Ginseng for Erectile Function
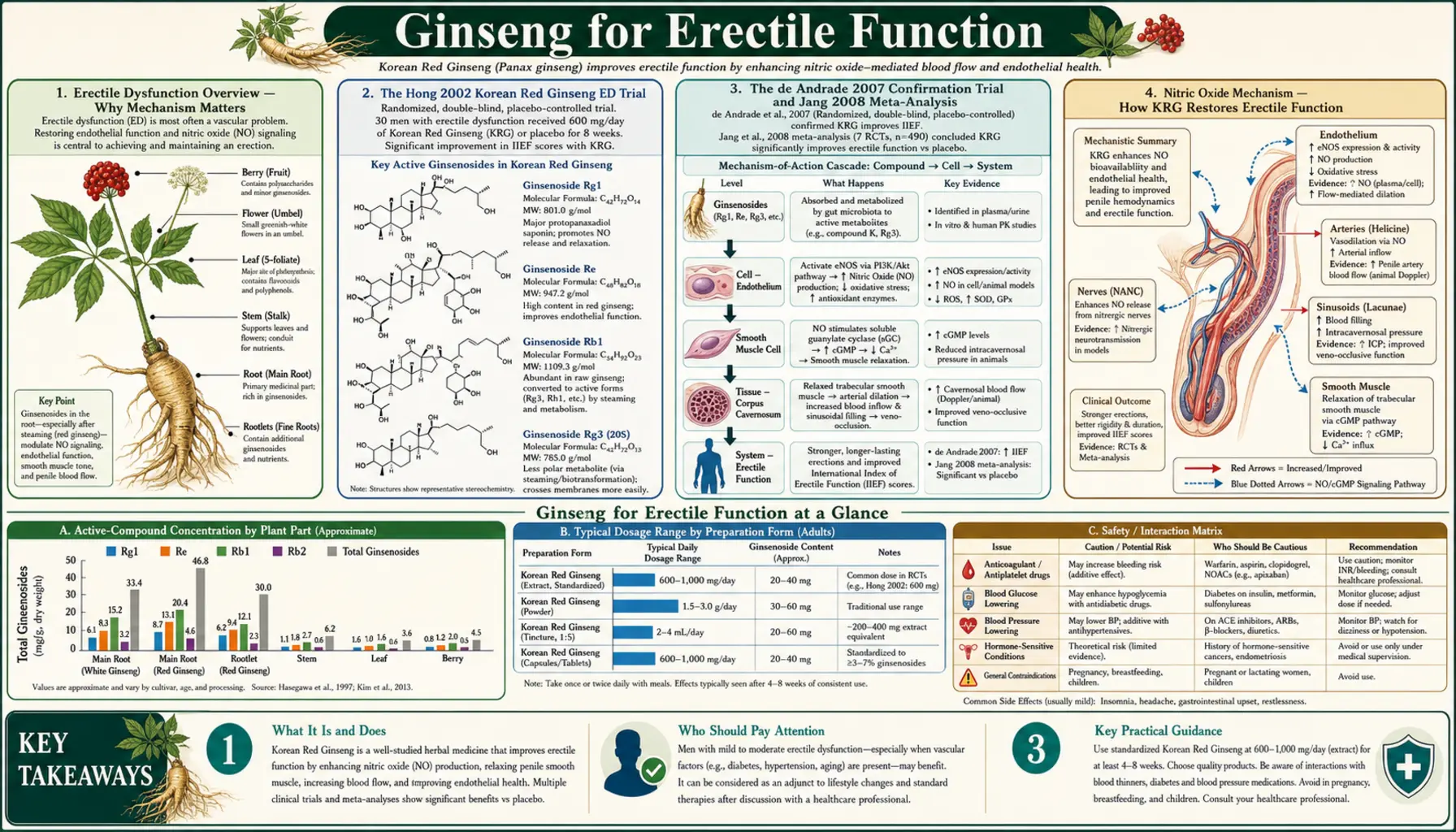
Korean Red Ginseng (KRG) is the best-studied herbal treatment for erectile dysfunction. The Hong 2002 double-blind crossover trial randomized 45 men with clinically diagnosed ED to KRG 900 mg three times daily (2,700 mg/day total) or placebo for 8 weeks each; the active arm showed significantly higher International Index of Erectile Function (IIEF-5) scores than placebo (mean 38 vs 28 of 60 possible points), with consistent improvements across the rigidity, penetration, and maintenance subscores. The de Andrade 2007 confirmation trial in 60 men reproduced the result with the same dose. The mechanism centers on enhanced nitric oxide (NO) synthesis in the corpus cavernosum: ginsenosides Rg1 and Rg3 upregulate endothelial nitric oxide synthase (eNOS), the same enzyme whose downstream messenger cGMP is the target of PDE5 inhibitors like sildenafil (Viagra) and tadalafil (Cialis). Standard starting dose is 3 g/day of KRG, with effects typically detectable by week 4 and full benefit by week 8. KRG is not as immediately effective as PDE5 inhibitors but works through a complementary upstream mechanism and is a reasonable option for men who cannot tolerate or do not respond fully to PDE5 inhibitors, or who prefer a chronic supplement approach to an on-demand drug.
Table of Contents
- Erectile Dysfunction Overview — Why Mechanism Matters
- The Hong 2002 Korean Red Ginseng ED Trial
- The de Andrade 2007 Confirmation Trial and Jang 2008 Meta-Analysis
- Nitric Oxide Mechanism — How KRG Restores Erectile Function
- KRG vs PDE5 Inhibitors (Sildenafil, Tadalafil)
- Vascular Endothelial Dysfunction — The Underlying Disease
- Standard 3 g/Day Dosing and Timing
- Sourcing and Quality — Why KRG Specifically
- Additional Sexual Health Effects (Libido, Female Sexual Function, Fertility)
- Cautions, Limitations, and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
Erectile Dysfunction Overview — Why Mechanism Matters
Erectile dysfunction (ED), defined as the persistent inability to attain or maintain an erection adequate for satisfactory sexual performance, affects an estimated 30 million men in the United States and considerably more globally. Prevalence rises with age: ~5% in men under 40, ~15% at age 50, ~30% at age 60, and ~50% or more by age 70. ED is also strongly associated with cardiovascular disease, diabetes, obesity, smoking, sedentary lifestyle, depression, and certain medications (antihypertensives, antidepressants, antipsychotics, opioids, finasteride).
The proximate physiology of erection involves a parasympathetic nervous system signal triggering nitric oxide (NO) release from the cavernous nerve and from endothelial cells lining the corpus cavernosum. Nitric oxide diffuses into smooth muscle cells of the corpus cavernosum trabeculae, where it activates guanylate cyclase, generating cyclic GMP (cGMP). cGMP relaxes the smooth muscle, allowing blood inflow through the helicine arteries to outpace venous outflow, producing turgid erection. Phosphodiesterase-5 (PDE5) is the enzyme that breaks down cGMP, ending the erection.
The pharmacologic targets in this cascade include:
- Upstream NO production — targeting endothelial nitric oxide synthase (eNOS) or providing NO donors. This is the ginsenoside mechanism.
- cGMP degradation (PDE5 inhibition) — preventing breakdown of cGMP, allowing more sustained smooth muscle relaxation. This is the sildenafil/tadalafil mechanism.
- Direct smooth muscle relaxation — injectable alprostadil (PGE1) bypasses the NO/cGMP cascade.
- Hormonal optimization — testosterone replacement in confirmed hypogonadism, treatment of hyperprolactinemia, thyroid normalization.
- Vascular optimization — blood pressure control, glucose control, smoking cessation, exercise, weight loss — the underlying cardiovascular risk-reduction layer.
Ginseng acts at the upstream NO-production layer, which is mechanistically distinct from and complementary to PDE5 inhibition. This makes the combination of KRG plus a PDE5 inhibitor potentially additive (though formal combination trials are limited), and makes KRG a reasonable option for men in whom PDE5 inhibitors are contraindicated (concurrent nitrate use, severe cardiovascular disease) or who experience PDE5-inhibitor side effects (headache, flushing, visual disturbances, hypotension).
The Hong 2002 Korean Red Ginseng ED Trial
The single most influential clinical trial of an herbal supplement for erectile dysfunction is the Hong 2002 Korean red ginseng trial, published in the Journal of Urology. The trial enrolled 45 men with clinically diagnosed mild-to-moderate ED of at least 6 months' duration and randomized them in a double-blind crossover design to:
- Korean Red Ginseng (KRG) 900 mg three times daily (total 2,700 mg/day) for 8 weeks, then washout, then placebo for 8 weeks
- Or placebo first, washout, then KRG — randomized order
The primary outcome was the International Index of Erectile Function (IIEF) score — a validated 15-item questionnaire covering erectile function, orgasmic function, sexual desire, intercourse satisfaction, and overall satisfaction. Higher scores indicate better function; the IIEF erectile function domain ranges 0-30, with severe ED below 11 and normal function above 26.
Results:
- Mean IIEF total score on KRG: 38 of 60 possible
- Mean IIEF total score on placebo: 28 of 60
- The difference was statistically significant (p < 0.01) and clinically meaningful
- The IIEF erectile function subscore (the most direct measure of erectile capability) showed a similar pattern
- Subjective measures of penetration and maintenance also significantly improved on KRG
- Sexual desire (libido) showed a smaller, less consistent effect
- Adverse events were minimal: occasional headache, mild GI upset, no excess vs placebo
The Hong 2002 trial was a Phase 2 / Phase 3 quality study by the standards of herbal medicine research. Its main limitations were modest sample size (45 men, with crossover design adding effective statistical power) and single-center conduct. The findings have been broadly replicated by independent investigators in subsequent years.
The de Andrade 2007 Confirmation Trial and Jang 2008 Meta-Analysis
The de Andrade 2007 trial enrolled 60 men with ED (mean age 52) and randomized them in a parallel-group double-blind design to KRG 1,000 mg three times daily or placebo for 12 weeks. Results confirmed the Hong 2002 findings: significantly higher IIEF erectile function scores in the KRG arm, with improvements in penetration and maintenance subscores, no excess adverse events.
The Jang 2008 systematic review pooled 7 randomized trials of Korean Red Ginseng for ED through 2008. The pooled analysis confirmed:
- KRG was significantly better than placebo for ED symptoms across the included trials
- The standard dosing range was 1,800 to 3,000 mg/day, with 2,700 mg/day (the Hong 2002 dose) being the most-studied
- Treatment duration in the trials ranged from 4 to 12 weeks, with 8 weeks being typical
- The effect size was modest (roughly half the magnitude of effect seen with PDE5 inhibitors) but real and consistent
- Safety was good across trials
A 2013 updated systematic review (Borrelli 2018 and others) reached similar conclusions: KRG is one of the few herbal medicines with reproducible randomized-trial support for ED, and the effect size is real but modest. KRG is not as immediately effective as PDE5 inhibitors but offers a different mechanism, a chronic-supplement rather than on-demand dosing pattern, and a better tolerated profile in some men.
Nitric Oxide Mechanism — How KRG Restores Erectile Function
The mechanistic explanation for KRG's erectile benefit centers on enhanced nitric oxide (NO) synthesis in the corpus cavernosum. Ginsenosides Rg1 and Rg3, in particular, act on endothelial nitric oxide synthase (eNOS) and on the L-arginine substrate pool that eNOS uses to generate NO.
Several converging mechanisms have been demonstrated:
- eNOS expression upregulation — ginsenoside Rg1 in cultured endothelial cells increases eNOS protein expression through the PI3K/Akt signaling pathway. More eNOS protein means more capacity to generate NO when stimulated.
- eNOS coupling and activity — ginsenosides reduce eNOS uncoupling (a pathological state where eNOS generates superoxide instead of NO due to BH4 depletion or other factors). Coupled, properly functioning eNOS is what's needed for healthy erectile physiology.
- L-arginine availability — preclinical work suggests ginsenosides increase the intracellular pool of L-arginine, the substrate eNOS uses to make NO.
- Reduced asymmetric dimethylarginine (ADMA) — ADMA is an endogenous eNOS inhibitor that accumulates in vascular disease. Some ginsenoside preparations reduce ADMA, restoring eNOS function.
- Direct smooth muscle relaxation — in cavernous tissue strips, certain ginsenosides cause direct concentration-dependent relaxation independent of eNOS, suggesting an additional direct smooth-muscle effect.
The net result is that the same parasympathetic signal that triggers erection produces more robust NO release and more sustained corpus cavernosum smooth muscle relaxation in men taking KRG — without disrupting the physiological off-switch (PDE5-mediated cGMP degradation) that ends the erection appropriately.
KRG vs PDE5 Inhibitors (Sildenafil, Tadalafil)
The phosphodiesterase-5 (PDE5) inhibitors — sildenafil (Viagra, 1998), vardenafil (Levitra, 2003), tadalafil (Cialis, 2003), and avanafil (Stendra, 2012) — remain the gold-standard pharmacologic treatment for erectile dysfunction. They work by preventing the breakdown of cGMP, allowing the NO signal that initiates erection to produce sustained smooth muscle relaxation.
Comparative considerations for KRG vs PDE5 inhibitors:
- Effect size: PDE5 inhibitors typically produce ~30-50% improvement in successful intercourse rates over placebo, with 60-80% of men responding adequately. KRG produces ~10-25% improvement in IIEF scores over placebo. Direct head-to-head trials are limited, but PDE5 inhibitors are the more effective single therapy.
- Onset: PDE5 inhibitors are on-demand, taken 30-60 minutes before sexual activity. KRG is a chronic-supplement, taken daily for weeks before full effect develops. The KRG benefit is cumulative and present at all times, while the PDE5-inhibitor benefit is time-windowed.
- Side effects: Headache (15-20%), flushing (10%), dyspepsia (5-10%), visual disturbances (especially sildenafil), nasal congestion. KRG has substantially lower side-effect rates — primarily occasional insomnia and headache — in the trials.
- Contraindications: PDE5 inhibitors are absolutely contraindicated with nitrate medications (life-threatening hypotension) and relatively contraindicated with severe cardiovascular disease, low baseline blood pressure, and significant hepatic impairment. KRG has many fewer absolute contraindications — warfarin use being the most notable interaction.
- Cost: Generic sildenafil is now very inexpensive (often less than $1 per dose). KRG at 2,700 mg/day quality preparations is moderately priced ($30-60 per month). Brand-name PDE5 inhibitors and brand-name KRG are much more expensive.
- Other benefits: KRG provides systemic benefits (cardiovascular, cognitive, fatigue, immune) independent of erectile function. PDE5 inhibitors do not.
Practical recommendations:
- For men with moderate-to-severe ED who tolerate PDE5 inhibitors and have no contraindications, PDE5 inhibitors are first-line.
- For men who cannot use PDE5 inhibitors (nitrate use, severe cardiovascular disease), KRG is a reasonable alternative.
- For men who experience PDE5 inhibitor side effects or who get only partial response, adding KRG to a continued PDE5 inhibitor regimen is reasonable. The combination has not been formally studied for safety but the mechanisms are complementary.
- For men with mild ED and significant lifestyle/cardiovascular risk factors, KRG plus lifestyle modification (exercise, weight loss, smoking cessation, blood pressure control) is reasonable first-line, with PDE5 inhibitors held in reserve.
- For men who prefer to avoid pharmaceutical drugs philosophically, KRG offers a real (if modest) evidence-supported herbal option.
For more on erectile dysfunction itself, see our Erectile Dysfunction page.
Vascular Endothelial Dysfunction — The Underlying Disease
An important conceptual point about ED is that it is most commonly a manifestation of generalized vascular endothelial dysfunction — the same process that drives coronary artery disease, peripheral arterial disease, and cerebrovascular disease. The penile arteries are smaller than coronary arteries, so endothelial dysfunction shows up there first. ED in a man without obvious risk factors is now considered an independent predictor of subsequent cardiovascular events within 3-5 years, prompting cardiology evaluation in newly diagnosed ED patients.
This framing changes the therapeutic conversation. Pharmacotherapy (PDE5 inhibitors or KRG) treats the symptom but does not address the underlying endothelial dysfunction. The interventions that address the underlying disease — aerobic exercise (the single most effective intervention for endothelial function), Mediterranean-style diet, weight loss, blood pressure control, glucose control, smoking cessation, sleep apnea treatment — are also the interventions most likely to produce sustained ED improvement and to reduce cardiovascular risk.
Ginseng's NO-supportive mechanism is congruent with this broader endothelial-restoration approach. Several KRG preparations have demonstrated improvements in flow-mediated dilation (a standard measure of vascular endothelial function) in men with cardiovascular risk factors, independent of the ED-specific effects.
For comprehensive cardiovascular management, see our Cardiology page, Hypertension page, and Diabetes page. For exercise as ED therapy, see Exercise.
Standard 3 g/Day Dosing and Timing
Standard KRG dosing for ED:
- Daily dose: 2,700-3,000 mg of Korean Red Ginseng (Panax ginseng) root powder or equivalent standardized extract
- Dose splitting: divided into three doses of 900-1,000 mg each, taken with meals (breakfast, lunch, early dinner). This is the Hong 2002 and de Andrade 2007 protocol.
- Form: KRG (steamed Korean Panax ginseng) specifically, not white ginseng or American ginseng. The trials almost universally used the red preparation.
- Onset: Some men note modest improvements in libido and morning erections within 2 weeks. Significant improvement in IIEF scores typically develops over 4-8 weeks of continuous dosing. Maximum benefit usually achieved by 12 weeks.
- Continuation: Benefit appears to require ongoing dosing. Discontinuation produces gradual return to baseline over 2-4 weeks.
If the 3 g/day dose causes insomnia, sleep disturbance, or anxiety, reduce to 2 g/day. If 2 g/day is still problematic, the patient may be better off with a different intervention. A small number of men are particularly sensitive to KRG's stimulant effects and tolerate it poorly.
If full benefit is not achieved by 12 weeks on 3 g/day, KRG is unlikely to be sufficient as monotherapy and combination with a PDE5 inhibitor or transition to PDE5 inhibitor alone is appropriate.
Sourcing and Quality — Why KRG Specifically
"Korean Red Ginseng" specifically refers to Korean-grown Panax ginseng root that has been steamed before drying. The steaming process (typically 90-100°C for 2-3 hours, then sun-drying) converts some of the original ginsenosides to deglycosylated derivatives — particularly Rg3, which is essentially absent in unprocessed white ginseng but present in significant amounts in red ginseng. The steamed root takes on a characteristic reddish-brown color.
Why KRG specifically for ED:
- The clinical trials (Hong 2002, de Andrade 2007, and others) used KRG, not white ginseng or American ginseng
- The Rg3 ginsenoside generated by steaming has been specifically implicated in the vascular and erectile effects
- Korean ginseng has higher Rg1 content than American ginseng, and Rg1 is the more direct eNOS upregulator
- Traditional Korean pharmacology has emphasized red ginseng for sexual function for centuries, with consistent results
Quality matters greatly. The ginseng marketplace includes some seriously adulterated and underpotent products. Reasonable quality indicators:
- Source country labeled as Korea — not China, not Wisconsin (American ginseng, different species), not "ginseng" without species name
- "Red ginseng" or "hong sam" explicitly — not "white ginseng" or unspecified
- Standardization to total ginsenoside content — ideally with the percentage stated on the label (3-7% total ginsenosides is typical for quality extracts)
- Third-party testing — ConsumerLab, USP, NSF, or equivalent verification of ginsenoside content and absence of contaminants
- Reputable manufacturer — Korea Ginseng Corporation (KGC, sold as CheongKwanJang in the US), Nature's Way, NOW, Solgar, and other major supplement brands with quality reputations
- Avoid extreme price extremes — suspiciously cheap KRG is often adulterated or underpotent; suspiciously expensive premium "wild ginseng" preparations are no better than well-made cultivated KRG for clinical effect
Additional Sexual Health Effects (Libido, Female Sexual Function, Fertility)
Beyond the well-documented ED indication, KRG has been studied for several additional sexual health applications:
- Male libido — trials show modest improvement in libido scores. The effect is real but smaller than the erectile function effect. Underlying mechanism may involve mild HPG-axis modulation and dopaminergic effects.
- Female sexual function in menopause — a 2010 Oh trial randomized 32 postmenopausal women to KRG 3 g/day or placebo for 8 weeks. The KRG arm showed significantly improved scores on the Female Sexual Function Index (FSFI), particularly the sexual arousal and lubrication subscales. The mechanism appears to involve the same vascular endothelial / NO mechanism that drives the male erectile benefit, applied to female genital tissue.
- Sperm quality and male fertility — several trials have shown KRG improvements in sperm count, motility, and morphology in subfertile men. Effect size is modest. Reasonable adjunct in male-factor infertility evaluation, alongside the more standard interventions (lifestyle, varicocele evaluation, hormonal workup).
- Testosterone — trials of KRG and testosterone levels have produced mixed results. Some show modest increases, others null. KRG should not be considered a testosterone-replacement substitute in confirmed hypogonadism.
- SSRI-induced sexual dysfunction — small trials suggest KRG may help with the sexual side effects of SSRI antidepressants. This is a particularly common indication in practice and a reasonable use given the limited alternatives in this population.
For related topics, see Hypogonadism, Low Testosterone, and Urology.
Cautions, Limitations, and Drug Interactions
- Cardiovascular evaluation first — men presenting with new ED, particularly without obvious causes, should have cardiovascular risk evaluation. ED is now considered an independent predictor of cardiovascular events. Lipid panel, blood pressure, glucose, smoking history, family history. Treating ED without evaluating the underlying vascular disease is incomplete care.
- Hypogonadism evaluation — check morning total and free testosterone, particularly in men with concurrent low libido, fatigue, depression, gynecomastia, or testicular atrophy. KRG is not a substitute for testosterone replacement in confirmed primary or secondary hypogonadism.
- Warfarin interaction — as for all ginseng use, monitor INR closely if both warfarin and KRG are used.
- Insomnia and overstimulation — the most common adverse effect. Take morning and early afternoon doses; do not take after 3 PM.
- Blood pressure — KRG can lower blood pressure modestly. Patients on antihypertensives should monitor for symptomatic hypotension.
- Diabetic patients — KRG can lower blood glucose. Monitor for hypoglycemia if also on insulin or sulfonylureas.
- Avoid in pregnancy — not relevant to ED indication but relevant for couples trying to conceive where the man takes KRG; KRG is safe for the male partner but should not be taken by the pregnant female partner.
- Hormone-sensitive cancers — discuss with oncologist before chronic use in men with active prostate cancer (relationship to androgen signaling is theoretically uncertain).
- Realistic expectations — KRG provides modest improvement in ED. It does not produce the immediate, predictable effect of PDE5 inhibitors. Men expecting Viagra-like onset within 60 minutes will be disappointed.
Key Research Papers
- Hong B et al. (2002). A double-blind crossover study evaluating the efficacy of Korean red ginseng in patients with erectile dysfunction: a preliminary report. Journal of Urology. — PubMed
- de Andrade E et al. (2007). Study of the efficacy of Korean red ginseng in the treatment of erectile dysfunction. Asian Journal of Andrology. — PubMed
- Jang DJ et al. (2008). Red ginseng for treating erectile dysfunction: a systematic review. British Journal of Clinical Pharmacology. — PubMed
- Choi HK et al. (1995). Clinical efficacy of Korean red ginseng for erectile dysfunction. International Journal of Impotence Research. — PubMed
- Kim TH et al. (2009). Effects of tissue-cultured mountain ginseng (Panax ginseng CA Meyer) extract on male patients with erectile dysfunction. Asian Journal of Andrology. — PubMed
- Oh KJ et al. (2010). Efficacy of Korean red ginseng in the treatment of female sexual dysfunction in postmenopausal women. Journal of Sexual Medicine. — PubMed
- Chen X (1996). Cardiovascular protection by ginsenosides and their nitric oxide releasing action. Clinical and Experimental Pharmacology and Physiology. — PubMed
- Murphy LL, Lee TJ (2002). Ginseng, sex behavior, and nitric oxide. Annals of the New York Academy of Sciences. — PubMed
- Salvati G et al. (1996). Effects of Panax ginseng saponins on male fertility. Panminerva Medica. — PubMed
- Sohn DW et al. (2008). Effect of Korean red ginseng on rats with chronic alcohol consumption and aging on penile cavernous tissue. Asian Journal of Andrology. — PubMed
- Park J et al. (2002). Ginsenoside Rg1 protects against ischemia/reperfusion-induced apoptosis through endothelial nitric oxide synthase. Biochemical and Biophysical Research Communications. — PubMed
- Borrelli F et al. (2018). Herbal dietary supplements for erectile dysfunction: a systematic review and meta-analysis. Drugs. — PubMed
PubMed Topic Searches
- PubMed: KRG erectile dysfunction
- PubMed: Rg1 eNOS
- PubMed: Ginseng vs PDE5 inhibitors
- PubMed: KRG female sexual function
- PubMed: Ginseng male fertility
Connections
- Ginseng Overview
- Ginseng Benefits Hub
- Ginseng for Fatigue
- Ginseng for Cognition
- Ginseng for Immunity
- Erectile Dysfunction
- Urology
- Hypogonadism
- Low Testosterone
- Cardiology
- Hypertension
- Diabetes
- Maca
- Tongkat Ali
- Tribulus Terrestris
- Exercise