Ginseng for Immune and Antiviral Function
Ginseng's immune-supporting reputation in traditional medicine has been confirmed by an unusually well-designed clinical trial. The Scaglione 1996 study randomized 227 healthy adults to either G115 standardized Panax ginseng extract (100 mg twice daily for 12 weeks) or matching placebo, with all subjects receiving a polyvalent influenza vaccine at week 4. By week 12, the ginseng arm showed an influenza incidence of 15% versus 42% in placebo — a relative risk reduction of approximately 64% — and antibody titers to the vaccine antigens were roughly doubled. A separate line of research on American ginseng extract CVT-E002 (sold commercially as COLD-FX) by the University of Alberta produced consistent reductions in upper respiratory infection frequency in institutionalized elderly populations across multiple trials. The mechanism centers on enhanced natural killer (NK) cell cytotoxicity, increased macrophage and dendritic cell activation, and an adjuvant-like effect on antibody-class switching in B cells — the same broad immune-modulating effects that explain ginseng's traditional use as a "winter tonic" in cold climates.
Table of Contents
- The Traditional "Winter Tonic" Indication
- The Scaglione 1996 Trial — G115 + Influenza Vaccine
- CVT-E002 (COLD-FX) — American Ginseng for Upper Respiratory Infection
- Natural Killer (NK) Cell Activation
- Macrophage and Dendritic Cell Activation
- Antibody Class-Switching and Vaccine Adjuvant Effect
- Polysaccharides vs Ginsenosides — Two Active Fractions
- Elderly Immune Decline (Immunosenescence)
- Dosing and Timing for Immune Use
- Cautions, Limitations, and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
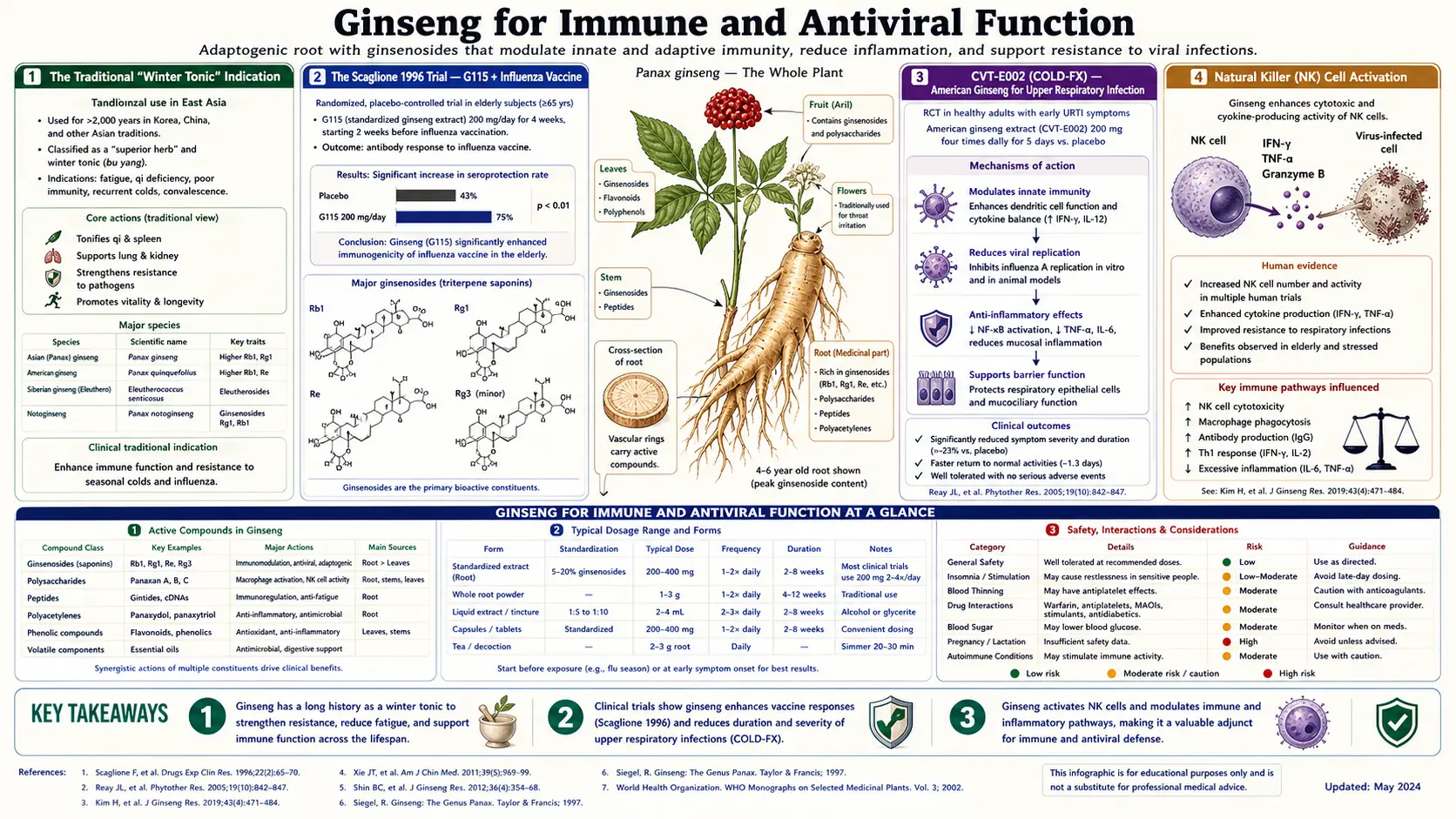
The Traditional "Winter Tonic" Indication
The traditional Chinese and Korean medical use of ginseng for "preventing colds" and "supporting recovery from prolonged illness" predates any concept of viruses or immune cells by roughly two thousand years. The empirical observation was that people who took ginseng regularly tended to get fewer respiratory illnesses each winter, recovered faster from those they did catch, and convalesced from major illness with more vigor. The classical Chinese pharmacology categorized this as ginseng's effect of "tonifying lung qi and protecting wei qi" (defensive qi, roughly equivalent to the modern concept of innate immunity).
Modern immunology has largely vindicated the traditional claim, though with the caveat that "regularly" is doing important work in the description — ginseng's immune effects accumulate over weeks of dosing and are not particularly impressive in single-dose form. The classical "winter tonic" use, where someone begins taking ginseng in early autumn and continues through winter, maps closely to the most successful modern clinical trials, which use 4-12 weeks of pre-exposure dosing before evaluating infection rates.
The relevance of ginseng to acute infectious disease (taking ginseng once a cold has already started) is less well-supported by the literature. Like vitamin C, ginseng appears more useful for prevention than for treatment of established viral illness.
The Scaglione 1996 Trial — G115 + Influenza Vaccine
The single most important clinical demonstration of ginseng's immune effect is the Scaglione 1996 trial, conducted at the University of Milan and published in the journal Drugs Under Experimental and Clinical Research. The trial enrolled 227 healthy adults (mean age 49) during the autumn influenza season and randomized them to either:
- G115 standardized Panax ginseng extract, 100 mg twice daily for 12 weeks
- Identical-appearing placebo
All subjects received a polyvalent (3-strain) influenza vaccine at week 4. The trial measured (1) confirmed influenza or common-cold incidence over the 12-week period, (2) post-vaccination antibody titers to the included influenza strains, and (3) natural killer cell activity in a subset.
Results:
- Influenza/cold incidence: 15 cases in the ginseng arm vs 42 cases in placebo — a relative risk reduction of approximately 64% (statistically significant, p < 0.001)
- Antibody titers: the ginseng arm showed mean antibody titers approximately double those in placebo to all three included influenza strains, measured 8 weeks post-vaccination
- NK cell activity: approximately 2-fold higher in the ginseng arm than in placebo
- Tolerability: adverse event rates were not statistically different between arms; no excess of any specific adverse event
The Scaglione trial is widely cited as the strongest single demonstration of an herbal supplement potentiating vaccine response in healthy adults. It has not been replicated at exactly the same scale, but the consistent direction of effect across the various downstream measures (clinical infection rate, antibody titer, NK cell activity) gives the result internal coherence beyond a single endpoint.
The G115 product used in the trial is a Panax ginseng (Korean / Asian) extract standardized to 4% total ginsenosides — specifically, a defined ratio of Rg1, Rb1, and other ginsenosides developed and patented in the 1970s. It is sold under multiple brand names and is the same extract used in the Reay cognitive trials, the Caso Marasco 1996 placebo-controlled stress trial, and many other modern ginseng studies.
CVT-E002 (COLD-FX) — American Ginseng for Upper Respiratory Infection
A parallel line of research on American ginseng (Panax quinquefolius) was conducted at the University of Alberta starting in the late 1990s. The team isolated a poly-saccharide-rich fraction of American ginseng root, designated CVT-E002, and commercialized it under the brand name COLD-FX. Multiple randomized trials evaluated this preparation in different populations:
- McElhaney 2004 (institutionalized elderly): 198 nursing-home residents randomized to CVT-E002 200 mg twice daily or placebo for 8-12 weeks. Acute respiratory illness incidence: 23% in placebo, 8% in CVT-E002 (p = 0.009). Severe respiratory illness was also reduced.
- Predy 2005 (community-dwelling adults): 323 adults (mean age 43) randomized to CVT-E002 400 mg/day or placebo for 4 months during influenza season. The CVT-E002 arm experienced 0.68 colds per subject vs 0.93 colds per subject in placebo, with the difference being more pronounced in cold severity and duration.
- McElhaney 2011 (elderly chronic disease): a smaller trial in community-dwelling elderly adults with chronic obstructive pulmonary disease or congestive heart failure, suggesting CVT-E002 reduced exacerbations — though the trial was underpowered for definitive conclusions.
The CVT-E002 (American ginseng polysaccharide) and G115 (Korean ginseng standardized ginsenoside extract) lines of research suggest that two distinct fractions of ginseng can each independently support immune function: the polysaccharide fraction (more prominent in American ginseng, particularly the CVT-E002 preparation) and the ginsenoside fraction (more prominent in Korean Panax ginseng standardized extracts). This is biologically reasonable since polysaccharides and triterpene saponins activate different innate immune pathways — polysaccharides predominantly through pattern-recognition receptors on macrophages and dendritic cells, ginsenosides through more diverse downstream signaling.
COLD-FX (CVT-E002) is the most commercially successful evidence-supported herbal cold preventive in North America, particularly in Canada where it has been a fixture of the cough/cold aisle since the early 2000s. The product's regulatory status in the US is as a dietary supplement; in Canada it is a Natural Health Product with a Health Canada license number authorizing claims about cold/flu prevention.
Natural Killer (NK) Cell Activation
Natural killer (NK) cells are innate-immune lymphocytes specialized to kill virus-infected cells and certain tumor cells without requiring prior antigen exposure or MHC restriction. They are first-line responders to viral infection, killing infected cells before adaptive immunity (T cells, antibody) has time to organize. NK cell activity declines with age and chronic stress, contributing to elderly susceptibility to viral infection and reactivation of latent herpesviruses.
Multiple ginseng preparations have demonstrated NK cell enhancement in human studies:
- Scaglione 1996 showed roughly 2-fold NK activity increase in vaccinated subjects taking G115
- Korean red ginseng polysaccharide preparations have shown NK enhancement in cancer patient populations
- CVT-E002 (American ginseng polysaccharide) has shown NK enhancement in vitro and in elderly subjects
- Ginsenoside Rh1 (a deglycosylated ginsenoside metabolite generated by gut microbial action on Rg1) has been shown to enhance NK cytotoxicity against tumor cell lines in vitro
The NK-enhancing effect is particularly relevant for elderly populations (where immunosenescence has reduced baseline NK function), cancer patients (where chemotherapy and disease have depressed NK function), and chronically stressed individuals (where elevated cortisol suppresses NK activity).
Macrophage and Dendritic Cell Activation
Macrophages and dendritic cells are the principal antigen-presenting cells of the innate immune system. They phagocytize pathogens, process antigens, and present them to T cells in the context of MHC class II to initiate adaptive immune responses. Ginsenosides modulate both cell types:
- Macrophage activation — ginsenoside Rg1 increases macrophage phagocytic activity, increases TNF-alpha and IL-1-beta production at appropriate doses (an effect that is paradoxically anti-inflammatory in the context of chronic low-grade inflammation, because it shifts macrophages from a stuck M2 phenotype to a more flexible M1 capability), and increases nitric oxide production from inducible NOS (iNOS) as part of pathogen-killing capacity.
- Dendritic cell maturation — ginsenoside Rb1 promotes dendritic cell maturation from immature precursors, upregulates surface MHC class II and co-stimulatory molecules (CD80, CD86), and enhances T-cell priming capacity. The net effect is improved antigen presentation to naive T cells, contributing to the vaccine adjuvant effect seen in the Scaglione trial.
- Toll-like receptor (TLR) signaling — ginseng polysaccharides act as agonists of TLR4 on macrophages and dendritic cells, mimicking some aspects of pathogen-associated molecular patterns (PAMPs) without the actual pathogenic risk. This is a common mechanism for plant-derived polysaccharide immunomodulators.
The macrophage / dendritic cell mechanism explains why ginseng is more useful for general immune resilience than for acute treatment of established infection — it primes the innate immune system to respond more robustly to future challenges, rather than substituting for antiviral or antibacterial therapy in active infection.
Antibody Class-Switching and Vaccine Adjuvant Effect
The Scaglione 1996 finding of doubled antibody titers in vaccinated subjects taking G115 is mechanistically explained by ginseng's adjuvant-like effects on B-cell biology. B cells require help from T-helper cells to class-switch from initial IgM production to higher-affinity IgG (the dominant protective antibody class for influenza). The factors that enhance this T-cell help and B-cell maturation include:
- Improved dendritic cell antigen presentation to naive T cells (ginseng effect, discussed above)
- Enhanced IL-4 and IL-21 production from T-follicular helper (Tfh) cells
- Improved germinal center reaction in lymph nodes, where B cells undergo somatic hypermutation and affinity maturation
- Improved follicular dendritic cell function holding antigen on display for affinity selection
Several preclinical studies in mice have shown that ginsenosides act on each of these steps, with the net effect of higher-titer and higher-affinity antibody responses to co-administered antigens. The clinical translation in the Scaglione trial — doubled antibody titers to influenza strains — is consistent with this mechanism.
The adjuvant effect has practical relevance beyond seasonal influenza vaccination. Elderly patients, immunosuppressed patients (post-organ-transplant, on chronic prednisone, on biologic immunomodulators for autoimmune disease), and patients with hypogammaglobulinemia all mount weaker antibody responses to vaccines. Ginseng pre-vaccination has been investigated as a strategy to improve vaccine responsiveness in these populations, with promising but preliminary results.
It is important to note that the FDA does not recommend any over-the-counter supplement specifically as a vaccine adjuvant, and patients should discuss any supplement use around vaccination with their clinician. For more on vaccination, see Immune Boosting.
Polysaccharides vs Ginsenosides — Two Active Fractions
One of the more interesting aspects of ginseng pharmacology is that the root contains two largely independent classes of bioactive molecules, both with immune-modulating activity:
- Ginsenosides — triterpene saponins, the better-studied class. ~30 individual ginsenosides have been characterized. Variable lipid-solubility; ginsenosides are absorbed (in part) intact through the gut wall and circulate systemically.
- Polysaccharides — complex sugar polymers, including beta-glucans, pectins, and arabinogalactans. Not absorbed intact (too large to cross the gut epithelium) but act locally on gut-associated lymphoid tissue (GALT) and through pattern-recognition receptor signaling. CVT-E002 (COLD-FX) is a polysaccharide-enriched preparation.
The two fractions activate different aspects of immune function and are likely additive in whole-root preparations. Most traditional ginseng preparations (decoctions, teas, whole-root powder) contain both. Modern standardized extracts vary: G115 is standardized for ginsenoside content but contains some polysaccharide; CVT-E002 is enriched for polysaccharide but contains some ginsenoside; ginsenoside-only purified preparations exist primarily in research settings.
For general winter-immune use, whole-root powder or extract is probably preferable to either pure fraction, since both immune mechanisms contribute and the practical clinical benefit of selecting one over the other has not been demonstrated.
Elderly Immune Decline (Immunosenescence)
Immune function declines with age in stereotyped ways: thymic involution reduces naive T-cell output, NK cell function declines, B-cell antibody response to vaccination weakens, and the cytokine environment shifts toward chronic low-grade inflammation ("inflammaging"). The net effect is increased susceptibility to viral infection (influenza, RSV, herpes zoster reactivation), reduced vaccine effectiveness, and slower recovery from infectious illness. The CDC and WHO data on influenza mortality concentrate the majority of deaths in adults over 65 for this reason.
Ginseng has been studied as an intervention for immunosenescence in multiple trials:
- McElhaney 2004 (CVT-E002 in nursing home residents) showed substantial reduction in acute respiratory illness
- McElhaney 2011 (CVT-E002 in elderly with COPD/CHF) showed reduced exacerbations
- Several small Korean red ginseng trials in elderly populations have shown improved NK cell function and reduced URI frequency
- Pre-vaccination ginseng dosing in elderly subjects has shown trends toward improved antibody response, though the elderly studies are smaller than the Scaglione 1996 trial in middle-aged adults
For elderly patients (particularly those over 75, in institutional settings, or with significant comorbidities), the case for ginseng as a routine winter-season immune support is reasonable. The Canadian regulatory acceptance of COLD-FX is partly based on this evidence base in elderly populations.
For more on healthy aging strategies, see Healthy Aging, Vitamin D3, and Zinc — all three of which have substantial evidence for supporting elderly immune function as well.
Dosing and Timing for Immune Use
Standard immune-support dosing varies by preparation:
- G115 standardized Panax ginseng extract — 100 mg twice daily, the Scaglione trial dose. Start 4-12 weeks before peak respiratory infection season (typically late October in temperate Northern Hemisphere) and continue through the season.
- CVT-E002 (COLD-FX) American ginseng polysaccharide — 200 mg twice daily as the routine dose; many sources recommend doubling to 400 mg twice daily at the first sign of cold symptoms ("rescue" dosing) for 3 days. Best evidence supports the routine prophylactic use rather than the rescue dose.
- Whole-root Korean red ginseng powder — 1-3 g/day, taken in the morning. Continuous through the cold/flu season.
- Whole-root American ginseng powder — 1-3 g/day, morning. Slightly preferred over Korean red for evening-shift workers and patients with significant anxiety or insomnia.
Timing relative to vaccination: if the goal is to enhance the antibody response to an influenza vaccine, the Scaglione protocol started ginseng 4 weeks before vaccination and continued for 8 weeks after. Practical recommendation: start ginseng in early October, get vaccinated in mid-October to early November, continue ginseng through January.
For acute use at the onset of cold symptoms, the evidence is weaker. The COLD-FX rescue protocol (400 mg twice daily for 3 days at the first cold symptom) has some marketing support but limited rigorous clinical evidence. The general principle is that ginseng works better prophylactically than therapeutically.
Cautions, Limitations, and Drug Interactions
- Immunosuppressant interaction — patients on cyclosporine, tacrolimus, methotrexate, biologic immunomodulators (anti-TNF agents, JAK inhibitors), or chronic prednisone face a theoretical interaction with ginseng's immune-activating effects. Discuss with the prescriber before starting ginseng. Most patients tolerate moderate doses without measurable interference with the immunosuppressant's effect, but blood-level monitoring may be warranted for narrow-therapeutic-window drugs.
- Autoimmune disease — theoretical concern that immune-activating herbs may worsen autoimmune conditions (lupus, rheumatoid arthritis, multiple sclerosis, type 1 diabetes). Clinical observation does not consistently support this concern with ginseng specifically, but patients with active autoimmune disease should approach immune-stimulating supplements cautiously.
- Active infection (bacterial) — ginseng is not a substitute for antibiotics in confirmed bacterial infection. Use ginseng for prevention and supportive care, not as primary therapy for streptococcal pharyngitis, pneumonia, urinary tract infection, or other bacterial conditions.
- Warfarin interaction — same caution as for all ginseng use. Monitor INR closely.
- Pregnancy — safety not established. Avoid in pregnancy. Postpartum use is sometimes considered for fatigue and immune support but should be discussed with the obstetric team.
- Insomnia — Korean red ginseng particularly can disrupt sleep if taken in the evening. Morning dosing only.
- Children — CVT-E002 has been studied at lower doses in children for cold prevention, with reasonable safety but limited efficacy data. Discuss with pediatrician before giving ginseng to children under 12.
Key Research Papers
- Scaglione F et al. (1996). Efficacy and safety of the standardised ginseng extract G115 for potentiating vaccination against the influenza syndrome and protection against the common cold. Drugs Under Experimental and Clinical Research. — PubMed
- Predy GN et al. (2005). Efficacy of an extract of North American ginseng containing poly-furanosyl-pyranosyl-saccharides for preventing upper respiratory tract infections: a randomized controlled trial. Canadian Medical Association Journal. — PubMed
- McElhaney JE et al. (2004). A placebo-controlled trial of a proprietary extract of North American ginseng (CVT-E002) to prevent acute respiratory illness in institutionalized older adults. Journal of the American Geriatrics Society. — PubMed
- McElhaney JE et al. (2011). Efficacy and safety of CVT-E002, a proprietary extract of Panax quinquefolius in the prevention of respiratory infections in influenza-vaccinated community-dwelling adults. Influenza and Other Respiratory Viruses. — PubMed
- High KP et al. (2012). A randomized, controlled trial of Panax quinquefolius extract (CVT-E002) to reduce respiratory infection in patients with chronic lymphocytic leukemia. Journal of Supportive Oncology. — PubMed
- Lee CS et al. (2014). Effects of Korean red ginseng on respiratory infections. Journal of Ginseng Research. — PubMed
- Yoo DG et al. (2012). Protective effect of ginseng polysaccharides on influenza viral infection. PLoS One. — PubMed
- Wang Y et al. (2010). Immunomodulatory effects of polysaccharides from Panax ginseng. International Immunopharmacology. — PubMed
- Kang S, Min H (2012). Ginseng, the immunity boost: the effects of Panax ginseng on immune system. Journal of Ginseng Research. — PubMed
- Lee JS et al. (2014). Salutary effect of Korean red ginseng on systemic inflammation. Journal of Ethnopharmacology. — PubMed
- Block KI, Mead MN (2003). Immune system effects of echinacea, ginseng, and astragalus: a review. Integrative Cancer Therapies. — PubMed
- Lim TS et al. (2002). Polysaccharide isolated from Panax ginseng induces apoptosis of human melanoma cells. Acta Pharmacologica Sinica. — PubMed
PubMed Topic Searches
- PubMed: Ginseng influenza vaccine
- PubMed: CVT-E002 / COLD-FX trials
- PubMed: Ginsenoside NK cells
- PubMed: Ginseng polysaccharide macrophage
- PubMed: Ginseng immunosenescence
Connections
- Ginseng Overview
- Ginseng Benefits Hub
- Ginseng for Fatigue
- Ginseng for Cognition
- Ginseng for ED
- Astragalus (Sister Immune Tonic)
- Andrographis
- Elderberry
- Echinacea
- Immune Boosting
- Vitamin C
- Vitamin D3
- Zinc
- Healthy Aging
- Pneumonia
- Influenza