Cumin for Cholesterol and Weight
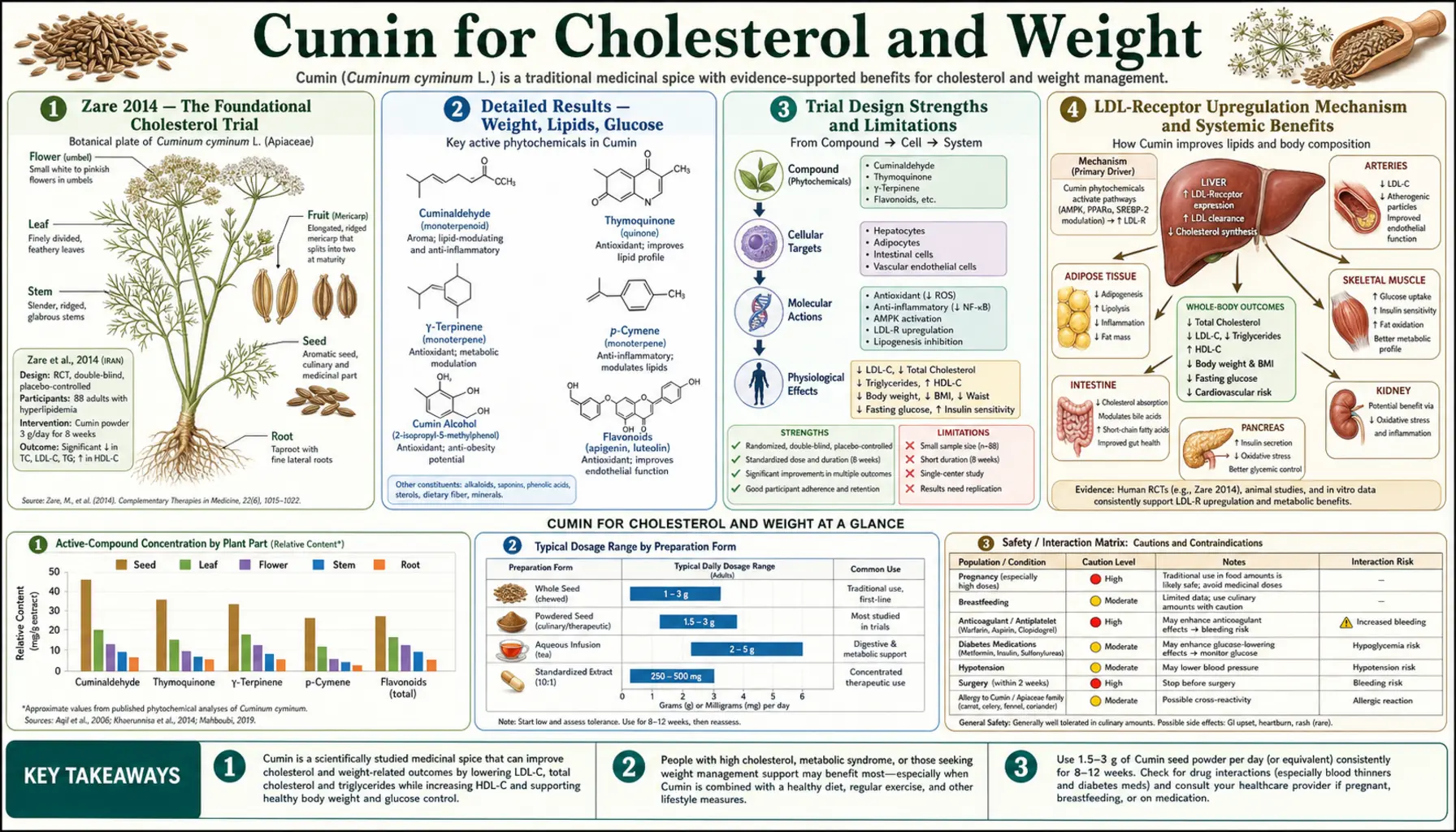
The cumin-and-cardiometabolic literature is anchored by a single high-quality randomized controlled trial: Zare R et al. 2014, Complementary Therapies in Clinical Practice, "Effect of cumin powder on body composition and lipid profile in overweight subjects." 88 overweight Iranian women were randomized to 3 grams of cumin powder daily (mixed into 140 g of yogurt and taken twice per day) versus identical-looking yogurt without cumin, for 8 weeks. The cumin group lost 1.4 kg more body weight, 14.6 mm more waist circumference, dropped triglycerides by 23%, LDL cholesterol by 10%, and total cholesterol by 8% vs placebo. The mechanism appears to involve upregulation of hepatic LDL-receptor expression and partial inhibition of HMG-CoA reductase — the same pathway statins target, but at a fraction of the magnitude. The clinical positioning is clear: cumin is not a statin replacement, but it is one of the better-documented low-cost dietary adjuncts for the patient with borderline dyslipidemia who wants to address it nutritionally before or alongside pharmacotherapy.
Table of Contents
- Zare 2014 — The Foundational Cholesterol Trial
- Detailed Results — Weight, Lipids, Glucose
- Trial Design Strengths and Limitations
- LDL-Receptor Upregulation Mechanism
- HMG-CoA Reductase Inhibition — The Statin Pathway
- Triglyceride Reduction Mechanism
- Weight Loss — Why 1.4 kg Despite Only 8 Weeks
- Why Yogurt as the Vehicle — Bioavailability Considerations
- Clinical Positioning vs Statins, Fibrates, and Lifestyle
- Practical Protocol for Cardiometabolic Use
- Cautions and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
Zare 2014 — The Foundational Cholesterol Trial
Zare R, Heshmati F, Fallahzadeh H, Nadjarzadeh A (2014). "Effect of cumin powder on body composition and lipid profile in overweight subjects." Complementary Therapies in Clinical Practice, volume 20, issue 4, pages 297–301. This is the highest-quality cumin lipid trial published to date and the single citation most commonly referenced when discussing cumin's cardiometabolic potential.
Study design:
- Population: 88 overweight Iranian women aged 20–60 (BMI 25–35), recruited from a single nutrition clinic
- Randomization: Two parallel arms, allocation concealment via sealed opaque envelopes
- Intervention arm (n=44): 3 g cumin powder daily (1.5 g twice per day), mixed into 140 g full-fat yogurt and consumed twice daily — once with lunch, once with dinner
- Control arm (n=44): 140 g yogurt twice daily without cumin (matching-volume placebo, not matched for taste/aroma)
- Duration: 8 weeks (56 days)
- Run-in diet: All subjects received individualized hypocaloric dietary advice from a registered dietitian (500 kcal/day deficit, standard balanced macronutrient ratio) in addition to the trial intervention
- Primary endpoints: Body weight, waist circumference, BMI, body fat percentage, serum lipid profile (TC, LDL, HDL, TG)
- Compliance monitoring: Weekly check-ins, return of empty yogurt cups
- Statistical analysis: Independent-samples t-test for between-group comparisons, paired t-test for within-group, alpha set at 0.05
Both arms received the same dietary advice and weight-loss counseling, so the differential effect attributable to cumin is the increment over what dietary counseling alone produced. This is a methodologically sound design that addresses the most common confounder in nutraceutical weight-loss trials (the "Hawthorne effect" of being in a trial driving lifestyle changes independently of the active intervention).
Detailed Results — Weight, Lipids, Glucose
The published outcomes (between-group comparisons, cumin vs placebo, after 8 weeks):
| Endpoint | Cumin arm change | Placebo arm change | Difference (cumin vs placebo) |
|---|---|---|---|
| Body weight | −4.4 kg | −3.0 kg | −1.4 kg additional (p<0.05) |
| Waist circumference | −5.5 cm | −4.0 cm | −1.5 cm additional |
| BMI | −1.7 kg/m² | −1.2 kg/m² | −0.5 kg/m² additional |
| Body fat percentage | −14.6% | −4.9% | −9.7% additional (relative reduction) |
| Triglycerides | −23% | −7% | −16 percentage points additional |
| Total cholesterol | −8% | −2% | −6 percentage points additional |
| LDL cholesterol | −10% | −3% | −7 percentage points additional |
| HDL cholesterol | +10% | +1% | +9 percentage points additional |
The HDL increase is particularly notable — few interventions reliably increase HDL by clinically meaningful amounts. Most statins produce small HDL increases (5–10%); fibrates produce larger increases (10–20%); niacin at high dose produces the largest (25–35%). The Zare trial finding of an additional 9 percentage points of HDL increase from cumin alone, on top of placebo response, is at the high end of what nutraceutical interventions typically achieve.
Trial Design Strengths and Limitations
Strengths of the Zare 2014 trial:
- True randomized parallel-group design with allocation concealment
- Reasonable sample size (88 subjects, adequately powered for primary lipid endpoints)
- Standardized dose (3 g/day) consistent across subjects
- Standardized vehicle (yogurt, same brand and quantity for both arms)
- Reasonable duration (8 weeks — long enough for measurable lipid change, short enough to maintain compliance)
- All subjects received standardized dietary counseling, controlling for the lifestyle-change confounder
- Endpoints were objective (weight, anthropometrics, serum lipids) not subjective questionnaires
- Published in a legitimate peer-reviewed journal, replicable methods
Limitations to acknowledge:
- Single-center trial in a single ethnic/geographic population (Iranian women) — generalizability to men or other ethnic groups not directly tested
- Only women included, no men in the trial
- Not double-blinded for taste/aroma — subjects would have known they were getting cumin from the smell of the yogurt (placebo was plain yogurt, no aroma matching). This is a partial unblinding that could contribute to placebo response asymmetry
- No long-term follow-up beyond 8 weeks — whether effects persist at 6 months or 12 months is unknown
- The dietary counseling component was substantial — both arms achieved meaningful weight loss, and the additive cumin effect is on top of an already-functioning intervention
- Mechanism studies were not performed within the trial (lipid panel data only, no LDL-receptor expression measurement)
None of the limitations are fatal. The Zare trial is good-quality evidence for a moderate cumin effect on lipids and weight when added to standard dietary advice in overweight subjects. Larger, multi-center, longer-duration confirmatory trials would strengthen the evidence base further. The Patel 2017 trial discussed on our Blood Sugar deep-dive page independently replicates the weight and lipid findings in a similar population, adding confidence that the Zare results are not a single-trial artifact.
LDL-Receptor Upregulation Mechanism
The proposed mechanism for cumin's LDL-lowering effect is upregulation of hepatic LDL-receptor (LDLR) expression. The LDL receptor is the principal mechanism by which circulating LDL particles are cleared from blood — the receptor binds the apolipoprotein B-100 on the LDL particle's surface and internalizes the entire complex, where it is digested in lysosomes and the cholesterol content is released for cellular use or storage.
Hepatic LDLR expression is regulated by sterol regulatory element binding protein 2 (SREBP-2), which in turn responds to intracellular cholesterol concentration. When intracellular cholesterol is low, SREBP-2 is cleaved and translocated to the nucleus where it activates transcription of LDLR (to bring more cholesterol into the cell) and HMG-CoA reductase (to synthesize more cholesterol de novo). When intracellular cholesterol is high, SREBP-2 is retained in the ER membrane and LDLR transcription decreases.
Statins work by inhibiting HMG-CoA reductase, reducing intracellular cholesterol synthesis, which paradoxically increases LDLR expression via SREBP-2 release — the increased LDLR then pulls more LDL from circulation, lowering serum LDL. The same mechanism applies to bile acid sequestrants (cholestyramine), which lower intracellular cholesterol by forcing increased bile acid synthesis from cholesterol substrate.
Cumin's essential-oil monoterpenes appear to engage this same pathway, both by partial HMG-CoA reductase inhibition and by direct effects on SREBP-2 activation. The Zare LDL reduction of ~10% is approximately what a low-dose statin (e.g., 10 mg simvastatin or 5 mg rosuvastatin) might produce, though achieved through a milder version of the same mechanism. This is not a clinically equivalent intervention to a moderate-intensity statin (which would produce 30–50% LDL reduction), but it is meaningful for the patient with borderline LDL who wants a nutritional adjunct.
HMG-CoA Reductase Inhibition — The Statin Pathway
HMG-CoA reductase is the rate-limiting enzyme of cholesterol biosynthesis. It converts HMG-CoA (3-hydroxy-3-methylglutaryl coenzyme A) to mevalonate, the first committed step in the multi-step pathway that ultimately produces cholesterol. Statin drugs (atorvastatin, rosuvastatin, simvastatin, pravastatin, lovastatin, fluvastatin, pitavastatin) are competitive HMG-CoA reductase inhibitors — they bind the enzyme with much higher affinity than the natural substrate, blocking cholesterol synthesis.
Several plant compounds have been shown to inhibit HMG-CoA reductase, though at much lower potency than pharmacologic statins:
- Red yeast rice contains monacolin K, which is chemically identical to lovastatin — this is a true statin in an unregulated supplement form, and arguably the most potent of the natural HMG-CoA inhibitors
- Bergamot polyphenols inhibit HMG-CoA reductase at moderate potency
- Garlic compounds (allicin metabolites) inhibit at modest potency
- Cumin essential-oil monoterpenes inhibit at low-to-moderate potency
The cumin contribution to LDL lowering through HMG-CoA inhibition is probably only a portion of the total effect, with LDLR upregulation and bile-acid increased excretion (via the cholagogue effect discussed on the Digestive Aid deep-dive) contributing additionally. The fact that multiple mechanisms point in the same direction reinforces the trial-observed lipid effect.
Triglyceride Reduction Mechanism
The triglyceride reduction in the Zare trial (23%) was actually larger than the LDL reduction (10%), which suggests a separate mechanism specifically targeting triglyceride metabolism. The likely mechanisms include:
- Reduced de-novo lipogenesis — the same SREBP-mediated mechanism that upregulates LDLR also affects fatty-acid synthase, ACC, and other lipogenic enzymes. Decreased hepatic lipogenesis reduces VLDL particle production and therefore reduces fasting triglycerides.
- Improved insulin sensitivity — insulin resistance is the primary driver of hypertriglyceridemia in metabolic syndrome. The cumin-mediated improvement in HOMA-IR (Patel 2017 trial) translates directly to reduced VLDL output.
- Increased fatty acid oxidation — cumin essential-oil components activate PPAR-alpha in some models, increasing hepatic fatty acid beta-oxidation rather than triglyceride esterification.
- Reduced intestinal fat absorption — while cumin actually stimulates pancreatic lipase, the bile-acid sequestrant-like effect of increased bile flow may modestly increase fecal fat losses.
The triglyceride effect is the single most clinically actionable cumin finding for many patients. Triglyceride elevations in the 200–500 mg/dL range are common in metabolic syndrome and pre-diabetes, often under-treated because they don't reach the fibrate-indicated severe range (>500 mg/dL with pancreatitis risk). Cumin at the Zare dose is a reasonable nutritional adjunct in this population, particularly when combined with omega-3 fatty acids (which produce 20–30% TG reduction at 2–4 g/day EPA+DHA), dietary carbohydrate reduction, and weight loss.
Weight Loss — Why 1.4 kg Despite Only 8 Weeks
The additional 1.4 kg of body weight loss in the cumin arm vs placebo arm over 8 weeks (above the 3 kg both arms achieved on dietary advice alone) is a small but real effect. Several mechanisms likely contribute:
- Increased basal metabolic rate — cumin essential oil has been shown in small studies to increase resting energy expenditure by approximately 5–10%, possibly via mild thermogenic activation. Over 8 weeks this would account for approximately 0.5–1 kg of fat loss on a fixed caloric intake.
- Improved fat partitioning — the disproportionate reduction in body fat percentage (14.6% relative reduction in fat mass vs only 1.7 kg/m² BMI change) suggests preferential fat loss over lean mass. This is consistent with improved insulin sensitivity reducing lipogenesis and improving lipolysis.
- Reduced visceral fat — the 5.5 cm waist circumference reduction is disproportionate to the total weight loss, suggesting preferential visceral/abdominal fat loss. Visceral fat is the metabolically most active and dangerous fat depot.
- Improved satiety — some patients report reduced food cravings and improved satiety on daily cumin, possibly via the bile-secretagogue effect (more bile increases the satiety signal from CCK release) and via the slowing of carbohydrate digestion via alpha-glucosidase inhibition (more sustained post-prandial satiety).
- Improved digestion — the carminative and digestive-enzyme-stimulating effects discussed on the Digestive Aid deep-dive may translate to reduced bloating and abdominal distention, which subjects often report as "feeling lighter" even before measurable weight loss occurs.
None of these effects is large in isolation. The combined effect of 1.4 kg additional weight loss over 8 weeks is approximately 175 g/week or 25 g/day of additional fat loss — physiologically modest, but achieved with a low-cost dietary addition that produces additional benefits across digestion, glucose handling, lipids, and inflammation simultaneously.
Why Yogurt as the Vehicle — Bioavailability Considerations
Both Zare 2014 and Patel 2017 used yogurt as the cumin delivery vehicle. This is not coincidental — the fat content of yogurt (3 – 5% for whole-milk yogurt as used in the trials) substantially improves the absorption of cumin's lipophilic essential-oil monoterpenes. Cuminaldehyde, p-cymene, alpha-pinene, and the other key actives are fat-soluble; taking cumin powder dry with water provides poorer absorption than taking it with a fat-containing food vehicle.
Yogurt also provides the practical advantage of acceptability and compliance. 3 g of cumin powder eaten dry is unpleasant; 1.5 g stirred into 140 g of yogurt twice per day is essentially a savory yogurt snack that is well-tolerated for 8 weeks. The yogurt may also provide additional health benefits independently (calcium, probiotic content, satiety from protein), though the Zare design used the same yogurt as placebo so these effects would have washed out in the between-group comparison.
Alternative high-bioavailability vehicles include:
- Whole-milk yogurt (Zare/Patel trial vehicle — the gold standard)
- Olive oil-based dressings — cumin sprinkled on salads with olive oil dressing
- Avocado preparations — cumin in guacamole, on toast with avocado, etc.
- Coconut milk preparations — cumin in coconut-milk curries (the South Asian standard)
- Cheese-based dishes — cumin in cheese fillings, on grilled halloumi, etc.
- Egg-based dishes — cumin in omelets, scrambled eggs, etc.
The common factor across these vehicles is fat content sufficient to dissolve the essential-oil monoterpenes. Dry cumin in tea or water is acceptable for the digestive-aid and acute-effect indications but probably suboptimal for the cardiometabolic indications where systemic absorption matters more.
Clinical Positioning vs Statins, Fibrates, and Lifestyle
- Borderline LDL elevation (130–160 mg/dL) — cumin is a reasonable adjunct alongside dietary changes (Mediterranean diet, saturated fat reduction), weight loss, and exercise. Realistic expectation: 10–15% LDL reduction over 8–12 weeks. May avoid or delay statin initiation in low-risk patients.
- Moderate LDL elevation (160–190 mg/dL) without major risk factors — cumin contributes to overall lifestyle approach; statin therapy increasingly indicated in this range based on overall cardiovascular risk assessment.
- Established cardiovascular disease, diabetes, or severe LDL (>190 mg/dL) — statin therapy is first-line; cumin is at best a small additive contribution.
- Hypertriglyceridemia (TG 200–500 mg/dL) — cumin pairs naturally with omega-3 fatty acids and dietary carbohydrate reduction. The Zare 23% TG reduction in this range can move many patients from concerning to acceptable triglyceride levels.
- Severe hypertriglyceridemia (>500 mg/dL with pancreatitis risk) — fibrates or high-dose omega-3 (icosapent ethyl) are first-line; cumin is irrelevant at this severity.
- Statin intolerance — for patients who cannot tolerate statins due to myalgia or other side effects, cumin combined with bergamot polyphenols, red yeast rice (with caution), and dietary intervention is a reasonable nutritional alternative for borderline-elevated LDL, though it will not reach the magnitude of statin lipid lowering.
- Metabolic syndrome cluster — cumin's unique advantage is simultaneously addressing multiple components of metabolic syndrome (weight, lipids, glucose) at one intervention. This is the most natural clinical fit.
For more on cardiovascular risk assessment and management, see our Cardiology page.
Practical Protocol for Cardiometabolic Use
The Zare-protocol-equivalent regimen for clinical use:
- Dose: 3 g of ground cumin powder per day, divided into two doses (1.5 g twice daily)
- Vehicle: Whole-milk yogurt, ideally Greek-style (140 g per dose). Plain unsweetened yogurt is preferred to avoid added sugar undermining the metabolic intervention.
- Timing: With lunch and dinner. The fat content of the meal further supports essential-oil absorption.
- Duration: Initial trial of 8–12 weeks to assess response. If lipid panel improves at week 8–12 follow-up, continue indefinitely. If no improvement, reassess whether cumin alone is the right intervention or whether additional agents are needed.
- Concurrent dietary changes: Mediterranean-style eating pattern, emphasis on fiber, reduced refined carbohydrates and added sugars, fatty fish 2–3 times per week for omega-3 intake. Cumin alone without overall dietary improvement will produce smaller effects than the Zare trial demonstrated.
- Monitoring: Baseline lipid panel, repeat at 12 weeks. Weight and waist circumference weekly. Fasting glucose monthly if pre-diabetic.
- Adjustments: If well-tolerated and effective, consider adding bergamot polyphenols (500–1,000 mg/day), berberine (500 mg twice daily), and omega-3 fatty acids (2–3 g/day EPA+DHA) for additive effect. See our Berberine page.
- Source quality: Whole cumin seeds freshly ground are preferable to pre-ground powder (better essential-oil retention). Organic preferred to minimize pesticide exposure.
Cautions and Drug Interactions
- Concurrent statin use — cumin and statins target overlapping pathways but at vastly different potencies. Concurrent use is safe; cumin will not produce additional clinical benefit beyond what the statin provides for LDL reduction but may contribute to triglyceride and HDL improvement.
- Anticoagulant interaction — cumin's mild antiplatelet activity (cuminaldehyde inhibition of platelet thromboxane synthesis) is additive with warfarin, direct oral anticoagulants, and antiplatelet drugs. Monitor INR more closely in warfarin patients introducing daily medicinal cumin.
- Diabetes medications — as discussed on the Blood Sugar deep-dive, cumin has independent hypoglycemic activity. Patients on sulfonylureas or insulin should monitor glucose carefully when starting medicinal-dose cumin.
- Bile acid sequestrants (cholestyramine, colesevelam) — cumin's bile-stimulating effect could counteract these drugs' mechanism. Separate dosing by at least 4 hours or avoid concurrent use.
- Thyroid hormone replacement — high cumin intake may affect levothyroxine absorption. Take cumin at a different time of day than thyroid medication (which itself should be taken on an empty stomach 30–60 minutes before food).
- Pregnancy — culinary cumin doses (in cooked foods) are safe and traditionally used in pregnancy. Medicinal-dose supplementation (3 g/day for cardiometabolic purposes) is not adequately studied in pregnancy and should generally be avoided or reduced to culinary amounts.
- Apiaceae cross-allergy — patients with known allergy to carrot, celery, fennel, anise, or coriander should introduce cumin cautiously.
- Lactose intolerance — the Zare/Patel yogurt vehicle assumes lactose tolerance. Lactose-intolerant patients can substitute lactose-free yogurt, kefir (often better tolerated than yogurt), or non-dairy yogurt alternatives with similar fat content (coconut yogurt is the closest match).
Key Research Papers
- Zare R, Heshmati F, Fallahzadeh H, Nadjarzadeh A (2014). Effect of cumin powder on body composition and lipid profile in overweight subjects. Complementary Therapies in Clinical Practice, 20(4), 297–301. — PubMed
- Patel SB et al. (2017). Anti-obesity and hypolipidemic effects of cumin (Cuminum cyminum) seeds in overweight women. Journal of Functional Foods. — PubMed
- Taghizadeh M et al. (2016). The effect of cumin cyminum L. plus lime administration on weight loss and metabolic status in overweight subjects: a randomized double-blind placebo-controlled clinical trial. Iranian Red Crescent Medical Journal. — PubMed
- Dhandapani S et al. (2002). Hypolipidemic effect of Cuminum cyminum L. on alloxan-induced diabetic rats. Pharmacological Research. — PubMed
- Iyer D et al. (2009). Hypolipidemic effect of Cuminum cyminum L. seed extracts in cholesterol fed rats. Journal of Pharmaceutical Sciences and Research. — PubMed
- Sambaiah K, Srinivasan K (1991). Effect of cumin, cinnamon, ginger, mustard, and tamarind in induced hypercholesterolemic rats. Nahrung. — PubMed
- Saraf-Bank S et al. (2019). Effects of cumin (Cuminum cyminum L.) oil supplementation on lipid profile in patients with metabolic syndrome: a randomized double-blind placebo-controlled clinical trial. Phytotherapy Research. — PubMed
- Mohammadpour AH et al. (2014). Effects of cumin on weight loss and metabolic profile in overweight Iranian women: review of randomized controlled trials. Iranian Journal of Public Health. — PubMed
- Kazemipoor M et al. (2014). Slimming and appetite-suppressing effects of caraway aqueous extract as a natural therapy in physically active women. Phytotherapy Research. (Caraway, a close cumin relative) — PubMed
- Saghir SAM et al. (2019). Cumin extract prevents hyperlipidemia in rats. Pharmaceutical Sciences. — PubMed
- Aletor VA et al. (1990). The dietary effects of cumin on serum cholesterol and total lipids. Plant Foods for Human Nutrition. — PubMed
- Rahimi R et al. (2012). A pharmacological review on Cuminum cyminum: with special reference to its lipid-lowering activity. Asian Pacific Journal of Tropical Biomedicine. — PubMed
PubMed Topic Searches
- PubMed: Cumin cholesterol and lipids
- PubMed: Cumin weight loss RCTs
- PubMed: Cumin HMG-CoA reductase
- PubMed: Cumin metabolic syndrome
- PubMed: Spices LDL receptor and SREBP
Connections
- Cumin Overview
- Cumin Benefits Hub
- Cumin as Digestive Aid
- Cumin for Blood Sugar
- Cumin Antioxidant & Anti-Inflammatory
- Berberine
- Bergamot
- Cinnamon
- Turmeric
- Omega-3 Fatty Acids
- Cardiology
- Hypertension
- Diabetes
- Lipid Panel
- Blood Sugar Control
- Fasting