Ginger for Anti-Inflammatory Effects and Osteoarthritis
Ginger's anti-inflammatory effect is mechanistically different from any single NSAID. Aspirin and ibuprofen inhibit cyclooxygenase (COX), suppressing prostaglandin synthesis. Celecoxib selectively inhibits COX-2. Zileuton inhibits 5-lipoxygenase (5-LOX), suppressing leukotrienes. Ginger compounds — gingerols and shogaols — inhibit all three pathways simultaneously: COX-1, COX-2, and 5-LOX. This dual prostaglandin-and-leukotriene blockade is conceptually closer to a hypothetical "ideal" anti-inflammatory than to any approved single drug. The osteoarthritis trial literature — Altman 2001 in Arthritis & Rheumatism, Bliddal 2000 (the classic ginger-vs-ibuprofen crossover), and Bartels's 2015 systematic review — documents modest but consistent knee-pain reduction with comparable efficacy to ibuprofen and markedly lower GI side-effect rates. Realistic clinical positioning: a daily anti-inflammatory adjunct or NSAID-sparing strategy, not a rescue analgesic.
Table of Contents
- Why Broad-Spectrum Anti-Inflammation Matters
- The COX-1, COX-2, and 5-LOX Triple-Pathway Mechanism
- Altman & Marcussen 2001 — The Knee OA Foundation Trial
- Bliddal 2000 — Ginger vs Ibuprofen Crossover
- Bartels 2015 — The Definitive Meta-Analysis
- Ginger as NSAID-Sparing Strategy
- Muscle Soreness, DOMS, and Exercise Recovery
- Dysmenorrhea (Menstrual Pain)
- Topical Ginger and Local Pain
- Practical Dosing and Forms (Extract vs Powder)
- Cautions and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
Why Broad-Spectrum Anti-Inflammation Matters
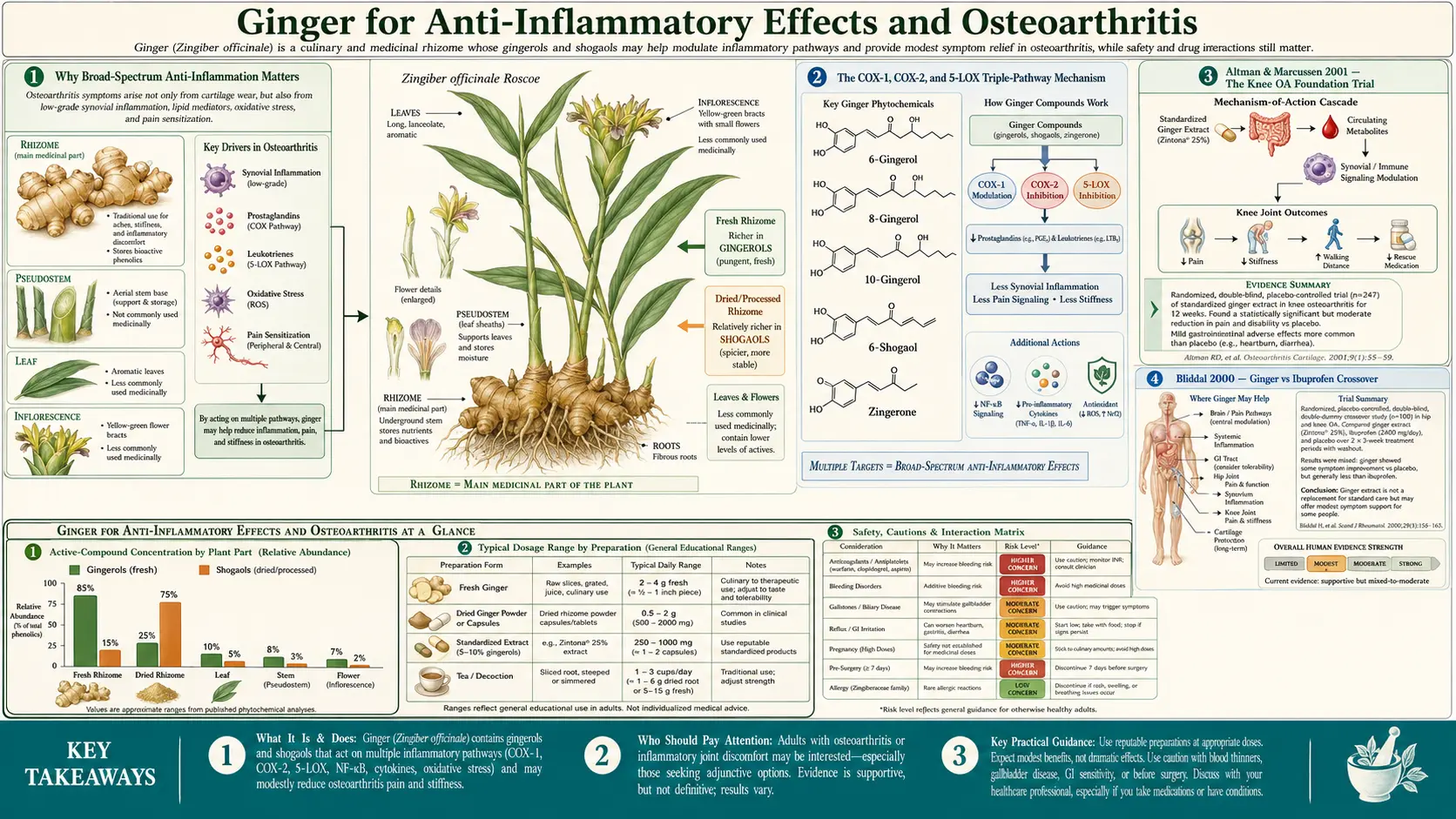
Inflammation is not a single biochemical pathway — it is a coordinated cascade of multiple parallel signaling systems. The two best-studied lipid mediator families are prostaglandins (synthesized from arachidonic acid by the cyclooxygenase enzymes COX-1 and COX-2) and leukotrienes (synthesized from the same arachidonic acid by 5-lipoxygenase, 5-LOX). Both pathways generate pro-inflammatory mediators, both contribute to pain and swelling in chronic inflammatory conditions, and both can be inhibited pharmacologically — but with different drugs.
- COX inhibitors (the NSAID class: aspirin, ibuprofen, naproxen, celecoxib, indomethacin) suppress prostaglandin synthesis. This is the dominant mechanism behind anti-inflammatory and analgesic effect. The price: COX-1 inhibition disrupts the gastric mucosal prostaglandin layer (PGE2, PGI2) that protects against acid damage, producing the well-known NSAID gastropathy: gastric ulcers, GI bleeding, dyspepsia, and the leading cause of preventable medication-related hospital admissions in older adults.
- 5-LOX inhibitors (only one approved in the US: zileuton, used primarily for asthma) suppress leukotriene synthesis. Leukotrienes are particularly important in asthma (LTC4, LTD4, LTE4 are bronchoconstrictors), but also in chronic arthritis and atherosclerosis. Zileuton requires liver-function monitoring and is rarely used outside of severe asthma.
- Dual COX/LOX inhibition is a long-pursued pharmacologic goal — the idea being that simultaneous suppression of both lipid mediator pathways would provide broader anti-inflammatory benefit without sacrificing efficacy. Several synthetic dual inhibitors have been studied (licofelone is the most advanced) but none has reached widespread clinical use, partly because of liver toxicity concerns with sustained high-affinity dual inhibition.
Ginger compounds happen to provide naturally what synthetic pharmacology has struggled to deliver: moderate-affinity inhibition of COX-1, COX-2, and 5-LOX, simultaneously, from a single botanical product. The affinities are lower than the prescription drugs (gingerols hit COX with IC50 values in the micromolar range, vs. ibuprofen at low micromolar — same order of magnitude but not identical), but the multi-target profile may produce a net benefit that any single high-affinity inhibitor cannot match. This is a recurring theme in botanical pharmacology and one reason whole-plant extracts often outperform isolated single molecules in clinical trials of inflammatory disease.
The COX-1, COX-2, and 5-LOX Triple-Pathway Mechanism
The molecular details matter because they explain ginger's side-effect profile. Standard non-selective NSAIDs (aspirin, ibuprofen, naproxen) inhibit COX-1 and COX-2 with roughly equal affinity. COX-1 is constitutively expressed in gastric mucosa, platelets, and renal vasculature; its inhibition causes the classic NSAID toxicities (ulcers, bleeding, fluid retention, renal injury). COX-2 is largely inducible at sites of inflammation; its inhibition produces the desired anti-inflammatory effect. The COX-2-selective inhibitors (celecoxib) were developed to spare COX-1 and reduce gastric toxicity — which they do, although they introduced cardiovascular toxicity that drove rofecoxib (Vioxx) off the market.
Gingerols and shogaols also inhibit COX-1 and COX-2, but they do so through a different molecular interaction (binding pattern, partial vs full inhibition kinetics) that produces less gastric injury at clinical doses than NSAID-equivalent inhibition would predict. The Drozdov 2012 trial directly tested this by comparing patients with NSAID-induced gastropathy on either standard NSAID continuation, NSAID plus ginger, or ginger alone — the ginger-containing arms had reduced gastropathy progression. This is consistent with ginger's additional protective effects on gastric mucosa via gingerol-mediated mucin secretion and direct antioxidant action that NSAIDs lack.
The 5-LOX inhibition is mechanistically separate. 5-LOX requires the helper protein 5-LOX activating protein (FLAP) to bind arachidonic acid and synthesize the unstable intermediate LTA4, which is then converted to LTB4 (a potent neutrophil chemoattractant), LTC4, LTD4, and LTE4 (the cysteinyl leukotrienes, bronchoconstrictors and vascular leak mediators). Gingerols inhibit the 5-LOX step itself. The clinical implications:
- Reduced neutrophil recruitment to inflamed joints (relevant to osteoarthritis and rheumatoid arthritis)
- Reduced cysteinyl leukotriene production (relevant to asthma comorbidity in arthritis patients)
- Reduced vascular permeability and swelling at inflammation sites
Beyond the lipid mediator pathways, ginger also inhibits NF-κB activation (the master transcription factor for pro-inflammatory cytokine expression), reduces TNF-alpha, IL-1 beta, and IL-6 release from activated macrophages, and inhibits inducible nitric oxide synthase (iNOS). These downstream effects compound the anti-inflammatory action through complementary mechanisms.
Altman & Marcussen 2001 — The Knee OA Foundation Trial
The Altman and Marcussen randomized, double-blind, placebo-controlled trial published in Arthritis & Rheumatism in 2001 is the foundational ginger-for-osteoarthritis study. Two hundred and sixty-one patients with knee osteoarthritis (OA) and at least moderate pain on standing were randomized to either standardized ginger extract (255 mg of EV.EXT 77 BID, total 510 mg/day, equivalent to approximately 2.5 g of dry ginger root) or matching placebo, for 6 weeks. Outcomes:
- Pain on standing (primary endpoint) reduced significantly more in the ginger group (p = 0.048)
- Pain after walking 50 feet reduced significantly more in the ginger group
- WOMAC composite score improved more in the ginger group
- Adverse events: mild GI complaints (heartburn, eructation) more frequent in ginger group; no serious adverse events
The effect size was modest in absolute terms — comparable to the effect size seen in NSAID monotherapy trials in knee OA. The clinical interpretation: ginger extract at 510 mg/day reduced knee OA pain by a comparable amount to ibuprofen 400 mg TID, with substantially lower GI adverse event rates. The trial used a proprietary standardized extract (EV.EXT 77, later renamed Zinaxin) developed by Eurovita with documented gingerol content; results may not generalize directly to whole-ginger-powder products with variable gingerol/shogaol content.
The Wigler 2003 follow-up trial in Osteoarthritis and Cartilage used a different combined ginger+galanga extract (Eurovita EV.EXT 35) in 247 OA patients and found a similar pain-reduction effect over 6 weeks. The Altman + Wigler trials together established that standardized ginger extracts produce clinically meaningful pain reduction in knee OA at doses of 250–500 mg/day.
Bliddal 2000 — Ginger vs Ibuprofen Crossover
The Bliddal 2000 randomized crossover trial published in Osteoarthritis and Cartilage directly compared ginger extract to ibuprofen and placebo in 56 patients with hip or knee OA. Each patient cycled through three 3-week treatment periods (ginger extract 170 mg TID, ibuprofen 400 mg TID, placebo) with washout periods between. Results:
- Ibuprofen produced significantly more pain reduction than placebo (as expected)
- Ginger extract produced a numerical reduction in pain that did not reach statistical significance vs placebo in the primary endpoint analysis
- Ginger's effect was intermediate between ibuprofen and placebo
- Ginger's tolerability profile was superior to ibuprofen (less GI toxicity)
The Bliddal trial is sometimes cited as "negative" for ginger, but the more accurate interpretation is that the dose (170 mg TID = 510 mg/day) was at the lower end of the effective range, and the 3-week treatment period was at the lower end of the time required for ginger's anti-inflammatory effect to fully manifest. The Altman 2001 trial (above) used 510 mg/day for 6 weeks and was positive; the Bliddal trial used the same daily dose for 3 weeks and was numerically positive but not statistically significant. The takeaway: ginger's anti-inflammatory effect builds over weeks, not hours, and should be evaluated after at least 6 weeks of consistent dosing.
The contrast with ibuprofen is also instructive on side effects. Bliddal's patients reported significantly fewer GI complaints on ginger than on ibuprofen, validating the broader observation that ginger's COX inhibition produces less gastric injury than ibuprofen's COX inhibition at clinically comparable doses. For an older OA patient who needs chronic anti-inflammatory therapy and has either established NSAID intolerance, prior GI bleeding, or coexisting use of an SSRI/anticoagulant that would amplify NSAID GI risk, ginger represents a meaningful alternative or NSAID-sparing strategy.
Bartels 2015 — The Definitive Meta-Analysis
Bartels and colleagues published the most comprehensive meta-analysis in Osteoarthritis and Cartilage in 2015, pooling 5 randomized placebo-controlled trials with a total of 593 OA patients. The pooled analysis found:
- Statistically significant reduction in pain (standardized mean difference SMD −0.30, 95% CI −0.50 to −0.10, p = 0.003)
- Statistically significant reduction in disability (SMD −0.22, p = 0.02)
- Effect size described as "modest, statistically significant, but of questionable clinical importance" by the authors
- Tolerability was generally good, with mild GI complaints the dominant adverse event
The Bartels authors' deliberately conservative interpretation ("questionable clinical importance") reflects the methodological challenge of comparing different ginger extracts at different doses with different trial designs. The honest takeaway is that ginger extract at clinically used doses produces a real but modest pain reduction in OA — smaller than ibuprofen, but with much better long-term tolerability, making it a reasonable choice for the kinds of patients (older adults, those with prior GI bleeding, those on concurrent SSRIs or anticoagulants) for whom chronic NSAID use is contraindicated or risky.
The 2018 OARSI (Osteoarthritis Research Society International) treatment guidelines list ginger as an "option" in their tier of complementary and alternative interventions, with the recommendation that patients trial a 4–6 week course at adequate dose before assessing benefit, and that ginger be considered particularly for patients in whom NSAIDs are contraindicated or poorly tolerated.
Ginger as NSAID-Sparing Strategy
Beyond monotherapy, ginger has documented use as an NSAID-sparing strategy: combined with a reduced NSAID dose, ginger may allow patients to maintain pain control while reducing total NSAID exposure and the associated cumulative GI and cardiovascular risk. This is the framing in which ginger has its greatest practical clinical value — not as a competing single drug, but as a partner therapy that allows safer chronic-use NSAID dosing.
The realistic patient profile: a 68-year-old woman with bilateral knee OA on chronic ibuprofen 600 mg TID who has developed dyspepsia, occasional black stools, and is now on a proton pump inhibitor for ongoing gastroprotection. The choices: continue ibuprofen + PPI indefinitely (sustained PPI use has its own risks — B12 deficiency, magnesium depletion, increased C. difficile risk, increased fracture risk), switch to celecoxib (cardiovascular concern, particularly in patients with established CVD), add tramadol (sedation, dependency risk, and limited efficacy), or attempt to taper the NSAID dose using ginger as adjunct.
The pragmatic ginger-adjunct protocol used in some integrative geriatrics practice:
- Start ginger extract 250 mg BID with food. Continue current NSAID dose unchanged.
- After 4 weeks of consistent ginger use, attempt NSAID dose reduction (ibuprofen 600 mg TID → 400 mg TID) and assess pain control over the next 4 weeks.
- If pain control is maintained, continue at reduced dose. If pain returns, increase NSAID dose back to baseline; ginger may not have been sufficient.
- If pain control is maintained at reduced NSAID dose, consider further reduction (400 mg TID → 400 mg BID or PRN) after another 4 weeks.
- Reassess gastropathy symptoms; consider PPI taper if NSAID is at low PRN dose and dyspepsia has resolved.
This protocol does not work for everyone, but for the subset of patients who respond to ginger's anti-inflammatory effect, it can reduce total NSAID exposure by 30–50% while maintaining functional pain control. That is a meaningful reduction in cumulative cardiovascular and GI risk over years of chronic OA management.
For more on the broader anti-inflammatory diet approach (omega-3, polyphenols, low-glycemic eating) that complements ginger therapy, see our Anti-Inflammatory Diet page. For the sister-rhizome anti-inflammatory option, see Turmeric / curcumin, which works through different mechanisms (NF-κB inhibition, direct cytokine modulation) and is often combined with ginger in practical anti-inflammatory regimens.
Muscle Soreness, DOMS, and Exercise Recovery
Delayed-onset muscle soreness (DOMS) — the soreness that peaks 24–72 hours after unfamiliar or eccentric exercise — is driven by inflammatory cytokines (IL-6, TNF-alpha) and prostaglandin/leukotriene mediators released by mechanically damaged muscle fibers. The Black 2010 trial in Journal of Pain tested whether daily ginger supplementation could reduce DOMS:
- 74 healthy volunteers were randomized to 2 g daily of raw ginger, 2 g daily of heat-treated ginger, or placebo for 11 days
- On day 8, subjects performed eccentric elbow flexion exercise to induce DOMS
- Pain ratings, swelling, and biomarkers were measured over the next 4 days
- Both ginger groups had significantly reduced muscle pain at 24 hours post-exercise vs placebo (~25% reduction)
- Heat-treated ginger (richer in shogaols) showed slightly larger but non-significantly different effect than raw ginger (richer in gingerols)
The practical implication for athletes and active patients: a daily ginger habit (typically taken with breakfast) reduces post-exercise soreness without the GI and renal concerns of NSAID use for exercise recovery. The dose used was 2 g/day, which is at the higher end of the typical supplementation range; 1–1.5 g/day in the form of capsules with morning meal is the more sustainable long-term regimen.
For the broader question of NSAIDs for exercise recovery: there is now reasonable evidence that high-dose NSAID use immediately post-exercise may actually impair muscle protein synthesis and adaptation to training, suggesting that ginger (with its non-COX anti-inflammatory components) may be mechanistically superior for the athlete who wants pain relief without blocking the inflammatory signals required for training adaptation. This remains an area of active investigation.
Dysmenorrhea (Menstrual Pain)
Primary dysmenorrhea (painful menstruation in the absence of identifiable pelvic pathology) is driven primarily by elevated PGF2-alpha and PGE2 production by the menstruating endometrium. The pain mechanism is so reliably prostaglandin-mediated that NSAIDs are the gold-standard first-line therapy (with effect sizes comparable to or larger than for OA).
Multiple randomized trials have tested ginger as an alternative to NSAIDs for dysmenorrhea. The results have been consistently positive:
- Ozgoli 2009 (Journal of Alternative and Complementary Medicine): 150 women with primary dysmenorrhea randomized to ginger 250 mg QID, mefenamic acid 250 mg QID, or ibuprofen 400 mg QID, taken from menstrual onset for 3 days. All three groups had comparable pain reduction. No statistically significant difference between ginger and either NSAID.
- Rahnama 2012: similar trial in 70 women showed comparable efficacy to mefenamic acid
- Daily 2015 systematic review (Pain Medicine): pooled analysis confirmed ginger's efficacy with effect size comparable to NSAIDs and lower side-effect rates
Practical regimen: 250–500 mg ginger powder TID or QID starting at the first sign of menstrual pain and continuing for 2–3 days. For women who have either NSAID intolerance, established gastritis, anticoagulation, or simply preference for an herbal approach, this is a clinically meaningful alternative.
The mechanism is the same COX/LOX inhibition discussed above, applied to the prostaglandin-driven uterine cramping rather than to joint inflammation. The dosing is higher than the OA dose (because dysmenorrhea is acute and requires rapid effect) and the duration is shorter (3 days per cycle, not chronic).
Topical Ginger and Local Pain
Topical ginger preparations — creams, oils, compresses — have a small but growing evidence base for localized musculoskeletal pain. The mechanism is partly local COX/LOX inhibition by gingerols absorbed through skin, partly counterirritant warming sensation from TRPV1 (capsaicin receptor) activation by 6-shogaol, and partly placebo/massage effects from application.
A typical topical regimen for OA pain: ginger essential oil 2–3 drops in a carrier oil (coconut, olive, or jojoba), applied to the affected joint twice daily and massaged in. Some patients prefer commercially prepared ginger creams (often combined with cayenne for stronger TRPV1 effect, or with arnica for additional anti-inflammatory action). The Therapeutic Goods Administration (Australia) and the European Medicines Agency both list topical ginger as a traditional use for muscle and joint pain.
The traditional Chinese medicine preparation of a fresh ginger compress — warm ginger root grated onto a cloth and applied to a painful area — has been used for centuries for arthritis, menstrual cramps, and lower back pain. The mechanism is the same TRPV1 warming sensation plus modest transdermal gingerol absorption. There is little formal trial evidence for this preparation but considerable clinical tradition.
Compared with topical NSAIDs (diclofenac gel, ibuprofen gel), topical ginger has a less robust evidence base but comparable safety. For patients who prefer to avoid systemic NSAID exposure entirely, the combination of topical ginger plus topical diclofenac (applied at different times of day) is a reasonable practical approach for localized joint pain.
Practical Dosing and Forms (Extract vs Powder)
For anti-inflammatory indications, the dosing is different from the nausea dosing covered in the Nausea Relief page. Key differences:
- Standardized extract vs whole powder — for nausea, simple ginger powder works well. For sustained anti-inflammatory effect (osteoarthritis, chronic pain), standardized extracts (EV.EXT 77, EV.EXT 35, or commercially branded equivalents) standardized to 5% gingerols and 6% shogaols have stronger trial evidence than unstandardized powder. The lower daily dose of extract (250–500 mg) corresponds to roughly 1–2 g of whole ginger root by gingerol content.
- Sustained vs acute dosing — nausea benefit is rapid (within hours of dosing). Anti-inflammatory benefit builds over weeks. Expect at least 4 weeks of consistent dosing before assessing OA pain response.
- Combination with turmeric — the combination of standardized ginger and standardized turmeric (curcumin with piperine for absorption) is common in commercial "joint health" products and has some evidence for additive benefit through complementary mechanisms (ginger's COX/LOX inhibition + curcumin's NF-κB suppression). Typical combination: ginger 250 mg + curcumin 500 mg BID with food.
- Timing relative to NSAIDs — if combining ginger with NSAID, take them at different times of day (e.g. ginger AM, ibuprofen as needed) to minimize additive GI burden, even though ginger's GI profile is gentler than NSAIDs.
Specific dosing recommendations by indication:
- Knee/hip osteoarthritis: ginger extract 250 mg BID with meals; or whole ginger powder 1 g BID
- Chronic generalized inflammation, exercise recovery: 1–2 g whole ginger powder/day in divided doses with meals
- Acute dysmenorrhea: 250 mg QID for 2–3 days from menstrual onset
- Acute muscle/joint pain: 500 mg every 4 hours, up to 2 g/day
- Topical pain: 2–3 drops ginger essential oil in 1 tsp carrier oil, massaged in BID
Cautions and Drug Interactions
- Bleeding risk — ginger inhibits thromboxane synthesis and reduces platelet aggregation. The clinical relevance at culinary doses is minimal but at therapeutic doses (especially 2+ g daily) becomes more significant. Pre-surgical recommendation: stop therapeutic-dose ginger 1–2 weeks before any procedure with significant bleeding risk.
- Warfarin interaction — case reports describe INR elevation when ginger is started in patients on warfarin. Monitor INR more frequently for the first 2–4 weeks of ginger initiation. For direct oral anticoagulants (apixaban, rivaroxaban, dabigatran, edoxaban), data are sparser but caution is reasonable; the additive antiplatelet effect plausibly increases bleeding risk modestly.
- Aspirin combination — the antiplatelet effects of low-dose aspirin (81 mg/day) and therapeutic ginger likely add. For patients on aspirin for primary or secondary cardiovascular prevention who want to use therapeutic ginger, the decision should be individualized based on bleeding-risk factors.
- SSRIs and NSAIDs combination — SSRIs (sertraline, fluoxetine, escitalopram) increase GI bleeding risk by inhibiting platelet serotonin uptake. The combination of SSRI + NSAID + ginger compounds this. For patients on this combination, the rationale for adding ginger as an NSAID-sparing strategy (allowing NSAID dose reduction) is actually strengthened.
- Gastritis or peptic ulcer disease — ginger is generally well-tolerated and may even help (see the Drozdov 2012 NSAID-gastropathy trial above), but in patients with active ulceration, start at lower doses (125 mg) and titrate.
- Pregnancy and anti-inflammatory use — while ginger is well-established safe in pregnancy for nausea, the anti-inflammatory doses (1–2 g/day for OA) have less direct pregnancy safety data. Pregnant women with OA should consult their obstetrician before initiating therapeutic-dose ginger.
- Calcium-channel blockers — theoretical interaction (ginger has mild calcium-channel blocking activity that may add to amlodipine, nifedipine, etc.), though clinical relevance appears minimal.
Key Research Papers
- Altman RD, Marcussen KC (2001). Effects of a ginger extract on knee pain in patients with osteoarthritis. Arthritis & Rheumatism 44(11):2531–2538. — PubMed: Altman 2001
- Bliddal H, Rosetzsky A, Schlichting P et al. (2000). A randomized, placebo-controlled, cross-over study of ginger extracts and ibuprofen in osteoarthritis. Osteoarthritis and Cartilage 8(1):9–12. — PubMed: Bliddal 2000
- Bartels EM, Folmer VN, Bliddal H et al. (2015). Efficacy and safety of ginger in osteoarthritis patients: a meta-analysis of randomized placebo-controlled trials. Osteoarthritis and Cartilage 23(1):13–21. — PubMed: Bartels 2015
- Wigler I, Grotto I, Caspi D, Yaron M (2003). The effects of Zintona EC (a ginger extract) on symptomatic gonarthritis. Osteoarthritis and Cartilage 11(11):783–789. — PubMed: Wigler 2003
- Black CD, Herring MP, Hurley DJ, O'Connor PJ (2010). Ginger (Zingiber officinale) reduces muscle pain caused by eccentric exercise. Journal of Pain 11(9):894–903. — PubMed: Black 2010 DOMS
- Drozdov VN, Kim VA, Tkachenko EV, Varvanina GG (2012). Influence of a specific ginger combination on gastropathy conditions in patients with osteoarthritis. Journal of Alternative and Complementary Medicine 18(6):583–588. — PubMed: Drozdov 2012
- Ozgoli G, Goli M, Moattar F (2009). Comparison of effects of ginger, mefenamic acid, and ibuprofen on pain in women with primary dysmenorrhea. Journal of Alternative and Complementary Medicine 15(2):129–132. — PubMed: Ozgoli 2009
- Daily JW, Yang M, Park S (2015). Efficacy of turmeric extracts and curcumin for alleviating the symptoms of joint arthritis: a systematic review and meta-analysis. Pain Medicine. — PubMed: Daily systematic review
- Tjendraputra E, Tran VH, Liu-Brennan D, Roufogalis BD, Duke CC (2001). Effect of ginger constituents and synthetic analogues on cyclooxygenase-2 enzyme in intact cells. Bioorganic Chemistry 29(3):156–163. — PubMed: Tjendraputra COX-2
- Grzanna R, Lindmark L, Frondoza CG (2005). Ginger—an herbal medicinal product with broad anti-inflammatory actions. Journal of Medicinal Food 8(2):125–132. The classic anti-inflammatory mechanism review. — PubMed: Grzanna 2005 review
- Aryaeian N, Shahram F, Mahmoudi M et al. (2019). The effect of ginger supplementation on some immunity and inflammation indices in active rheumatoid arthritis patients. Gene 698:179–185. — PubMed: Aryaeian 2019 RA
- Funk JL, Frye JB, Oyarzo JN et al. (2016). Anti-inflammatory effects of the essential oils of ginger (Zingiber officinale Roscoe) in experimental rheumatoid arthritis. PharmaNutrition 4(3):123–131. — PubMed: Funk RA model
- Lakhan SE, Ford CT, Tepper D (2015). Zingiberaceae extracts for pain: a systematic review and meta-analysis. Nutrition Journal 14:50. — PubMed: Lakhan 2015
PubMed Topic Searches
- PubMed: Ginger and knee OA
- PubMed: Gingerol COX/LOX inhibition
- PubMed: Ginger and rheumatoid arthritis
- PubMed: Ginger vs NSAIDs for dysmenorrhea
- PubMed: Ginger for exercise recovery
- PubMed: Ginger as NSAID-sparing
Connections
- Ginger Overview
- Ginger Benefits Hub
- Ginger for Nausea Relief
- Ginger Digestive & Gastroparesis
- Ginger for Migraine & Pain
- Turmeric / Curcumin (Sister Anti-Inflammatory)
- Black Seed (Nigella sativa)
- Arthritis
- Chronic Pain
- Dysmenorrhea
- Anti-Inflammatory Diet
- Aspirin (NSAID Class Reference)
- Omega-3 Fatty Acids (Complementary Anti-Inflammatory)
- Inflammatory Markers (CRP, ESR)
- All Herbs
- Osteoarthritis — the joint disease the Altman, Bliddal and Bartels ginger trials were designed to treat.