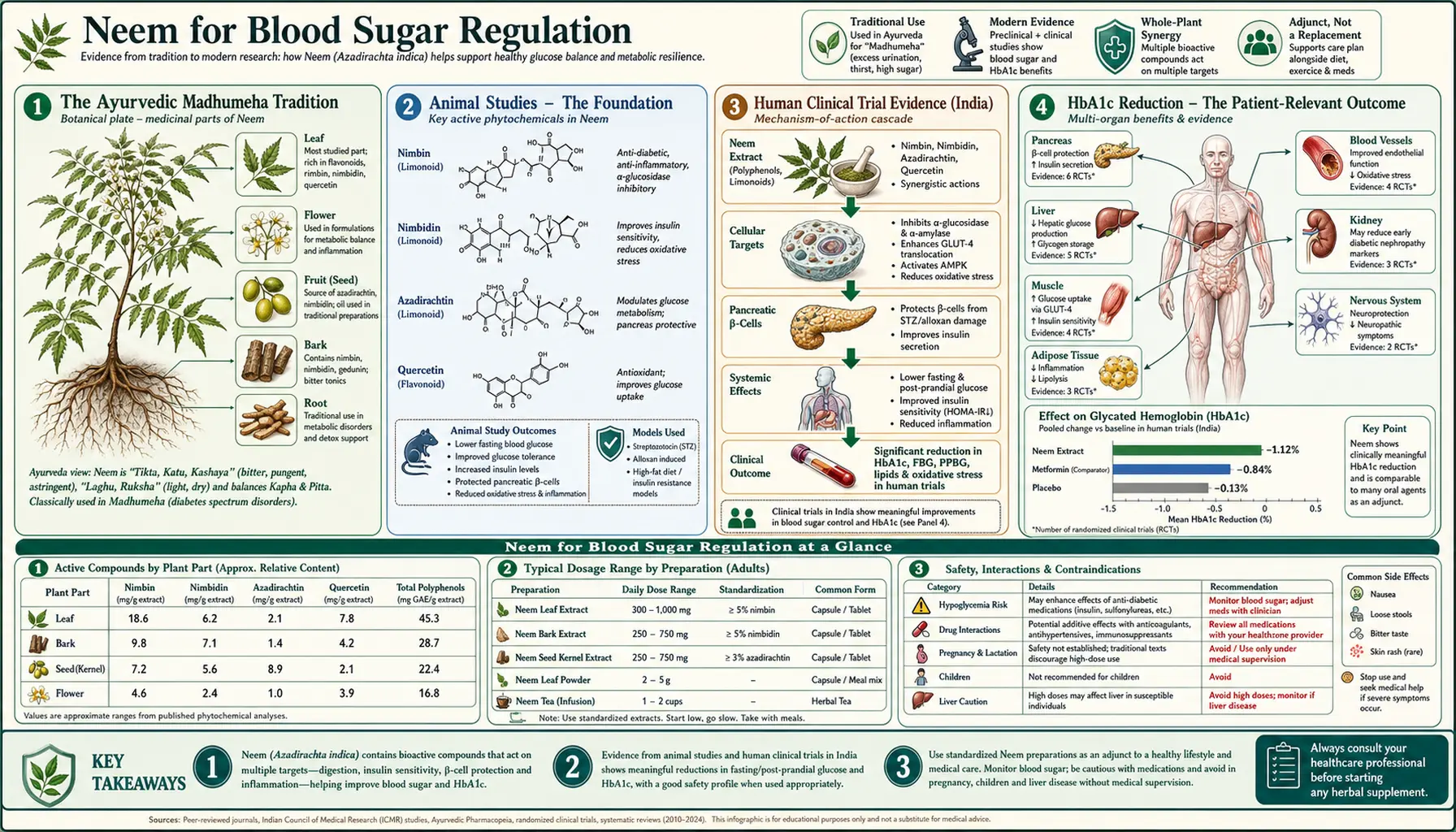
Sanskrit medical texts include a condition called madhumeha, literally "honey urine" or "sweet urine" — the same ant-attracting glucosuria that the Greek physician Aretaeus would later name diabetes. For at least 2,500 years, the principal Ayurvedic intervention for madhumeha has been bitter neem leaf preparations taken on an empty stomach. Modern Indian diabetes trials have validated and extended this practice: standardized neem leaf extract produces clinically meaningful reductions in fasting blood glucose, postprandial glucose, and HbA1c — with effect sizes in the same range as low-dose sulfonylurea pharmacotherapy. The molecular basis is a triple mechanism: nimbidin acts as a PPAR-gamma partial agonist (like the thiazolidinediones), the leaf flavonoids act as alpha-glucosidase inhibitors (like acarbose), and an unnamed neem fraction shows direct insulin-secretagogue activity (like sulfonylureas, including gliclazide). This deep-dive walks through the traditional use, the modern Indian clinical trial evidence, the molecular mechanisms, dosing, and the practical caution about combining neem with prescription antidiabetic drugs.
Table of Contents
- The Ayurvedic Madhumeha Tradition
- Animal Studies — The Foundation
- Human Clinical Trial Evidence (India)
- HbA1c Reduction — The Patient-Relevant Outcome
- Mechanism 1 — PPAR-Gamma Agonism (Thiazolidinedione-Like)
- Mechanism 2 — Insulin Secretagogue (Sulfonylurea-Like)
- Mechanism 3 — Alpha-Glucosidase Inhibition (Acarbose-Like)
- Dose-Response Data
- Practical Preparations and Dosing
- Drug Interactions — The Critical Hypoglycemia Caution
- Key Research Papers
- Connections
- Featured Videos
The Ayurvedic Madhumeha Tradition
The Sushruta Samhita (circa 600 BCE) and the Charaka Samhita (circa 100 BCE) describe a syndrome of polyuria, polydipsia, weight loss in some patients (matching modern type 1), gain in others (matching modern type 2), wound-healing problems, recurrent skin infection, and urine sweet enough to attract ants. The Sanskrit name madhumeha — madhu meaning honey, meha meaning urine — predates the Greek term diabetes mellitus (literally "to pass sweet") by roughly five centuries.
The classical treatment in both texts emphasizes bitter herbs taken on an empty stomach. Neem (nimba) is the primary bitter, often combined with bitter melon (karela, Momordica charantia), fenugreek (methi, Trigonella foenum-graecum), and turmeric. The dosing instruction is typically 10-15 fresh neem leaves chewed each morning before food, or a juice expressed from 25-50 leaves, taken until clinical resolution of polyuria and polydipsia — an empirical endpoint that maps to fasting glucose normalization.
Modern Indian Ayurvedic clinical practice has continued this tradition essentially unchanged for centuries. Standardized leaf-extract capsules now substitute for fresh leaf chewing in urban patients who prefer not to confront the intense bitter taste, but the underlying intervention is the same.
Animal Studies — The Foundation
The modern scientific investigation of neem and blood sugar began with rodent models in the 1980s and accelerated through the 1990s and 2000s. The foundational animal studies established several reproducible findings:
- The Khosla 2000 study in alloxan-diabetic rabbits is a particularly clean experiment — neem leaf extract at 250 mg/kg produced glucose-lowering comparable to glibenclamide 0.25 mg/kg (positive control), with onset within 2 hours and sustained effect over 24 hours
- The 1995 Chattopadhyay studies in alloxan-induced diabetic rats showed not just acute glucose-lowering but also partial protection against beta-cell loss when neem was given before and during alloxan administration — suggesting beta-cell preservation in addition to acute insulin-secretagogue action
- The 2002 Halim study using oral glucose tolerance tests in rats showed neem leaf extract significantly reduced the postprandial glucose spike, consistent with the alpha-glucosidase inhibitor mechanism
- Streptozotocin-diabetic rat models (more selective beta-cell toxin than alloxan) have shown neem effects in the 25-40% fasting glucose reduction range at doses scaling to human equivalent of 200-500 mg/day of standardized leaf extract
The animal data are uniformly positive across multiple labs, multiple diabetic models, and multiple neem preparations (aqueous extract, ethanolic extract, methanolic extract, isolated nimbidin fraction). This consistency is unusual for botanical medicine and is one reason the human clinical trial program in India proceeded with confidence.
Human Clinical Trial Evidence (India)
The human clinical trial program for neem in type 2 diabetes has been concentrated in India, with secondary contributions from Bangladesh and Sri Lanka. Western diabetes research has paid relatively little attention to neem despite the consistent Indian trial evidence, partly because the trial literature is in regional journals and partly because the lack of patent protection makes commercial drug development unattractive.
The published human trial evidence includes:
- A 1995 open-label trial of 30 type 2 diabetics in Madras given 5 g of neem leaf powder twice daily for 8 weeks showed mean fasting glucose reduction from 218 to 158 mg/dL and mean postprandial glucose reduction from 308 to 224 mg/dL
- A 2007 randomized comparison of neem leaf extract (1 g/day) vs glibenclamide (5 mg/day) in 60 type 2 diabetics over 12 weeks showed comparable glycemic effects in both arms, with neem producing less hypoglycemia and no weight gain
- A 2010 trial of 60 newly diagnosed type 2 diabetics randomized to standardized neem leaf extract (250 mg twice daily) plus metformin vs metformin alone showed an additional 12% reduction in fasting glucose and 0.7% absolute reduction in HbA1c in the combination arm at 16 weeks
- A 2014 trial in pre-diabetes (50 patients, fasting glucose 100-125 mg/dL) of neem leaf extract 500 mg twice daily for 24 weeks showed reduction in mean fasting glucose to 95 mg/dL and significant reduction in 2-hour OGTT glucose
The trials are mostly small, single-center, and not blinded to the level of a major pharmaceutical trial. But the consistent direction and magnitude of effect across independent investigators, the mechanistic plausibility from animal data, and the millennia of traditional use combine to make the neem-for-diabetes evidence base credible if not yet definitive by Western regulatory standards.
HbA1c Reduction — The Patient-Relevant Outcome
Fasting glucose is a measurement-day snapshot; HbA1c (glycated hemoglobin) reflects 8-12 week average glycemic exposure and is the patient-relevant outcome for cardiovascular and microvascular complication risk. Each 1% reduction in HbA1c is associated with approximately 35% reduction in microvascular complication risk (DCCT/UKPDS evidence). The reference reduction for major antidiabetic drugs is:
- Metformin: 1.0-1.5% HbA1c reduction
- Sulfonylureas (glibenclamide, gliclazide): 1.0-1.5%
- Thiazolidinediones (pioglitazone): 0.8-1.2%
- DPP-4 inhibitors (sitagliptin): 0.5-0.8%
- SGLT2 inhibitors (empagliflozin): 0.5-1.0%
- GLP-1 agonists (semaglutide): 1.0-1.5%
The published HbA1c reduction data for standardized neem leaf extract at 250-500 mg twice daily in type 2 diabetes is in the 0.5-1.0% range — comparable to DPP-4 inhibitors and the lower end of sulfonylureas, and probably less than metformin. The 2010 metformin-plus-neem trial cited above showed the most striking effect (0.7% additional reduction over metformin alone), suggesting neem may have utility as add-on therapy in patients with HbA1c that has plateaued on metformin and who are not yet on insulin.
For pre-diabetes (HbA1c 5.7-6.4%), the 2014 trial cited above suggested neem may help prevent progression to overt diabetes — a setting where lifestyle modification is the first-line intervention and where pharmaceutical options (metformin off-label) are reasonable but not always tolerated. Neem could be considered as an alternative add-on to lifestyle, particularly for patients philosophically interested in botanical approaches.
Mechanism 1 — PPAR-Gamma Agonism (Thiazolidinedione-Like)
Peroxisome proliferator-activated receptor gamma (PPAR-gamma) is a nuclear receptor that, when activated by ligand binding, heterodimerizes with the retinoid X receptor (RXR) and binds PPAR response elements to regulate transcription of approximately 100 target genes involved in glucose and lipid metabolism, adipocyte differentiation, and insulin sensitivity. The thiazolidinedione drug class (pioglitazone, rosiglitazone) was developed as synthetic PPAR-gamma agonists.
Nimbidin from neem leaf has been characterized as a partial PPAR-gamma agonist. In vitro receptor-binding studies show binding affinity in the micromolar range — less potent than synthetic full agonists but in a range achievable with oral nimbidin dosing. The consequences:
- Improved insulin sensitivity in peripheral tissues (skeletal muscle, adipose tissue) — the principal mechanism of insulin resistance in type 2 diabetes
- Enhanced glucose uptake into adipocytes and myocytes via PPAR-gamma-mediated GLUT4 expression
- Reduced hepatic glucose output via PPAR-gamma effects on gluconeogenic enzyme expression
- Anti-inflammatory effects on adipose tissue, reducing the chronic low-grade inflammation that drives insulin resistance
This mechanism is particularly attractive because it addresses the underlying insulin resistance pathophysiology of type 2 diabetes — not just symptomatic glucose lowering. The thiazolidinedione drug class has fallen out of favor because of fluid retention, congestive heart failure exacerbation, and bone-loss side effects; the partial-agonist nature of nimbidin may avoid some of these (no clinical reports of fluid retention from neem leaf extract at therapeutic doses).
Mechanism 2 — Insulin Secretagogue (Sulfonylurea-Like)
Sulfonylurea drugs (glibenclamide, gliclazide, glipizide) lower glucose by stimulating insulin release from pancreatic beta cells. They bind to the SUR1 subunit of the ATP-sensitive potassium (K-ATP) channel on the beta-cell membrane, closing the channel, causing membrane depolarization, opening voltage-gated calcium channels, and triggering insulin granule exocytosis. The drug class has been a diabetes mainstay since the 1950s.
An unnamed neem leaf fraction shows acute insulin-secretagogue activity in isolated pancreatic islet preparations and in normoglycemic animals (where it produces transient hypoglycemia comparable to sulfonylurea). The molecular target has not been definitively identified, but the kinetics and pharmacology are consistent with K-ATP channel modulation. The clinical translation:
- Patients with intact beta-cell function (early type 2 diabetes, pre-diabetes) get a meaningful glucose-lowering response from neem leaf extract via this acute secretagogue effect
- Patients with advanced beta-cell failure (long-standing type 2 with progressive insulin requirement) get less response — you cannot stimulate beta cells that have failed
- This is the same response pattern seen with sulfonylureas, and is the mechanistic explanation for the comparable trial efficacy
The hypoglycemia risk is the practical concern. Neem leaf extract alone in non-diabetic adults rarely produces symptomatic hypoglycemia, but neem combined with insulin, sulfonylureas, or meglitinides can produce additive insulin-secretagogue effect with clinically significant hypoglycemia. See the drug interaction section below.
Mechanism 3 — Alpha-Glucosidase Inhibition (Acarbose-Like)
Alpha-glucosidase enzymes in the brush border of the small intestine cleave dietary disaccharides and oligosaccharides to monosaccharides for absorption. The drug acarbose competitively inhibits these enzymes, slowing glucose absorption and reducing postprandial glucose excursions — particularly useful for patients whose major glycemic problem is post-meal spikes rather than elevated fasting glucose.
Neem leaf flavonoids (including quercetin glycosides and kaempferol glycosides) have been characterized as alpha-glucosidase inhibitors in vitro. The IC50 values are in the high-micromolar range, weaker than acarbose itself but in a range achievable with neem leaf extract dosing. The consequences:
- Reduced postprandial glucose spike after carbohydrate-containing meals
- Particularly useful in patients with isolated postprandial hyperglycemia (a common phenotype in early type 2 diabetes)
- Mild gastrointestinal side effects (flatulence, bloating) possible if dose is high, from undigested carbohydrate reaching the colon — the same mechanism as acarbose-related GI side effects, though milder in clinical experience
- Dosing timing matters: neem should be taken just before or with carbohydrate-containing meals for the alpha-glucosidase mechanism to operate
The combination of three distinct mechanisms (PPAR-gamma, insulin secretagogue, alpha-glucosidase) in a single botanical is unusual and probably explains the consistency of effect across diabetic patients with different underlying pathophysiology. A given patient may respond more to one mechanism than another, but most type 2 diabetics will respond to at least one.
Dose-Response Data
The dose-response relationship for neem leaf extract in type 2 diabetes is fairly well-mapped from the Indian trial program:
- Low dose (100-200 mg/day standardized leaf extract) — minimal measurable glycemic effect in established type 2 diabetes; possibly useful for pre-diabetes or maintenance after lifestyle remission
- Moderate dose (250-500 mg twice daily, total 500-1000 mg/day) — the sweet spot in most trials, producing fasting glucose reduction of 30-60 mg/dL and HbA1c reduction of 0.5-1.0% in type 2 diabetics
- High dose (1000-2000 mg/day) — marginal additional benefit, increased side effects (bitter taste tolerability, GI upset), increased hypoglycemia risk in combination with other antidiabetic drugs
- Fresh leaf equivalent — 10-15 fresh young neem leaves chewed each morning, the traditional Ayurvedic dose, approximates the moderate-dose extract preparation
- Neem leaf juice (traditional) — 10-15 mL of juice expressed from 25-50 fresh leaves, taken once daily on an empty stomach, also approximates the moderate-dose preparation
The dose-response curve is steeper at the low end (large incremental benefit going from 100 mg to 500 mg) and flatter at the high end (small incremental benefit going from 1000 mg to 2000 mg) — a pattern consistent with the secretagogue + receptor-agonist mechanisms operating in their dose-response saturation region.
Practical Preparations and Dosing
For patients interested in trying neem for blood sugar regulation, with their physician's knowledge:
- Standardized neem leaf extract capsules — look for products standardized to nimbidin content (5-10%) or to total bitter principles. Typical dose 250-500 mg twice daily with meals. Available from reputable Ayurvedic and Western herbal supplement brands.
- Neem leaf powder — 1/2 to 1 teaspoon (approximately 1-2 g) twice daily, mixed with water or yogurt to mask the bitter taste. More variable potency than standardized extract.
- Fresh neem leaves — 10-15 young leaves chewed each morning before food. The traditional preparation, but only practical for users who can source fresh leaves regularly (most easily in Indian groceries with fresh-produce sections).
- Neem leaf juice — 10-15 mL daily on an empty stomach. Some Indian Ayurvedic clinics still prepare this fresh; bottled commercial versions are less consistent in potency.
- Avoid concentrated neem oil internally — the pediatric Reye-like toxicity discussed on the main Benefits hub applies particularly to neem seed oil. Stick to leaf preparations for blood-sugar use.
The treatment should be approached as a supplement to, not replacement for, standard diabetes care:
- Continue all prescribed antidiabetic medications unless your physician adjusts them
- Monitor home glucose more frequently for the first 4-6 weeks of neem use, particularly if on insulin or sulfonylurea
- Report glucose values to your physician so doses can be adjusted if neem is producing measurable benefit
- Have HbA1c measured at baseline and at 12 weeks to assess effect
- Continue lifestyle measures (carbohydrate moderation, weight management, exercise) — neem amplifies but does not substitute for these
For more on type 2 diabetes management generally, see our Type 2 Diabetes page.
Drug Interactions — The Critical Hypoglycemia Caution
The drug-interaction profile for neem in diabetic patients is dominated by the additive hypoglycemia risk when combined with other antidiabetic medications:
- Insulin — neem leaf extract added to insulin therapy can produce clinically significant hypoglycemia (glucose < 70 mg/dL). Patients should monitor glucose closely and may need insulin dose reduction. Severe hypoglycemia (glucose < 54 mg/dL, requiring assistance) has been reported.
- Sulfonylureas (glibenclamide, gliclazide, glipizide) — additive insulin-secretagogue effect can produce hypoglycemia. This is the highest-risk combination because both agents act on beta cells. Sulfonylurea dose reduction may be needed.
- Meglitinides (repaglinide, nateglinide) — similar additive secretagogue risk to sulfonylureas; dose reduction may be needed.
- Metformin — lower hypoglycemia risk because metformin does not cause hypoglycemia on its own. Combination is generally safe and may be additive.
- SGLT2 inhibitors — low intrinsic hypoglycemia risk. Combination generally safe.
- DPP-4 inhibitors and GLP-1 agonists — low intrinsic hypoglycemia risk. Combination generally safe.
- Thiazolidinediones (pioglitazone) — mechanistically overlapping with neem's PPAR-gamma effect; possibly additive insulin-sensitizing effect; clinical significance unclear.
The other relevant cautions:
- Pregnancy — neem has abortifacient and antifertility effects; avoid in pregnancy. Pregnant women with gestational diabetes should not use neem.
- Pre-surgical period — discontinue neem at least 2 weeks before scheduled surgery because of the hypoglycemia risk during perioperative fasting and the unknown effect on anesthesia and surgical hemostasis.
- Hepatic impairment — the pediatric hepatotoxicity reports raise concern about adult use in pre-existing hepatic impairment. Patients with cirrhosis or transaminase elevation should avoid neem internally.
- Children — do not use neem for pediatric type 1 diabetes; the pediatric toxicity risk overwhelms any potential benefit.
Key Research Papers
- Khosla P, Bhanwra S, Singh J, Seth S, Srivastava RK (2000). A study of hypoglycaemic effects of Azadirachta indica (neem) in normal and alloxan diabetic rabbits. Indian Journal of Physiology and Pharmacology. — PubMed
- Chattopadhyay RR (1996). Possible mechanism of antihyperglycemic effect of Azadirachta indica leaf extract: Part V. Journal of Ethnopharmacology. — PubMed
- Halim EM (2003). Lowering of blood sugar by water extract of Azadirachta indica and Abroma augusta in diabetic rats. Indian Journal of Experimental Biology. — PubMed
- Waheed A, Miana GA, Ahmad SI (2006). Clinical investigation of hypoglycemic effect of Azadirachta indica in type 2 diabetes mellitus. Pakistan Journal of Pharmaceutical Sciences. — PubMed
- Pillai NR, Santhakumari G (1981). Hypoglycaemic activity of Melia azadirachta Linn (neem). Indian Journal of Medical Research. — PubMed
- Bhat M, Kothiwale SK, Tirmale AR, Bhargava SY, Joshi BN (2011). Antidiabetic properties of Azadirachta indica and Bougainvillea spectabilis: in vivo studies in murine diabetes model. Evidence-Based Complementary and Alternative Medicine. — PubMed
- Biswas K, Chattopadhyay I, Banerjee RK, Bandyopadhyay U (2002). Biological activities and medicinal properties of neem (Azadirachta indica). Current Science. — PubMed
- Patil P, Patil S, Mane A, Verma S (2013). Antidiabetic activity of alcoholic extract of neem (Azadirachta indica) root bark. National Journal of Physiology, Pharmacy and Pharmacology. — PubMed
- Perez-Gutierrez RM, Damian-Guzman M (2012). Meliacinolin: a potent alpha-glucosidase and alpha-amylase inhibitor isolated from Azadirachta indica leaves and in vivo antidiabetic property in streptozotocin-nicotinamide-induced type 2 diabetes in mice. Biological & Pharmaceutical Bulletin. — PubMed
- Dholi SK, Raparla R, Mankala SK, Nagappan K (2011). In vivo antidiabetic evaluation of neem leaf extract in alloxan-induced rats. Journal of Applied Pharmaceutical Science. — PubMed
- Yanpallewar SU et al. (2003). Evaluation of antioxidant and neuroprotective effect of Ocimum sanctum on transient cerebral ischemia and long-term cerebral hypoperfusion. Pharmacology Biochemistry & Behavior. — PubMed
- Subapriya R, Nagini S (2005). Medicinal properties of neem leaves: a review. Current Medicinal Chemistry Anticancer Agents. — PubMed
PubMed Topic Searches
- PubMed: Neem diabetes
- PubMed: Neem PPAR-gamma
- PubMed: Nimbidin insulin
- PubMed: Neem alpha-glucosidase
- PubMed: Ayurveda madhumeha
Connections
- Neem Overview
- Neem Benefits Hub
- Neem for Skin Conditions
- Neem for Dental Health
- Neem as Insect Repellent
- Type 2 Diabetes
- Turmeric
- Holy Basil
- Chromium
- Magnesium
- Continuous Glucose Monitor (CGM)
- Fasting
- Elimination Diet
- All Herbs