Ginger for Nausea Relief
Nausea is ginger's most evidence-backed indication — and the one where ginger directly competes with first-line pharmacology. Three pivotal randomized trials anchor the literature: Vutyavanich's 2001 Thai obstetric trial established 250 mg four times daily as the foundational dose for nausea and vomiting in pregnancy (where almost every conventional antiemetic is either teratogenic or relatively contraindicated). Chaiyakunapruk's 2006 meta-analysis of postoperative nausea and vomiting (PONV) showed effect sizes comparable to droperidol and metoclopramide. Marx's 2013 systematic review documented benefit in chemotherapy-induced nausea and vomiting (CINV) as an adjunct to 5-HT3 antagonist therapy. The unifying mechanism: ginger compounds are themselves 5-HT3 receptor antagonists, the same molecular target as ondansetron (Zofran) — not an analog, the actual same receptor.
Table of Contents
- Why Nausea Matters — The Clinical Burden
- The 5-HT3 Mechanism (Same Target as Zofran)
- Vutyavanich 2001 — The Pregnancy Foundation Trial
- Hyperemesis Gravidarum — The Severe End of Pregnancy Nausea
- Chaiyakunapruk 2006 — Postoperative Nausea Meta-Analysis
- Marx 2013 — Chemotherapy-Induced Nausea Meta-Analysis
- Motion Sickness — The Original Mowrey 1982 Lancet Trial
- Vestibular vs. Chemoreceptor Nausea — Where Ginger Works Best
- Practical Dosing — Forms, Timing, Routes
- Cautions and Contraindications
- Key Research Papers
- Connections
- Featured Videos
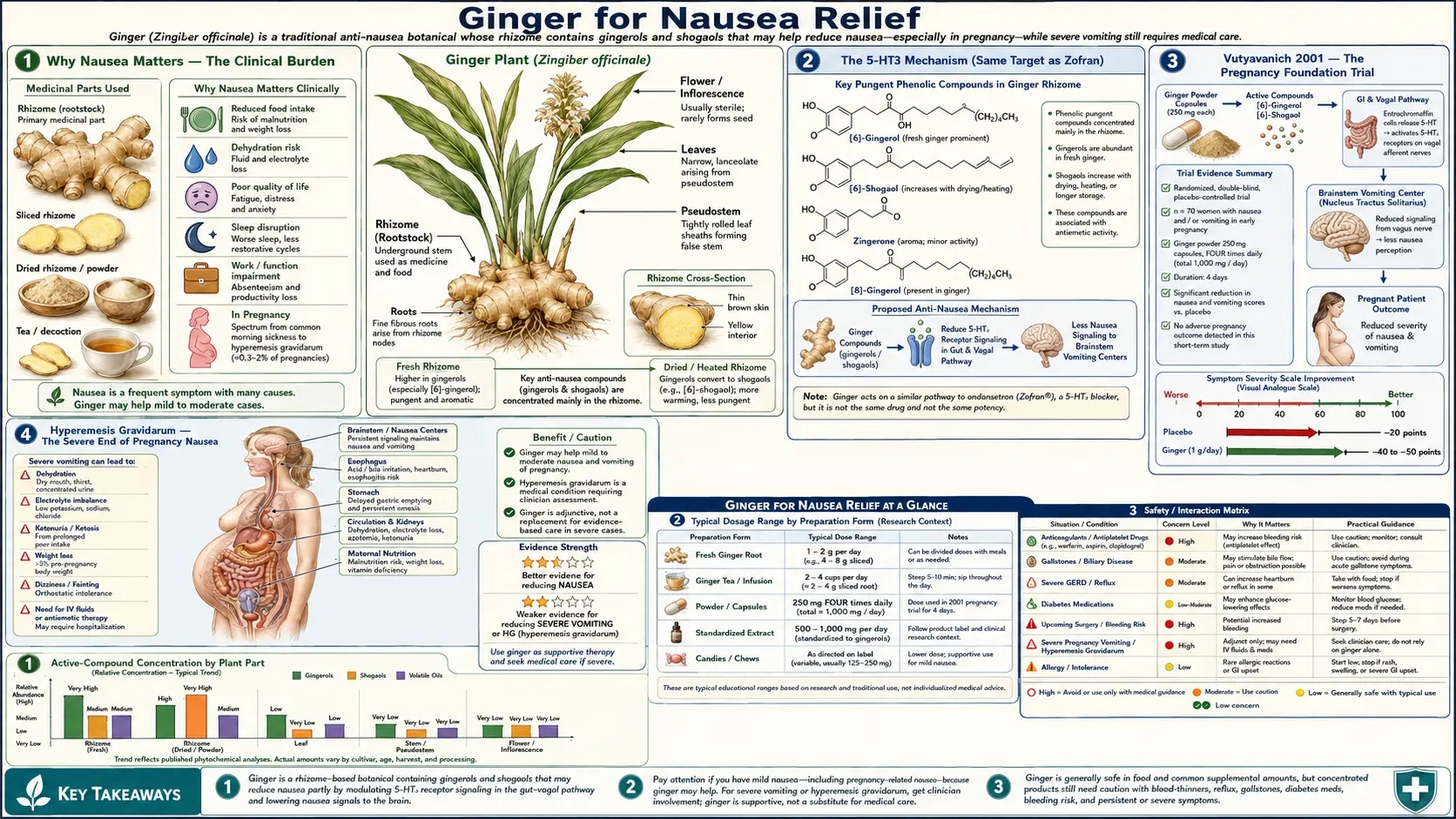
Why Nausea Matters — The Clinical Burden
Nausea is the most common symptom in clinical medicine after pain. Roughly 70–80% of pregnant women experience it (with about 1% progressing to hyperemesis gravidarum requiring hospitalization), 30–50% of post-surgical patients develop postoperative nausea/vomiting, and over 80% of patients on moderately or highly emetogenic chemotherapy report nausea despite standard prophylaxis. Beyond the immediate suffering, untreated nausea drives dehydration, electrolyte derangement, weight loss, treatment non-adherence, and (in chemotherapy patients) outright refusal of further cycles — with measurable impact on cancer survival.
The pharmacologic challenge is that the "perfect" antiemetic does not exist. Ondansetron (Zofran) is highly effective but can cause QT prolongation (FDA warning at higher doses) and constipation, and is unproven for the chronic-low-dose ambulatory use needed in pregnancy. Metoclopramide carries a black-box warning for tardive dyskinesia after chronic use. Prochlorperazine and promethazine cause significant sedation. Scopolamine patches dry every mucous membrane. Cannabinoids are useful but have their own side-effect spectrum and legal complications. Aprepitant is expensive and reserved for highly emetogenic chemotherapy.
Ginger's role is not to displace any of these drugs — it is to occupy the niche where conventional drugs are contraindicated (pregnancy), poorly tolerated (chronic ambulatory use), or simply additive (CINV adjunctive therapy alongside ondansetron and dexamethasone). The evidence base for that niche has been built up over four decades and three positive meta-analyses.
The 5-HT3 Mechanism (Same Target as Zofran)
The 5-HT3 receptor is a ligand-gated cation channel (not a G-protein-coupled receptor like most other serotonin receptors) expressed at high density in two anatomical locations critical to vomiting:
- Vagal afferent terminals in the gut wall — enterochromaffin cells in the intestinal epithelium release serotonin in response to mucosal irritation (chemotherapy, distention, toxin exposure). Released 5-HT binds 5-HT3 receptors on adjacent vagal afferent terminals, generating the afferent signal that travels via the nodose ganglion to the dorsal vagal complex of the brainstem.
- The chemoreceptor trigger zone (CTZ) in the area postrema — a circumventricular brainstem region with no blood-brain barrier, allowing direct sensing of blood-borne emetic stimuli. 5-HT3 receptors here couple directly to the vomiting center in the nucleus tractus solitarius (NTS).
Ondansetron, granisetron, palonosetron, and tropisetron are all competitive 5-HT3 antagonists; they bind the receptor and block the serotonin signal. They are the dominant first-line agents for chemotherapy-induced nausea precisely because chemotherapy works largely through massive gut-mucosal serotonin release.
Ginger compounds (gingerols and shogaols) demonstrate competitive 5-HT3 antagonism in radioligand binding studies and functional whole-cell patch-clamp experiments. The affinity is lower than ondansetron's (gingerols are weak partial antagonists in the micromolar range, vs. ondansetron at low nanomolar), but the clinical effect is real and additive when combined with conventional 5-HT3 antagonists. This is why the chemotherapy literature consistently shows ginger plus standard antiemetic prophylaxis outperforming standard prophylaxis alone, rather than ginger replacing it.
Ginger compounds also act at the muscarinic M3 receptor on enteric smooth muscle (relevant to the prokinetic effect discussed in the Digestive Aid & Gastroparesis page) and at the NK1 (substance P) receptor — the same target as aprepitant. The NK1 activity is modest but contributes to the broad-spectrum antiemetic profile.
Vutyavanich 2001 — The Pregnancy Foundation Trial
The Vutyavanich randomized, double-masked, placebo-controlled trial published in Obstetrics & Gynecology in 2001 remains the foundational pregnancy ginger study. Seventy women in the first trimester with nausea and vomiting of pregnancy (NVP) were randomized to either 250 mg ginger powder capsules four times daily (1 g per day total) or matching placebo, for 4 days. Outcomes:
- Nausea scores (visual analog scale) decreased significantly more in the ginger group (p = 0.014)
- Number of vomiting episodes decreased more in the ginger group (p < 0.001)
- No statistically significant difference in pregnancy outcomes between groups
- No serious adverse events in either group
The 250 mg QID dose has become the de facto standard for pregnancy nausea in every subsequent trial and guideline (American College of Obstetricians and Gynecologists, the German Society for Gynecology and Obstetrics, the European Medicines Agency monograph), although several follow-up studies have used 500 mg BID or 350 mg TID with comparable results. The total daily dose of 1–1.5 g of ginger powder is the operative target; the specific dosing interval is less critical.
The American College of Obstetricians and Gynecologists Practice Bulletin on NVP recommends ginger as a first-line non-pharmacologic intervention, alongside vitamin B6 (pyridoxine) 10–25 mg every 6–8 hours. The combination of B6 plus doxylamine (Diclegis / Bonjesta) is the only FDA-approved drug for NVP; ginger is the only evidence-supported herbal option at the same evidence tier.
One important distinction: the Vutyavanich trial used powdered dried ginger root in capsules, not ginger tea, candied ginger, or ginger ale. The ginger content of commercial ginger ale is essentially negligible (most contain only ginger flavoring extract, not measurable amounts of gingerols), and the sugar load is counterproductive. Crystallized ginger candy contains real ginger but at unpredictable doses. Capsulated standardized powder at 250 mg per cap is the format that matches the trial evidence.
Hyperemesis Gravidarum — The Severe End of Pregnancy Nausea
Hyperemesis gravidarum (HG) is the severe end of the NVP spectrum — intractable vomiting causing >5% weight loss, ketonuria, electrolyte disturbance, and often requiring hospitalization for IV fluid and antiemetic therapy. It affects roughly 0.3–3% of pregnancies, with substantially higher rates in twin pregnancies, women with a personal or family history of HG, and women with prior hyperemesis (recurrence rate >80% in subsequent pregnancies).
The first-line pharmacologic approach for HG escalates from doxylamine/B6, to promethazine or dimenhydrinate, to ondansetron, to corticosteroids, to (rarely) total parenteral nutrition. Ginger sits as an adjunct at the lower rungs of this escalation. The 2014 Cochrane review of NVP interventions found ginger "may improve symptoms" in mild-to-moderate NVP, with the evidence less robust at the severe HG end of the spectrum — not because ginger fails there, but because trial enrollment of severely symptomatic women is logistically difficult (they tend to be hospitalized and unable to tolerate any oral intake).
Some practical clinical wisdom on the severe end: ginger oil aromatherapy (a few drops on a tissue held near the nose) and ginger lozenges are sometimes tolerated when capsules are not, simply because they bypass the gastric absorption that may be the proximate trigger. Ginger tea brewed thin and consumed in sips may be tolerated for the same reason.
For the very severe end — the women who are hospitalized for HG, on IV ondansetron, and still vomiting — ginger is not going to be the rescue therapy. But for the mild-to-moderate first-trimester nausea that affects 70% of pregnancies, the evidence is strong enough that the ACOG and most international obstetric societies recommend it as first-line non-pharmacologic therapy.
Chaiyakunapruk 2006 — Postoperative Nausea Meta-Analysis
Postoperative nausea and vomiting (PONV) affects roughly 30% of all surgical patients and up to 80% in high-risk groups (women, non-smokers, history of motion sickness or prior PONV, opioid use, certain surgery types — laparoscopic, gynecologic, ENT). PONV is the most common reason for unplanned hospital admission after ambulatory surgery and the single most common patient-cited dissatisfaction with anesthesia care.
Chaiyakunapruk and colleagues published a meta-analysis in 2006 (American Journal of Obstetrics & Gynecology) pooling 5 randomized controlled trials with a total of 363 patients, examining preoperative ginger (typically 1 g of ginger powder given 1 hour before surgery induction). Findings:
- Ginger reduced the relative risk of PONV by approximately 31% vs placebo (RR 0.69, 95% CI 0.54–0.89)
- Effect size was comparable to metoclopramide 10 mg IV
- No significant adverse events attributable to ginger
- Effect was particularly pronounced in gynecologic and laparoscopic surgery populations
Subsequent meta-analyses (Lee & Chua 2018, Toth et al. 2018) have confirmed and slightly refined these findings. The optimal dose appears to be 1 g ginger powder taken approximately 1 hour preoperatively, with no clear additional benefit at higher doses (some evidence for diminishing returns above 2 g).
The contemporary anesthesia practice does not yet routinely incorporate preoperative ginger — the established standard of care is multimodal prophylaxis with 5-HT3 antagonists (ondansetron 4 mg IV), dexamethasone (4–8 mg IV), and droperidol (low dose, 0.625 mg IV) for high-risk patients. Ginger has an emerging role as an additional layer of prophylaxis or as an alternative in patients for whom the standard agents are contraindicated.
Marx 2013 — Chemotherapy-Induced Nausea Meta-Analysis
Chemotherapy-induced nausea and vomiting (CINV) is one of the most feared side effects of cancer therapy. Despite the introduction of 5-HT3 antagonists in the 1990s and NK1 antagonists (aprepitant) in the 2000s, roughly 50% of patients on moderately or highly emetogenic chemotherapy still report significant nausea, particularly the delayed phase (24–120 hours post-infusion) where 5-HT3 antagonists are less effective.
The Marx 2013 systematic review in Nutrition Reviews examined 7 randomized clinical trials of ginger as adjunctive therapy for CINV. The headline finding: ginger added to standard 5-HT3 antagonist prophylaxis (most commonly ondansetron) significantly reduced acute and delayed nausea severity, with the largest effect in the delayed phase where it complements rather than competes with the 5-HT3 antagonist mechanism.
The Ryan et al. 2012 URCC CCOP (University of Rochester Cancer Center Community Clinical Oncology Program) trial deserves specific mention: 576 cancer patients beginning chemotherapy were randomized to one of four arms (placebo or ginger 0.5 g, 1.0 g, or 1.5 g daily, starting 3 days before chemotherapy and continuing through the chemotherapy cycle). All arms also received standard 5-HT3 antagonist prophylaxis. Results:
- All ginger doses reduced acute nausea severity vs placebo (p < 0.003)
- The 0.5 g and 1.0 g doses produced the largest effect; 1.5 g did not provide additional benefit
- Effects were strongest on day 1 of the chemotherapy cycle
- Tolerability was excellent across all arms
The Ryan trial established the practical dosing for CINV: 0.5–1.0 g of ginger powder daily, divided BID or TID, starting 3 days before chemotherapy infusion and continuing for the first 6 days of the cycle. This regimen is now incorporated into the Society for Integrative Oncology and ASCO integrative oncology guidelines as an evidence-supported adjunct to standard CINV prophylaxis.
Motion Sickness — The Original Mowrey 1982 Lancet Trial
The modern Western interest in ginger as an antiemetic traces directly to a single 1982 letter to The Lancet by Mowrey and Clayson titled "Motion sickness, ginger, and psychophysics." The authors enrolled 36 undergraduates highly susceptible to motion sickness and randomized them in a triple-arm trial:
- 940 mg powdered ginger in capsules
- 100 mg dimenhydrinate (Dramamine) in capsules
- Placebo (chickweed in capsules)
Twenty minutes after dosing, subjects were strapped into a tilted rotating chair (a standardized motion sickness provocation rig) and rotated for up to 6 minutes or until they signaled they were about to vomit. The ginger group lasted significantly longer than the placebo group (mean ~5.5 min vs ~3 min) and longer than the dimenhydrinate group. The contrast with dimenhydrinate was particularly striking because the conventional pharmacology of the time held that motion sickness was a primarily vestibular phenomenon — an H1 histamine receptor problem — for which a peripheral gut-acting agent should be useless.
The Mowrey trial has been criticized methodologically (small sample, single trial, possible unblinding by the distinctive ginger taste), but it triggered a generation of follow-up studies that have generally confirmed ginger's utility for motion sickness, though with smaller effect sizes than Mowrey reported.
Practical clinical use: 250–500 mg ginger powder taken 30–60 minutes before anticipated motion exposure (boat travel, fishing trip, car ride for the susceptible child), repeated every 4 hours as needed. Crystallized ginger chewed during travel is a reasonable continuous-dosing form that doubles as a behavioral distraction. The principal advantage over dimenhydrinate, meclizine, or scopolamine is lack of sedation — useful for adults who need to function during travel or for children where conventional motion-sickness drugs cause paradoxical agitation.
Vestibular vs. Chemoreceptor Nausea — Where Ginger Works Best
An important pharmacologic clarification helps explain ginger's pattern of benefit: nausea has at least four mechanistically distinct triggers, each acting through different receptor pathways and responding to different drug classes:
- Vestibular nausea (motion sickness, vertigo, vestibular migraine) — driven primarily by acetylcholine and histamine at H1 receptors in the vestibular nuclei. First-line drugs: meclizine, dimenhydrinate, scopolamine. Ginger's evidence here is real but modest.
- Chemoreceptor trigger zone (CTZ) nausea (chemotherapy, opioids, uremia, electrolyte derangement) — driven by dopamine D2, 5-HT3, and NK1 receptors in the area postrema. First-line drugs: 5-HT3 antagonists, NK1 antagonists, dopamine antagonists. Ginger's evidence here (the CINV literature) is strong, working through its 5-HT3 antagonism.
- Vagal afferent nausea (gastric distension, mucosal irritation, food poisoning, gastroparesis) — driven by 5-HT3 receptors on vagal terminals in the gut. First-line drugs: 5-HT3 antagonists, prokinetics. Ginger's evidence here is strong, working through both 5-HT3 antagonism and the prokinetic effect discussed in Digestive Aid & Gastroparesis.
- Cortical/anticipatory nausea (anxiety-driven, conditioned-response after prior chemotherapy) — driven by higher cortical pathways and limbic input. First-line approach: benzodiazepines (lorazepam), behavioral therapy. Ginger has minimal evidence here.
The pattern explains why ginger's strongest evidence is in pregnancy nausea (largely vagal + CTZ), chemotherapy nausea (CTZ), and postoperative nausea (mixed CTZ + vagal from gas insufflation), with smaller and less consistent effect in vestibular and anticipatory nausea. When a clinician is considering ginger for a particular patient, the question to ask is "what receptor pathway is driving the nausea?" — ginger has its largest effect where 5-HT3 antagonism would help.
Practical Dosing — Forms, Timing, Routes
Ginger comes in radically different pharmaceutical forms with very different bioavailability and effect profiles. The recommendations below reflect what the clinical-trial literature actually used.
- Powdered ginger capsules (the trial standard) — 250 mg per capsule is the most common commercial format and matches the Vutyavanich pregnancy dose. Aim for 1–1.5 g total daily, divided BID/TID/QID. Look for products standardized to gingerol/shogaol content (typically 5–10% gingerols by HPLC). Take with food to avoid the empty-stomach "ginger burn."
- Fresh ginger root — roughly 1 tsp of grated fresh ginger root contains approximately 250 mg of ginger by dry weight (though gingerol content varies with root age and storage). Add to tea, smoothies, or cooking. Pharmacologically dominated by 6-gingerol (the fresh-form compound), which has slightly different effects than dried-ginger 6-shogaol.
- Crystallized / candied ginger — variable ginger content but typically 100–500 mg per piece. The chewing action and gradual buccal absorption may provide additional benefit for motion sickness and the early-morning component of pregnancy nausea. Watch for sugar content if managing blood glucose.
- Ginger tea (steeped from fresh root or tea bags) — convenient for mild nausea and the rehydration matters as much as the ginger content. Steep 2–3 thin slices of fresh root in 8 oz hot water for 10 minutes, or use a commercial ginger tea bag.
- Ginger ale and ginger beer — most commercial brands contain essentially no real ginger (only ginger flavoring extract); the carbonation and sugar may modestly settle an upset stomach but the pharmacologic effect is minimal. Specialty "real ginger" brands (read the label for grams of ginger or look for sediment in the bottle) are an exception.
- Ginger essential oil (aromatherapy) — a few drops on a cotton ball held near the nose. Used in some postoperative settings; small trials suggest modest benefit. Not a substitute for the oral capsule dose.
- Ginger lozenges and gum — useful when oral capsules cannot be tolerated (severe nausea, hyperemesis). The buccal absorption bypasses gastric processing.
Timing for specific indications:
- Pregnancy nausea: 250 mg QID, starting first thing in the morning before getting out of bed (the empty-stomach early-morning peak is the worst window)
- Chemotherapy nausea: 0.5–1 g daily, starting 3 days before infusion, continuing through day 6 of the cycle
- Postoperative nausea: 1 g approximately 1 hour preoperatively (if surgical fasting protocol allows)
- Motion sickness: 250–500 mg 30–60 minutes before motion exposure, repeat every 4 hours as needed
- Acute nausea (food poisoning, viral gastroenteritis, hangover): 250–500 mg every 2–4 hours as needed; if vomiting prevents capsule tolerance, switch to ginger lozenges or sips of ginger tea
Cautions and Contraindications
- Pregnancy — despite extensive favorable evidence, occasional concerns are raised about high-dose ginger and pregnancy. The consensus of obstetric organizations is that ginger up to 1.5 g daily is safe in pregnancy; there is no documented increase in spontaneous abortion, preterm birth, or congenital malformation rates. Some old concerns about ginger as an emmenagogue (period-inducer) at high doses are based on traditional-use folklore, not clinical evidence. The American College of Obstetricians and Gynecologists includes ginger in its first-line recommendations for NVP.
- Bleeding risk and surgery — ginger has antiplatelet activity through inhibition of thromboxane synthesis (the same pathway as aspirin). Most surgical pre-op protocols recommend stopping ginger supplements 1–2 weeks before surgery, particularly for procedures with significant bleeding risk (cardiac, neurosurgery, major vascular). Culinary use of ginger does not need to be stopped.
- Warfarin and other anticoagulants — case reports describe INR elevation when ginger is added to warfarin therapy. The mechanism is uncertain (additive antiplatelet effect plus possible CYP2C9 interaction). Patients on warfarin who want to take therapeutic doses of ginger (more than culinary use) should have INR checked more frequently during dose initiation. For patients on direct oral anticoagulants (apixaban, rivaroxaban, dabigatran), the data are sparser but caution is reasonable.
- Diabetes / hypoglycemia — ginger may modestly reduce blood glucose and HbA1c (see the cross-cutting Research Papers in the Benefits hub). Diabetic patients adding therapeutic-dose ginger to insulin or sulfonylurea therapy should monitor glucose more closely during dose initiation, particularly for the first 2–4 weeks.
- Gallstones — ginger stimulates bile flow. Patients with known cholelithiasis may experience biliary colic with high-dose ginger; consult a clinician before therapeutic use.
- GERD — mixed effects — ginger's prokinetic action can help GERD (faster gastric emptying reduces the volume available to reflux), but the pungent gingerols can also irritate already-inflamed esophageal mucosa in some patients. Start at lower doses (125–250 mg) and titrate.
- Children — ginger is generally safe for children over 2 years at proportionally reduced doses (50–100 mg per dose for ages 2–6; 100–250 mg for ages 6–12). Crystallized ginger or ginger tea may be more palatable than capsules.
Key Research Papers
- Vutyavanich T, Kraisarin T, Ruangsri R (2001). Ginger for nausea and vomiting in pregnancy: randomized, double-masked, placebo-controlled trial. Obstetrics & Gynecology 97(4):577–582. — PubMed: Vutyavanich 2001
- Chaiyakunapruk N, Kitikannakorn N, Nathisuwan S et al. (2006). The efficacy of ginger for the prevention of postoperative nausea and vomiting: a meta-analysis. American Journal of Obstetrics & Gynecology 194(1):95–99. — PubMed: Chaiyakunapruk 2006
- Marx W, Kiss N, Isenring L (2015). Is ginger beneficial for nausea and vomiting? An update of the literature. Current Opinion in Supportive & Palliative Care 9(2):189–195. — PubMed: Marx 2015 update
- Marx WM, Teleni L, McCarthy AL et al. (2013). Ginger (Zingiber officinale) and chemotherapy-induced nausea and vomiting: a systematic literature review. Nutrition Reviews 71(4):245–254. — PubMed: Marx 2013 CINV review
- Ryan JL, Heckler CE, Roscoe JA et al. (2012). Ginger (Zingiber officinale) reduces acute chemotherapy-induced nausea: a URCC CCOP study of 576 patients. Supportive Care in Cancer 20(7):1479–1489. — PubMed: Ryan 2012
- Mowrey DB, Clayson DE (1982). Motion sickness, ginger, and psychophysics. The Lancet 1(8273):655–657. — PubMed: Mowrey 1982
- Lien HC, Sun WM, Chen YH et al. (2003). Effects of ginger on motion sickness and gastric slow-wave dysrhythmias induced by circular vection. American Journal of Physiology — Gastrointestinal & Liver Physiology 284(3):G481–G489. — PubMed: Lien 2003
- Pillai AK, Sharma KK, Gupta YK, Bakhshi S (2011). Anti-emetic effect of ginger powder versus placebo as an add-on therapy in children and young adults receiving high emetogenic chemotherapy. Pediatric Blood & Cancer 56(2):234–238. — PubMed: Pillai 2011
- Sripramote M, Lekhyananda N (2003). A randomized comparison of ginger and vitamin B6 in the treatment of nausea and vomiting of pregnancy. Journal of the Medical Association of Thailand 86(9):846–853. — PubMed: Sripramote ginger vs B6
- Borrelli F, Capasso R, Aviello G, Pittler MH, Izzo AA (2005). Effectiveness and safety of ginger in the treatment of pregnancy-induced nausea and vomiting. Obstetrics & Gynecology 105(4):849–856. — PubMed: Borrelli 2005
- Toth B, Lantos T, Hegyi P et al. (2018). Ginger (Zingiber officinale): An alternative for the prevention of postoperative nausea and vomiting. A meta-analysis. Phytomedicine 50:8–18. — PubMed: Toth 2018
- Lete I, Allué J (2016). The Effectiveness of Ginger in the Prevention of Nausea and Vomiting during Pregnancy and Chemotherapy. Integrative Medicine Insights 11:11–17. — PubMed: Lete 2016
- Abdel-Aziz H, Windeck T, Ploch M, Verspohl EJ (2006). Mode of action of gingerols and shogaols on 5-HT3 receptors: binding studies, cation uptake by the receptor channel and contraction of isolated guinea-pig ileum. European Journal of Pharmacology 530(1–2):136–143. — PubMed: Abdel-Aziz mechanism
PubMed Topic Searches
- PubMed: Ginger and pregnancy nausea
- PubMed: Ginger and CINV
- PubMed: Ginger and PONV
- PubMed: Ginger and motion sickness
- PubMed: Ginger 5-HT3 mechanism
- PubMed: Ginger and hyperemesis gravidarum
Connections
- Ginger Overview
- Ginger Benefits Hub
- Ginger Anti-Inflammatory & OA
- Ginger Digestive & Gastroparesis
- Ginger for Migraine & Pain
- Nausea and Vomiting
- Cancer (Chemotherapy Context)
- GERD
- Irritable Bowel Syndrome
- Migraine (Migraine-Associated Nausea)
- Turmeric (Sister Rhizome)
- Cinnamon
- Vitamin B6 (Co-Therapy for Pregnancy Nausea)
- Gut Healing
- All Herbs