Mononucleosis
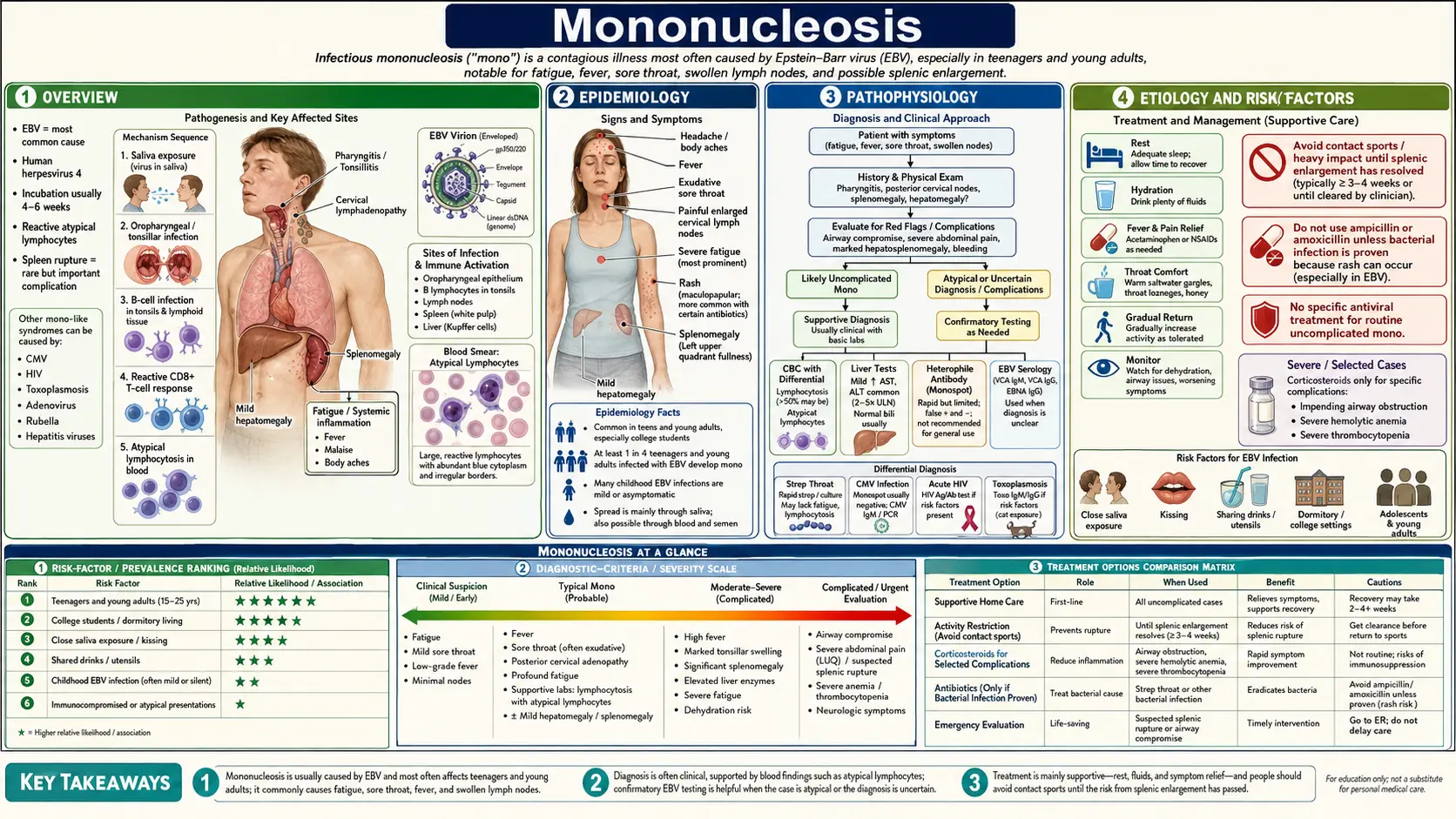
Table of Contents
- Overview
- Epidemiology
- Pathophysiology
- Etiology and Risk Factors
- Clinical Presentation
- Diagnosis
- Treatment
- Complications
- Prognosis
- Prevention
- Recent Research and Advances
- Research Papers
- Connections
- Featured Videos
1. Overview
Infectious mononucleosis — often just called mono, or famously "the kissing disease" — is the illness most people get when they first catch the Epstein–Barr virus (EBV), usually as a teenager or young adult. The hallmark is a sore throat that will not quit, swollen glands in the neck, a fever, and a bone-deep, knock-you-flat tiredness that lasts far longer than an ordinary cold. If you have ever been told you "have mono," what your body is really doing is mounting an enormous immune battle against EBV for the first time.
Here is the part that surprises most people: EBV is almost universal. By adulthood, roughly 90–95% of people worldwide carry the virus for life, mostly without ever knowing it. Mono is not what happens when EBV is rare or dangerous — it is what happens when the first infection is delayed from early childhood (when it is usually silent) to adolescence or young adulthood (when the immune response is bigger and the symptoms are dramatic). Catch EBV at age 4 and you probably never notice. Catch it for the first time at 18 and you may spend two weeks in bed.
The good news is that mono, while miserable, is almost always self-limiting — the immune system wins, and the vast majority of people recover completely. The complication everyone should know about is splenic rupture: the spleen swells during mono, and a sharp blow (or even straining) can rarely tear it. That single fact drives the most important practical advice in this article — no contact sports or heavy lifting for several weeks. This page also covers, honestly and carefully, the longer scientific tail of EBV: its real and well-documented links to multiple sclerosis, post-viral fatigue and chronic fatigue syndrome, and certain lymphomas — while steering firmly away from the pseudoscience of "chronic EBV" cure mills.
2. Epidemiology
EBV is one of the most successful viruses on Earth. It infects more than 90% of the global adult population, and once it is in, it stays for life, hiding quietly in a small pool of memory B cells. The disease mononucleosis, however, is far less common than the virus, because most infections happen in early childhood and cause nothing more than a mild cold — or no symptoms at all.
When EBV infection is delayed, the picture changes. In high-income countries with good hygiene, a large fraction of children reach adolescence still EBV-negative, and it is these teens and young adults who develop classic mono on first exposure. The peak incidence is between roughly ages 15 and 24. In one large prospective study of university students, about one in four of those who acquired primary EBV during college developed clinically recognizable infectious mononucleosis. Estimated incidence in the 15–24 age group is on the order of several hundred to ~1,000 cases per 100,000 people per year.
There is a striking socioeconomic and geographic pattern. In lower-income settings, EBV is acquired almost universally in the first few years of life, so symptomatic mono is uncommon — but EBV-associated cancers such as Burkitt lymphoma (in equatorial Africa) and nasopharyngeal carcinoma (in parts of East and Southeast Asia) are more frequent, reflecting different co-factors and host genetics. In wealthy countries, the trade-off is more mono in adolescence and a stronger statistical link to multiple sclerosis later in life.
3. Pathophysiology
To understand why mono feels the way it does, it helps to follow the virus. EBV is spread mainly through saliva — hence "the kissing disease," but also shared drinks, utensils, and toothbrushes. The virus first infects cells in the throat and then targets B lymphocytes, the antibody-producing white blood cells. EBV is a herpesvirus, and like all herpesviruses it is a master of persistence: rather than killing its host cells outright, it can switch into a latent program, driving infected B cells to proliferate while expressing only a handful of viral genes.
Crucially, most of the symptoms of mono are caused by your own immune system, not directly by the virus. The body responds to EBV-infected B cells with a massive expansion of CD8+ cytotoxic T cells — these are the "atypical lymphocytes" (also called reactive lymphocytes or Downey cells) seen on a blood smear, and the surge of mononuclear cells is what gives the disease its name. This enormous T-cell response is responsible for the swollen lymph nodes, the inflamed tonsils and throat, the enlarged spleen and liver, and much of the fever and fatigue. It is an immune "storm" of recognition and clearance.
Once the acute battle is won, EBV is not eliminated. It retreats into lifelong latency in resting memory B cells, where it periodically reactivates at low levels, sheds back into saliva, and is passed to the next person — usually without causing any symptoms. This permanent latency, and the way EBV manipulates B-cell biology, is the thread that connects acute mono to the virus's much rarer long-term associations with autoimmunity and cancer, discussed in the research section below.
4. Etiology and Risk Factors
Epstein–Barr virus causes the great majority of infectious mononucleosis — roughly 90% of cases. The single biggest risk factor is simply being an EBV-negative adolescent or young adult who is newly exposed, classically through intimate contact, shared drinks, or shared utensils. Crowded living, such as college dormitories and military barracks, raises the odds of exposure.
A smaller share of "mono-like" illness — the same fever, sore throat, swollen glands, and atypical lymphocytes — is caused by other infections, which matters because they are managed differently and the monospot test will be negative:
- Cytomegalovirus (CMV) — the most common cause of "heterophile-negative" mononucleosis; often less sore throat, more prolonged fever.
- Acute HIV infection — can mimic mono and must be considered, because diagnosis changes everything; ask about exposures and test when appropriate (see HIV/AIDS).
- Toxoplasmosis, and occasionally other viruses such as adenovirus or acute viral hepatitis.
It is also worth naming what does not cause mono. Strep throat (group A streptococcus) is a separate bacterial infection — but the two can look alike, and they can even coexist, which sets up one of the most useful clinical clues in all of medicine, covered next.
5. Clinical Presentation
After an incubation period of roughly four to six weeks from exposure, mono typically builds over several days. The classic triad is:
- Fever — often moderate to high, lasting one to two weeks.
- Pharyngitis — a severe, sometimes exudative sore throat with markedly enlarged, sometimes "kissing" tonsils that can nearly meet in the midline.
- Lymphadenopathy — swollen, tender lymph nodes, characteristically including the posterior cervical nodes (behind and below the ears, toward the back of the neck). Posterior chain involvement is a helpful pointer toward mono rather than ordinary strep, which favors the anterior nodes.
Layered on top of the triad are two features patients remember most: profound fatigue — an exhaustion out of all proportion to a "cold," sometimes making it hard to get through a school or work day — and splenomegaly, an enlarged spleen, present in roughly half of cases and the reason for the activity restrictions below. The liver is often mildly inflamed too, with elevated liver enzymes on blood tests in a large majority of patients (usually transient and harmless). Some people develop puffy eyelids, a fine rash, or a transient enlargement of the liver.
The amoxicillin/ampicillin rash — a practical pearl
Here is a clue worth knowing. When a person with active EBV mononucleosis is given amoxicillin or ampicillin (often because their sore throat was assumed to be strep), a high proportion — historically reported in the range of the majority of patients, though modern estimates are lower — develop a widespread, itchy, maculopapular rash within days. This is not a true lifelong penicillin allergy in most cases; it is a transient interaction between the antibiotic and the EBV-activated immune state. The practical message is twofold: it explains why mono is so often mistaken for strep and treated with the wrong drug, and the appearance of this rash after amoxicillin should make a clinician strongly suspect EBV. The lesson is not "never use penicillins forever," but "confirm the diagnosis before reaching for an antibiotic that will not help a viral illness."
6. Diagnosis
Mono is often suspected from the story and exam alone — a young person with a stubborn sore throat, big posterior neck nodes, fever, and disabling fatigue. Laboratory testing confirms it and rules out the look-alikes.
Blood count and smear
A complete blood count typically shows a lymphocytosis (high lymphocyte count) with a notable fraction of atypical/reactive lymphocytes on the smear — the activated T cells fighting the virus. Mild thrombocytopenia (low platelets) and elevated liver enzymes are common and usually benign.
The monospot (heterophile) test — useful, but with limits
The classic bedside test is the monospot, which detects heterophile antibodies — nonspecific antibodies the body makes during EBV mono. It is fast and cheap, but it has two important blind spots. First, it can be falsely negative early in the illness (in the first week or so) before heterophile antibodies have risen, so a negative test in someone who looks like they have mono may simply need repeating a week later. Second, it is less reliable in young children and does not become positive in CMV- or HIV-driven "mono-like" illness. A negative monospot does not rule mono out.
EBV-specific antibodies — the more precise tool
When the diagnosis is uncertain, or the monospot is negative but suspicion is high, EBV-specific serology sorts it out by timing:
- VCA IgM (viral capsid antigen, IgM class) — appears early and indicates a current/recent primary infection; it fades over weeks to months.
- VCA IgG — appears early and persists for life; it marks past or present infection.
- EBNA (Epstein–Barr nuclear antigen) IgG — the key timing clue: it appears late, typically weeks to months after onset, and persists for life. So VCA IgG positive but EBNA IgG negative points to a recent primary infection, whereas both positive indicates past infection.
Together these markers let clinicians distinguish a brand-new EBV infection (mono) from the lifelong, already-resolved infection that most adults carry. They also help avoid over-interpreting EBV antibodies as "proof" of an active chronic disease, a misuse discussed in the research section.
7. Treatment
The honest headline: there is no cure, and you mostly do not need one. Mono is a viral illness your immune system will defeat on its own. Treatment is supportive — comfort and time, not a pill that clears the virus.
- Rest — let your body do the work. Push through too hard and the fatigue tends to drag on.
- Fluids — a sore throat makes drinking unpleasant, so hydration takes effort; sip steadily.
- Pain and fever relief — acetaminophen (paracetamol) or ibuprofen for the throat, aches, and fever. Cool drinks, salt-water gargles, and throat lozenges help.
What does NOT help
This is important for avoiding both false hope and real harm:
- Antibiotics do nothing for mono — it is viral. And as noted above, amoxicillin/ampicillin can trigger a dramatic rash in EBV. Antibiotics are appropriate only if a separate bacterial infection (such as a true coexisting strep throat) is confirmed.
- Antivirals (such as acyclovir) do not meaningfully shorten mono. They can reduce viral shedding in the throat in studies, but this does not translate into faster recovery or better outcomes, so they are not recommended for routine cases.
Corticosteroids — reserved, not routine
Steroids are not used for ordinary mono and do not speed recovery. They are reserved for specific emergencies — most importantly impending airway obstruction from tonsils so enlarged that breathing or swallowing is threatened, and occasionally for severe complications such as marked thrombocytopenia or hemolytic anemia. In those situations a short steroid course can be life-saving, but it is a targeted intervention, not a general treatment for feeling unwell.
The spleen-and-sports message — the single most important advice
Because the spleen enlarges in mono, a blow to the abdomen, or even forceful straining, can rarely cause it to rupture — a true emergency. Guidance is consistent: avoid contact and collision sports, heavy lifting, and vigorous exertion for about three to four weeks from the start of symptoms (and longer for collision sports if the spleen is still enlarged). Most splenic ruptures occur within the first three weeks. This is not a casual suggestion — it is the one rule worth following to the letter. Light activity and a gradual return are fine once the acute phase passes; when in doubt about a contact sport, a clinician can reassess.
8. Complications
The overwhelming majority of people recover from mono without complications. When problems do occur, they include:
- Splenic rupture — rare (well under 1% of cases) but the most feared, presenting with sudden severe left-upper-abdomen or left-shoulder pain; a surgical emergency. This is the reason for the activity restrictions.
- Airway obstruction — from massively swollen tonsils; uncommon but a reason steroids exist for mono.
- Hematologic problems — mild thrombocytopenia is common and usually harmless; less often, autoimmune hemolytic anemia or significant low platelet counts.
- Hepatitis — mild liver inflammation with raised enzymes is the rule, not the exception; clinically obvious jaundice is uncommon (see hepatitis).
- Neurological complications — rare, including encephalitis, meningitis, or Guillain–Barré-type syndromes.
- Severe disease in the immunocompromised — people with weakened immune systems, or rare genetic susceptibilities, can develop chronic active EBV or aggressive lymphoproliferative disease.
9. Prognosis
For nearly everyone, mono is a self-limiting illness with an excellent outcome — but the timeline deserves an honest accounting, because unrealistic expectations cause real distress.
The acute symptoms — fever, the worst of the sore throat, the swollen glands — usually ease over one to two weeks. The fatigue is the laggard. Most people feel substantially better and return to normal activities within two to four weeks, but a meaningful minority feel low energy and reduced stamina for several weeks to a few months. That extended tiredness is normal and does not mean something is wrong; it reflects the size of the immune effort your body just made. Recovery is not always linear — good days and setback days are common.
A small subset of people experience prolonged, debilitating fatigue lasting six months or more after mono — this overlaps with chronic fatigue syndrome / myalgic encephalomyelitis (ME/CFS), discussed honestly in the research section. If you are still profoundly exhausted months later, your suffering is real and recognized in the medical literature; it is not "all in your head." What it does not require is repeated antiviral courses or "EBV detox" programs, which are not supported by evidence.
10. Prevention
Honesty first: there is no practical way to avoid a virus that more than 90% of humanity carries. EBV is ubiquitous, spread by ordinary saliva contact, and most people are exposed long before anyone could intervene. There is currently no licensed vaccine. So prevention advice is modest and aimed mainly at reducing spread during an active illness:
- While you (or someone) are sick with mono, do not share drinks, utensils, toothbrushes, or kisses. EBV is shed in saliva, sometimes for months after symptoms resolve, but transmission risk is highest during the acute illness.
- Ordinary hand and respiratory hygiene applies, though EBV is not as casually airborne as a cold.
- There is no need for isolation or staying home from school/work beyond what symptoms dictate — the virus is already everywhere, and the activity restriction that matters is about the spleen, not contagion.
The real hope for prevention is a vaccine. Decades of effort, and a renewed push using modern mRNA and nanoparticle platforms, are aimed at an EBV vaccine that could prevent mono and, potentially, reduce EBV-linked diseases such as multiple sclerosis and certain cancers. That work is genuinely exciting — and genuinely unproven — and is covered carefully below.
11. Recent Research and Advances
EBV has become one of the most scientifically interesting viruses in medicine, because its lifelong relationship with our immune system links a common teenage illness to some of the hardest problems in neurology and oncology. This section lays out what is genuinely established, what is plausible but unproven, and what is hype — because the difference matters enormously for patients.
EBV and multiple sclerosis — landmark, empowering science
This is real and important. In 2022, Bjornevik and colleagues published a landmark analysis in Science following more than 10 million young U.S. military personnel over two decades. They found that the risk of developing multiple sclerosis (MS) increased 32-fold after EBV infection — and, critically, MS essentially did not develop in people who remained EBV-negative. The data strongly support EBV as a likely necessary cause of MS: it appears you almost have to have been infected with EBV to develop MS.
It is just as important to state what this does not mean. EBV is necessary but clearly not sufficient — more than 90% of people carry EBV and the overwhelming majority never get MS. Genetics, other environmental factors (such as vitamin D status, smoking, and obesity in adolescence), and chance all contribute. A companion 2022 study by Lanz and colleagues in Nature offered a mechanism: some antibodies and immune cells targeting an EBV protein (EBNA1) cross-react with a protein in the brain (GlialCAM), a form of molecular mimicry that could drive autoimmune attack on myelin. This is empowering science — it reframes MS as a disease with an identifiable trigger and opens the door to prevention through an EBV vaccine — but it is not a simple one-virus-one-disease story, and EBV-positive people should not be alarmed.
EBV, post-viral fatigue, and ME/CFS — validating real suffering, honestly
The link between mono and prolonged fatigue is well documented. In a careful prospective study of adolescents, Katz and colleagues found that a measurable percentage still met criteria for chronic fatigue syndrome six months after mono, with a smaller fraction affected at one and two years. Post-infectious ME/CFS is a recognized phenomenon, and the disabling fatigue some people experience after mono is real, biological, and not imagined. Researchers are actively studying the mechanisms — persistent immune activation, autonomic dysfunction, and altered energy metabolism among them.
At the same time, the evidence does not support treating post-mono fatigue with repeated antiviral drugs, high-dose supplements marketed as "EBV killers," or "reactivation detox" protocols. Validating the suffering and chasing unproven cures are two different things. The compassionate, evidence-aligned approach is symptom management, pacing, and addressing sleep, mood, and deconditioning — see chronic fatigue syndrome for a fuller discussion.
"Chronic EBV" overdiagnosis — a caution
A genuine entity called chronic active EBV (CAEBV) exists, but it is rare and serious — characterized by very high viral loads, organ involvement, and a substantial mortality, as described by Kimura and colleagues. It is not the same as a positive EBV antibody test in someone with fatigue. Because more than 90% of healthy adults carry EBV and have positive antibodies for life, EBV serology is not a meaningful test for diagnosing chronic illness in the general population. A large industry of "chronic EBV reactivation" diagnoses and treatments has grown around misinterpreting normal antibody results. The honest position: real post-viral suffering deserves care and respect, but routine antiviral treatment of "chronic EBV" is not supported by evidence and can do harm.
EBV-associated cancers
EBV is one of the most important cancer-causing viruses in humans, contributing to a small fraction of cases of Burkitt lymphoma, some Hodgkin lymphoma, certain aggressive lymphomas in immunocompromised people, nasopharyngeal carcinoma, and a subset of gastric (stomach) cancers. The absolute risk for any one EBV-infected person is very low — these cancers require additional co-factors and host susceptibility — but at the population scale, given how common EBV is, the contribution is significant (see cancer). Thorley-Lawson and colleagues showed how EBV's manipulation of B-cell biology during lifelong latency provides the mechanistic bridge from a common infection to these malignancies.
An EBV vaccine — real hope, no overpromise
An effective EBV vaccine would be a landmark: it could prevent mono and, in principle, reduce the burden of EBV-linked MS and cancers. An earlier gp350 protein vaccine (Sokal and colleagues, phase 2) reduced the incidence of symptomatic mononucleosis but did not prevent EBV infection itself. The current generation uses mRNA and nanoparticle platforms targeting multiple viral proteins, with early-phase human trials underway. The honest status: these are promising but unproven — no EBV vaccine is yet licensed, efficacy and durability are still being tested, and any benefit for MS or cancer would take years to demonstrate. It is reasonable to be hopeful and unreasonable to claim a vaccine is around the corner.
12. References & Research
Historical Background
The clinical syndrome was named "infectious mononucleosis" by Thomas Sprunt and Frank Evans in 1920, who described the characteristic mononuclear-cell blood picture in young adults with acute febrile illness. The causative virus was discovered decades later: in 1964, Michael Anthony Epstein, Yvonne Barr, and Bert Achong identified herpesvirus-like particles by electron microscopy in cells from African Burkitt lymphoma — the first human tumor virus — and the agent was named the Epstein–Barr virus. In the late 1960s, Werner and Gertrude Henle serendipitously linked EBV to infectious mononucleosis when a laboratory worker developed mono and seroconverted, tying the new virus to the long-known heterophile-antibody disease (the basis of the monospot test). More than half a century on, the 2022 demonstration that EBV is a likely necessary cause of multiple sclerosis stands as a defining advance, transforming EBV from "the kissing-disease virus" into a central player in human neurology and oncology.
Key Research Papers
- Bjornevik K, Cortese M, Healy BC, et al. Longitudinal analysis reveals high prevalence of Epstein-Barr virus associated with multiple sclerosis. Science. 2022;375(6578):296-301.
- Lanz TV, Brewer RC, Ho PP, et al. Clonally expanded B cells in multiple sclerosis bind EBV EBNA1 and GlialCAM. Nature. 2022;603(7900):321-327.
- Luzuriaga K, Sullivan JL. Infectious mononucleosis. New England Journal of Medicine. 2010;362(21):1993-2000.
- Cohen JI. Epstein-Barr virus infection. New England Journal of Medicine. 2000;343(7):481-492.
- Dunmire SK, Verghese PS, Balfour HH. Primary Epstein-Barr virus infection. Journal of Clinical Virology. 2018;102:84-92.
- Odumade OA, Hogquist KA, Balfour HH. Progress and problems in understanding and managing primary Epstein-Barr virus infections. Clinical Microbiology Reviews. 2011;24(1):193-209.
- Lennon P, Crotty M, Fenton JE. Infectious mononucleosis. BMJ. 2015;350:h1825.
- Thorley-Lawson DA, Gross A. Persistence of the Epstein-Barr virus and the origins of associated lymphomas. New England Journal of Medicine. 2004;350(13):1328-1337.
- Katz BZ, Shiraishi Y, Mears CJ, et al. Chronic fatigue syndrome after infectious mononucleosis in adolescents. Pediatrics. 2009;124(1):189-193.
- Kimura H, Morishima T, Kanegane H, et al. Prognostic factors for chronic active Epstein-Barr virus infection. Journal of Infectious Diseases. 2003;187(4):527-533.
- Jayasooriya S, de Silva TI, Njie-jobe J, et al. Early virological and immunological events in asymptomatic Epstein-Barr virus infection in African children. PLOS Pathogens. 2015;11(3):e1004746.
- Sokal EM, Hoppenbrouwers K, Vandermeulen C, et al. Recombinant gp350 vaccine for infectious mononucleosis: a phase 2, randomized, double-blind, placebo-controlled trial in healthy young adults. Journal of Infectious Diseases. 2007;196(12):1749-1753.
- Zhong L, Krummenacher C, Zhang W, et al. Urgency and necessity of Epstein-Barr virus prophylactic vaccines. npj Vaccines. 2022;7(1):159.
Research Papers
Use the live PubMed searches below to explore the current peer-reviewed literature on mononucleosis and Epstein-Barr virus. Each link opens a fresh search in a new tab, so results stay up to date as new studies are published.
- Infectious mononucleosis diagnosis
- Epstein-Barr virus primary infection
- EBV and multiple sclerosis
- Mononucleosis splenic rupture
- EBV chronic fatigue syndrome
- Heterophile (monospot) test performance
- Amoxicillin rash and EBV
- EBV vaccine clinical trials
- EBV-associated cancers
- Corticosteroids in mononucleosis
- Chronic active EBV infection
- Mononucleosis return to sport
Connections
- Chronic Fatigue Syndrome (ME/CFS) — the post-viral fatigue some people develop after mono.
- Multiple Sclerosis — EBV is now considered a likely necessary cause.
- Hepatitis — mild EBV liver inflammation is common in mono.
- Lymphoma — EBV contributes to Burkitt, some Hodgkin, and other lymphomas.
- Cancer — EBV is an important human tumor virus.
- Anemia — autoimmune hemolytic anemia is a rare mono complication.
- Thrombocytopenia — mild low platelets are common in acute mono.
- Sinusitis — another cause of overlapping upper-respiratory and throat symptoms.
- Fatigue — the defining and longest-lasting symptom of mono.
- Joint Pain — body aches accompany the acute viral illness.
- HIV/AIDS — acute HIV can mimic mono and must be considered.
- Infectious Disease — the full category of infections.
- Silver Nanoparticles & EBV — related remedy discussion.
- All Conditions — browse every disease topic.