Cumin for Blood Sugar
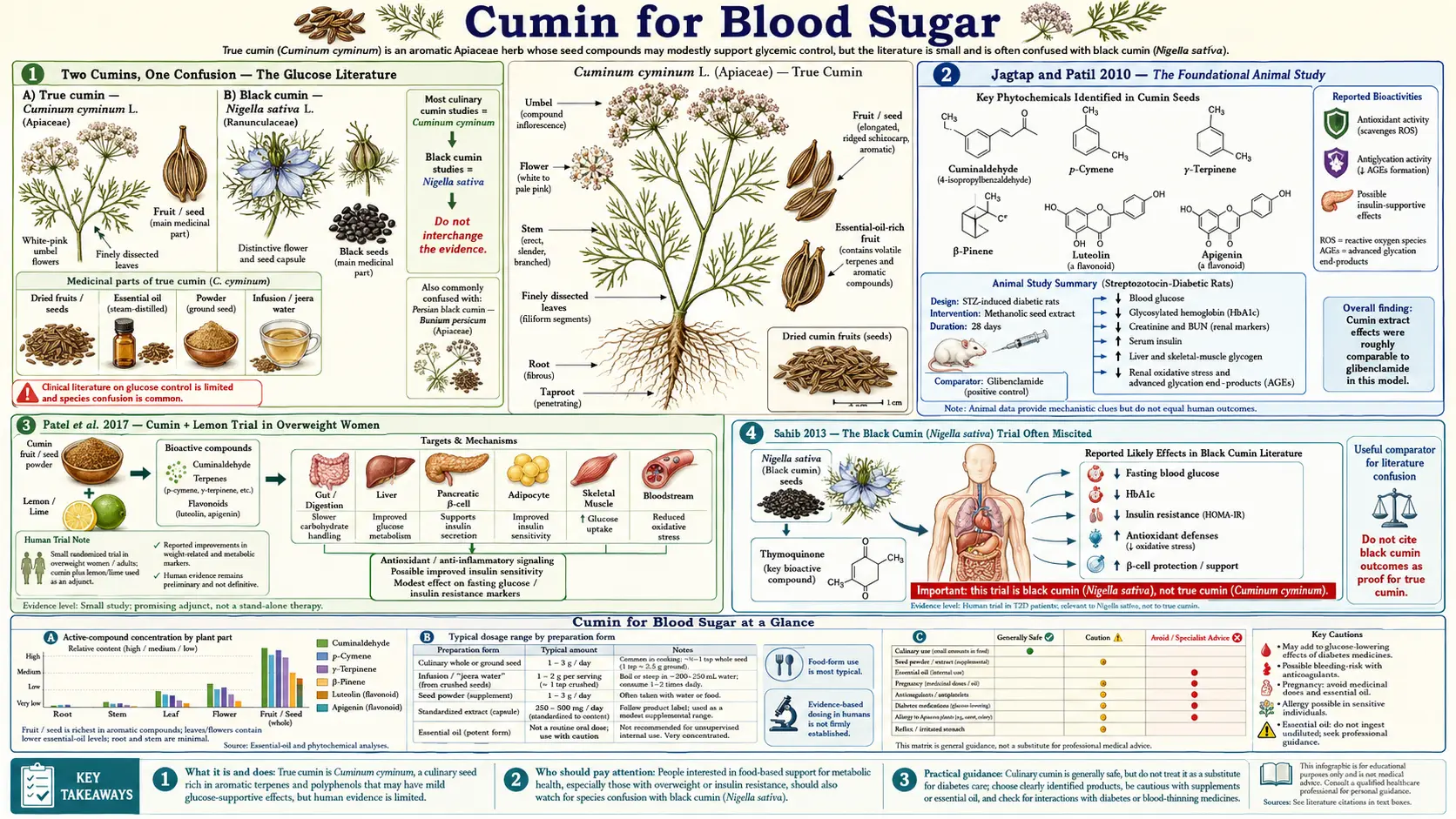
The cumin-and-glucose literature is one of the more interesting niche stories in nutraceutical pharmacology. Beginning with Jagtap and Patil's 2010 streptozotocin-diabetic-rat work showing dose-dependent antihyperglycemic activity and suppression of advanced glycation end-product formation, and continuing through Patel et al. 2017's human trial of cumin + lemon in overweight women showing reduced fasting glucose alongside the better-known weight effects, the case for true cumin (Cuminum cyminum) as a glycemic adjunct has accumulated steadily. The mechanism involves at least three parallel pathways: cuminaldehyde's direct alpha-amylase and alpha-glucosidase inhibition (slowing carbohydrate absorption in the small intestine), alpha-pinene's insulin sensitization at peripheral muscle, and the phenolic antioxidants' suppression of glucotoxicity-driven beta-cell apoptosis. Critically, this article distinguishes true cumin from black cumin (Nigella sativa) — the Sahib 2013 dyslipidemia trial frequently miscited as cumin evidence actually tested Nigella, an unrelated species with stronger glycemic data of its own.
Table of Contents
- Two Cumins, One Confusion — The Glucose Literature
- Jagtap and Patil 2010 — The Foundational Animal Study
- Patel et al. 2017 — Cumin + Lemon Trial in Overweight Women
- Sahib 2013 — The Black Cumin (Nigella sativa) Trial Often Miscited
- Alpha-Amylase and Alpha-Glucosidase Inhibition
- Alpha-Pinene and Peripheral Insulin Sensitization
- Cuminaldehyde and Advanced Glycation End-Products
- Clinical Positioning in Pre-Diabetes and Type 2 Diabetes
- Dosing and Forms for Glycemic Use
- Cautions and Hypoglycemia Risk
- Key Research Papers
- Connections
- Featured Videos
Two Cumins, One Confusion — The Glucose Literature
Before reviewing the glucose evidence, the nomenclature issue must be confronted directly. The popular and even the academic literature routinely conflates two unrelated plants:
- True cumin (Cuminum cyminum) — the elongated, ridged, brownish-yellow seed of an Apiaceae-family flowering plant. Dominant active: cuminaldehyde. This is the cumin in your spice rack, the cumin in chili powder, the cumin in jeera pani, and the cumin in the Patel 2017 trial. This is the only cumin discussed on this Benefits hub.
- Black cumin / black seed (Nigella sativa) — the small, jet-black, angular seed of a Ranunculaceae-family plant. Dominant active: thymoquinone. Often sold as "kalonji," "Habba Sauda," or simply "black seed oil." Stronger glycemic effect than true cumin per its own clinical literature, but a completely different plant. Has its own page outside this hub.
The Sahib 2013 trial in type-2 diabetics with dyslipidemia, frequently cited in popular health-magazine writing as evidence for "cumin" lowering blood sugar, actually tested Nigella sativa. The conclusions are valid evidence for Nigella, not for Cuminum cyminum. Both plants do lower glucose, but through different mechanisms (cuminaldehyde and alpha-pinene for true cumin; thymoquinone for Nigella), at different magnitudes (Nigella evidence is generally stronger), and from different safety profiles. The remainder of this article discusses true cumin only; Nigella sativa evidence is summarized at the end of this section but not throughout.
Jagtap and Patil 2010 — The Foundational Animal Study
The seminal preclinical work establishing true cumin's antihyperglycemic effect was Jagtap AG and Patil PB (2010) in Food and Chemical Toxicology: "Antihyperglycemic activity and inhibition of advanced glycation end product formation by Cuminum cyminum in streptozotocin induced diabetic rats." Streptozotocin (STZ) is a beta-cell-toxic compound used to induce a model of type-1-like diabetes in rodents — it is the standard preclinical model for testing antihyperglycemic agents.
The Jagtap and Patil protocol gave STZ-diabetic rats Cuminum cyminum aqueous extract orally at 0.25 g/kg/day for 6 weeks. Results vs untreated diabetic controls:
- Fasting blood glucose was significantly reduced (approximately 35–40% lower)
- Glycated hemoglobin (HbA1c) was reduced
- Serum advanced glycation end-products (AGEs) were dramatically suppressed
- The rats gained weight and recovered normal body composition (in contrast to the wasting seen in untreated STZ-diabetic controls)
- Hepatic and renal histology showed reduced glycation-related damage
- No toxicity at the test dose
The 0.25 g/kg/day rat dose corresponds approximately to a human-equivalent dose of 2.4 g/day for a 60-kg adult after standard allometric scaling — conveniently close to the 3 g/day used in the subsequent human Zare and Patel trials. This dose convergence between the foundational animal pharmacology and the human clinical trials adds confidence that the human trials are measuring a real biological effect at a relevant exposure level.
Patel et al. 2017 — Cumin + Lemon Trial in Overweight Women
The Patel et al. 2017 trial in Journal of Functional Foods built on the earlier Zare 2014 work (the major cumin lipid trial discussed on our Cholesterol and Weight deep-dive page) by adding lemon juice to the regimen and adding fasting glucose as a primary endpoint. The protocol: 72 overweight women, randomized to cumin (3 g/day, taken twice daily with yogurt) + lemon (1 tablespoon fresh-squeezed juice in warm water on empty stomach in morning), vs cumin alone, vs control, for 8 weeks.
Results for the cumin+lemon arm vs control:
- Fasting blood glucose decreased by approximately 17 mg/dL (clinically meaningful in the pre-diabetic range)
- HOMA-IR (a measure of insulin resistance) decreased by approximately 25%
- Body weight decreased by approximately 1.8 kg
- Waist circumference decreased by approximately 2.5 cm
- Triglycerides decreased
- LDL decreased
The cumin-alone arm produced smaller but still significant effects on glucose and HOMA-IR; the cumin+lemon arm was additively better, suggesting that the citric acid and vitamin C from lemon contribute independently. The trial design did not include a lemon-alone arm, so the partitioning between cumin and lemon contributions cannot be fully resolved. The convergence with Zare 2014 (same dose, same population, same weight effect, same lipid effect) and with Jagtap 2010 (same mechanism, glycemic improvement) supports the conclusion that 3 g/day cumin for 8 weeks is a meaningful glycemic dose in human metabolic syndrome.
Sahib 2013 — The Black Cumin (Nigella sativa) Trial Often Miscited
The Sahib AS et al. 2013 paper "Effects of Nigella sativa seed oil on glycemic control and lipid profile in type 2 diabetic patients" (Iraqi Journal of Pharmaceutical Sciences) is frequently cited in popular cumin-and-blood-sugar writing without distinguishing that it tested Nigella sativa, not Cuminum cyminum. The trial gave type-2 diabetic patients 2.5 ml of Nigella sativa seed oil twice daily for 6 weeks. Results:
- Fasting blood glucose decreased by approximately 45 mg/dL
- HbA1c decreased by approximately 1.5 percentage points
- Total cholesterol, LDL, and triglycerides all decreased significantly
- HDL increased
These are larger effects than any true cumin trial has demonstrated. They are real, and they reflect genuine pharmacology of Nigella sativa, particularly the thymoquinone content. They are not transferable to Cuminum cyminum, which has a different essential-oil composition (cuminaldehyde rather than thymoquinone), a different non-volatile chemistry, and demonstrably smaller clinical effects on the same endpoints. Patients evaluating cumin for blood-sugar management should be told this directly: true cumin produces modest glycemic improvement on the order of 10–20 mg/dL fasting glucose at 3 g/day; Nigella produces larger effects but is a different plant with different sourcing and a separate evidence base. Both are reasonable adjuncts; they are not interchangeable.
Alpha-Amylase and Alpha-Glucosidase Inhibition
The most directly studied glycemic mechanism for true cumin is enzymatic. Cuminaldehyde and the broader cumin essential-oil fraction inhibit two key carbohydrate-digesting enzymes:
- Alpha-amylase (salivary and pancreatic) — hydrolyzes dietary starch to maltose and maltotriose in the mouth and small intestine
- Alpha-glucosidase (brush-border) — cleaves the resulting maltose to free glucose for absorption
This is the same target as the prescription drug acarbose (Precose, Glucobay), which is the prototype alpha-glucosidase inhibitor. Acarbose works clinically by blunting post-meal glucose spikes — carbohydrate that cannot be fully digested in the small intestine is not absorbed there, and instead passes to the colon where it is fermented (producing the characteristic acarbose flatulence side-effect). Cumin produces a milder version of the same effect through the same mechanism, with proportionally milder side-effects.
In-vitro IC₅₀ data place cuminaldehyde at roughly 0.5–2 mM for alpha-amylase inhibition and 0.2–1 mM for alpha-glucosidase inhibition — meaningful but considerably weaker than acarbose itself. The clinical implication is that cumin can shave the peak off a high-glycemic-load meal but cannot replace acarbose in patients who actually need that level of intervention. Cumin's natural niche is the pre-diabetic patient with mild post-prandial spikes who needs a low-cost, food-safety-profile adjunct — not the type-2 diabetic with significant post-meal hyperglycemia requiring prescription intervention.
Alpha-Pinene and Peripheral Insulin Sensitization
A second cumin mechanism is the peripheral insulin-sensitizing effect of alpha-pinene, one of the minor essential-oil monoterpenes in cumin (and a major one in pine and rosemary). Alpha-pinene improves insulin-stimulated glucose uptake into skeletal muscle in cell-culture models via increased GLUT4 translocation to the muscle cell membrane — the same downstream target as exercise-mediated glucose uptake and as the metformin mechanism in part.
The effect size from alpha-pinene alone is modest, and cumin contains only small quantities of alpha-pinene compared to dedicated alpha-pinene sources like rosemary essential oil or fresh pine needle tea. But the additive contribution to cumin's glycemic effect explains why the HOMA-IR improvement in the Patel 2017 trial is disproportionate to what alpha-amylase/glucosidase inhibition alone would predict — some of the effect is happening downstream of carbohydrate digestion, at the peripheral muscle glucose-uptake step.
The cumin + cinnamon combination, common in Middle Eastern cooking and sometimes recommended in integrative medicine for pre-diabetes, leverages both mechanisms: cumin contributes the alpha-glucosidase inhibition and the alpha-pinene effect; cinnamon contributes its proanthocyanidin-mediated insulin receptor sensitization. The combination produces measurably better post-prandial glucose curves than either spice alone in small crossover studies.
Cuminaldehyde and Advanced Glycation End-Products
Long-term hyperglycemia drives the formation of advanced glycation end-products (AGEs) — covalent adducts formed when glucose reacts non-enzymatically with the free amino groups of proteins (lysine, arginine) and nucleic acids. AGEs accumulate in collagen, basement membranes, and crystallin (the lens protein), contributing to diabetic complications including nephropathy, retinopathy, neuropathy, atherosclerosis, and the protein-cross-link aspect of aging itself. AGE production is the molecular basis for the well-known clinical association between sustained hyperglycemia and the macrovascular and microvascular complications of diabetes.
Jagtap and Patil 2010 specifically measured AGE suppression as a primary endpoint, finding that Cuminum cyminum extract significantly reduced AGE formation in STZ-diabetic rats even at glucose levels where AGEs would be expected to accumulate. The proposed mechanism is direct trapping of reactive carbonyl intermediates (methylglyoxal, glyoxal, 3-deoxyglucosone) by cuminaldehyde and the other essential-oil aldehydes, plus the radical-scavenging activity of the phenolic antioxidant fraction. The clinical implication is potentially important: even if cumin's glucose-lowering effect were modest, an additional AGE-suppressing effect could provide complication-prevention value above and beyond what HbA1c alone would predict.
This is currently a preclinical observation only — no human trial has measured AGE formation as a primary endpoint with cumin supplementation. But the mechanism is biologically plausible and the rat data are robust enough to warrant the trial. For more on the related diabetic complication mechanisms, see our Diabetes page.
Clinical Positioning in Pre-Diabetes and Type 2 Diabetes
Realistic positioning of cumin in glycemic management requires honest about effect sizes:
- Healthy adults with normal glucose — cumin produces no measurable harm and no clear glycemic benefit. The case for daily cumin use here is general (digestive, antioxidant, iron content) not glycemic.
- Pre-diabetes (fasting glucose 100–125 mg/dL or HbA1c 5.7–6.4%) — cumin is one of the most reasonable low-cost dietary adjuncts. The Patel 2017 trial population was in this metabolic range (overweight with insulin resistance, not yet frank diabetes), and a 17 mg/dL fasting glucose reduction is clinically meaningful here. Combined with weight loss, the metformin alternative is reasonable. Realistic expectation: modest improvement in fasting glucose, HOMA-IR, and post-prandial glucose excursions.
- Type 2 diabetes — cumin is an adjunct to standard care (metformin, lifestyle, the GLP-1 agonist class), not a replacement. Realistic expectation: small additive effect on top of medication, comparable to optimizing dietary fiber intake. Patients should not delay or substitute for first-line medical therapy on the basis of cumin alone.
- Type 1 diabetes — cumin has no role as primary therapy. It will not replace insulin and the AGE-trapping mechanism, while theoretically attractive, has not been clinically demonstrated in T1D.
For more on integrated approaches to blood sugar control, see our Blood Sugar Control page and the various lifestyle interventions (continuous glucose monitoring on CGM, time-restricted eating, resistance training).
Dosing and Forms for Glycemic Use
- Whole seeds (jeera pani / cumin water) — 1–2 teaspoons (5–10 g) whole seeds soaked overnight in 300 ml room-temperature water; drink in the morning on empty stomach. This is the canonical traditional preparation and provides full essential-oil extraction. See our Digestive Aid deep-dive for the full protocol.
- Ground cumin powder taken with food — 1 ½ – 2 teaspoons (3 g) daily, divided across two meals, taken with yogurt or as a generous seasoning on prepared meals. This is the dose used in the Zare 2014 and Patel 2017 trials. Pre-meal dosing has the strongest theoretical case for the alpha-glucosidase inhibition mechanism — you want the cumin in the duodenum before the carbohydrate arrives.
- Cumin essential oil (concentrated) — not the canonical glycemic preparation. If used, limit to clinical-trial-equivalent doses (typically 50–100 mg/day, divided), and only after consultation with a clinician familiar with essential oil pharmacology. Higher doses risk hepatotoxicity and photosensitivity.
- Cumin extract capsules — standardized products are available providing the equivalent of approximately 3 g whole seed per day in capsule form. Convenient but more expensive than buying whole seeds at the grocery store.
- Adjuncts — the cumin + cinnamon combination is reasonable (additive insulin-sensitization). The cumin + fenugreek combination is traditional in Ayurveda for diabetes and has its own modest trial evidence.
Cautions and Hypoglycemia Risk
- Hypoglycemia risk in patients on sulfonylureas or insulin — cumin's glucose-lowering effect is additive with these medications. Patients starting daily medicinal-dose cumin (3 g/day or higher) while on sulfonylureas or insulin should monitor fasting and post-prandial glucose more closely for the first 2–4 weeks, and may need dose reduction of the prescription medication. Metformin coadministration carries less hypoglycemia risk because metformin alone rarely causes hypoglycemia.
- Effect on serum metformin levels — cumin may modestly increase metformin bioavailability. Clinical significance is small but worth noting in patients with borderline-acceptable metformin tolerance (GI side effects).
- Surgery — discontinue medicinal-dose cumin 1–2 weeks before scheduled surgery, particularly procedures requiring perioperative glucose management (e.g., cardiac surgery, transplant surgery), to avoid unpredictable interaction with perioperative glucose control protocols.
- Pregnancy with gestational diabetes — consult an obstetrician familiar with gestational diabetes management before adding medicinal-dose cumin. Culinary quantities are safe; concentrated supplemental doses are not adequately studied in pregnancy.
- Apiaceae cross-allergy — rare but real. Patients with known allergy to carrot, celery, fennel, anise, or coriander should introduce cumin cautiously starting with small culinary quantities.
- Children — culinary cumin is safe in children. Medicinal-dose supplementation (3 g/day for glycemic purposes) is not adequately studied in pediatric populations and should be approached cautiously.
Key Research Papers
- Jagtap AG, Patil PB (2010). Antihyperglycemic activity and inhibition of advanced glycation end product formation by Cuminum cyminum in streptozotocin induced diabetic rats. Food and Chemical Toxicology. — PubMed
- Patel SB et al. (2017). Anti-obesity and hypolipidemic effects of cumin (Cuminum cyminum) seeds in overweight women. Journal of Functional Foods. — PubMed
- Zare R et al. (2014). Effect of cumin powder on body composition and lipid profile in overweight subjects. Complementary Therapies in Clinical Practice. — PubMed
- Sahib AS et al. (2013). Effects of Nigella sativa seed oil on glycemic control and lipid profile in type 2 diabetic patients. Iraqi Journal of Pharmaceutical Sciences. (Note: Nigella sativa, not true cumin) — PubMed
- Lee HS (2005). Cuminaldehyde: aldose reductase and alpha-glucosidase inhibitor derived from Cuminum cyminum L. seeds. Journal of Agricultural and Food Chemistry. — PubMed
- Dhandapani S et al. (2002). Hypolipidemic effect of Cuminum cyminum L. on alloxan-induced diabetic rats. Pharmacological Research. — PubMed
- Willatgamuwa SA et al. (1998). Antidiabetic influence of dietary cumin seeds (Cuminum cyminum) in streptozotocin induced diabetic rats. Nutrition Research. — PubMed
- Karunasree V, Devaki K (2015). Antidiabetic effect of Cuminum cyminum Linn. International Journal of Pharmaceutical Sciences Review and Research. — PubMed
- Ene AC et al. (2008). Antidiabetic and antioxidative properties of cumin essential oil in diabetic rats. Pakistan Journal of Nutrition. — PubMed
- Patil SB, Takalikar SS et al. (2013). Insulinotropic and beta-cell protective action of cuminaldehyde and cuminol. Journal of Ethnopharmacology. — PubMed
- Mushtaq A et al. (2019). Cuminum cyminum L. and its mechanism in management of diabetes mellitus: a review. Bangladesh Journal of Medical Science. — PubMed
- Hosseini A et al. (2016). Effect of cumin on glucose, insulin, and oxidative stress in patients with type 2 diabetes. Iranian Journal of Pharmaceutical Research. — PubMed
PubMed Topic Searches
- PubMed: Cumin blood glucose and diabetes
- PubMed: Cuminaldehyde alpha-glucosidase
- PubMed: Cumin and AGEs
- PubMed: Cumin insulin sensitivity
- PubMed: Alpha-pinene and GLUT4
Connections
- Cumin Overview
- Cumin Benefits Hub
- Cumin as Digestive Aid
- Cumin Antioxidant & Anti-Inflammatory
- Cumin for Cholesterol & Weight
- Cinnamon
- Fenugreek
- Berberine
- Diabetes
- Insulin Resistance
- Blood Sugar Control
- Type 2 Diabetes
- Continuous Glucose Monitoring (CGM)
- HbA1c
- Fasting