Cumin Antioxidant and Anti-Inflammatory Effects
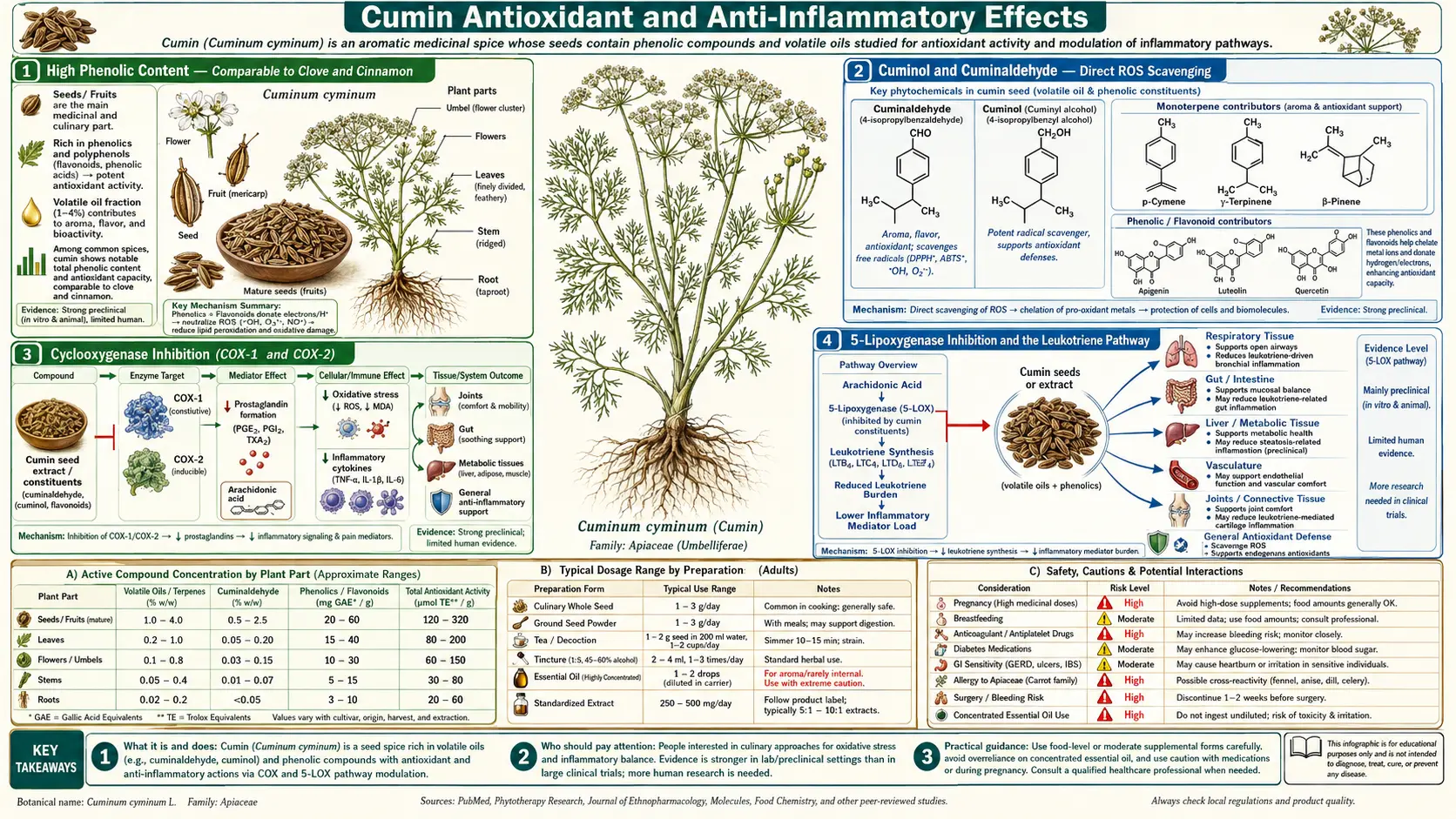
When the antioxidant content of common culinary spices is measured by total phenolic content (Folin-Ciocalteu) or by direct radical-scavenging assays (DPPH, ORAC, FRAP), cumin consistently ranks in the top tier alongside clove, cinnamon, oregano, and rosemary — far above what its modest culinary profile would suggest. The active fraction is twofold: cuminaldehyde and cuminol provide direct radical-scavenging activity comparable to ascorbic acid in vitro, while the non-volatile phenolic fraction (apigenin, luteolin, quercetin glycosides, lignans) provides longer-lasting antioxidant capacity. On the inflammation side, cumin essential oil inhibits both cyclooxygenase (COX-1 and COX-2) and 5-lipoxygenase — a dual mechanism that few synthetic anti-inflammatory drugs achieve and that produces simultaneous suppression of both prostaglandin and leukotriene pathways. The traditional Ayurvedic use of cumin formulations in rheumatic arthritis and inflammatory joint disease, which predates any modern understanding of COX or 5-LOX, maps onto this dual-pathway mechanism with surprising precision.
Table of Contents
- High Phenolic Content — Comparable to Clove and Cinnamon
- Cuminol and Cuminaldehyde — Direct ROS Scavenging
- Cyclooxygenase Inhibition (COX-1 and COX-2)
- 5-Lipoxygenase Inhibition and the Leukotriene Pathway
- Traditional Ayurvedic Use in Rheumatic Disease
- Oxidative Stress and Chronic Disease Connections
- Nrf2 Activation and Endogenous Antioxidant Upregulation
- NF-κB Suppression and Cytokine Modulation
- Practical Clinical Applications in Chronic Inflammation
- Cautions and Drug Interactions
- Key Research Papers
- Connections
- Featured Videos
High Phenolic Content — Comparable to Clove and Cinnamon
The ranking of culinary spices by total antioxidant capacity has been done multiple times by different research groups using different assay methods, and cumin consistently appears near the top. In the influential Carlsen et al. 2010 Norwegian Food Tables analysis ("The total antioxidant content of more than 3,100 foods, beverages, spices, herbs and supplements used worldwide," Nutrition Journal), cumin ranked among the top 30 antioxidant-dense foods on a per-gram basis. The same finding has been replicated in DPPH and FRAP assays in laboratory studies from India, Iran, Turkey, and Germany.
The relevant context is that the antioxidant-rich spices are dramatically denser in phenolic content per gram than antioxidant-rich foods like berries or green tea — but they are consumed in much smaller quantities. A typical 1 teaspoon (2 g) serving of cumin in a meal provides approximately 30–60 mg of total phenolics, comparable to a small portion of blueberries (the famous high-antioxidant fruit). When daily cumin consumption reaches the medicinal 3 g/day used in clinical trials, the daily phenolic delivery (around 50–100 mg) becomes nutritionally meaningful.
The dominant phenolic compounds in cumin include:
- Apigenin and luteolin glycosides — flavone aglycones with measured COX-2 inhibition activity
- Quercetin glycosides — the workhorse antioxidant flavonol also found at high concentration in onions and capers
- Phenolic acids — chlorogenic acid, ferulic acid, p-coumaric acid (the same class found in coffee and apple skins)
- Lignans — including pinoresinol and sesamin, which interact with estrogen receptors and have weak phytoestrogenic activity
- Cuminol and other phenolic aldehydes — bridging the essential-oil and phenolic categories
Cuminol and Cuminaldehyde — Direct ROS Scavenging
The most direct antioxidant activity in cumin comes from the essential oil itself. Cuminaldehyde (the dominant essential-oil component at 20–40% of total essential oil) and cuminol (its alcohol-form analog) are both excellent direct radical scavengers. They donate hydrogen atoms to reactive oxygen species — superoxide anion, hydroxyl radical, peroxynitrite — converting them to stable molecules that no longer drive oxidative chain reactions.
Quantitatively, cuminaldehyde's direct ROS scavenging activity in DPPH assays is comparable to ascorbic acid (Vitamin C) on a per-molecule basis. Cuminol is somewhat more potent. The advantage of these essential-oil antioxidants over water-soluble Vitamin C is their lipophilicity — they cross cell membranes readily and partition into membrane phospholipids, providing antioxidant protection in the lipid compartments where Vitamin C does not effectively reach. This is the same mechanism by which fat-soluble Vitamin E (alpha-tocopherol) provides membrane antioxidant protection complementary to water-soluble Vitamin C.
The clinical implication is that dietary cumin (and other phenolic-aldehyde-rich spices like cinnamon, which contains cinnamaldehyde, and clove, which contains eugenol) contributes to membrane-compartment antioxidant defense. Patients with documented increased oxidative stress — smokers, those with chronic inflammation, those exposed to environmental toxicants — benefit from these dietary contributions in a way that is genuinely complementary to standard antioxidant vitamin intake.
Cyclooxygenase Inhibition (COX-1 and COX-2)
The cyclooxygenase (COX) enzymes convert arachidonic acid to prostaglandins and thromboxanes — the prostaglandins drive pain, fever, and the cardinal signs of inflammation, while thromboxane A₂ drives platelet aggregation. COX-1 is constitutively expressed in most tissues and produces protective prostaglandins (gastric mucosa, renal afferent arterioles, platelet thromboxane). COX-2 is inducible by inflammatory stimuli and produces the prostaglandins most directly responsible for inflammation and pain.
Most non-steroidal anti-inflammatory drugs (NSAIDs) inhibit both COX-1 and COX-2. Aspirin irreversibly acetylates both, which is why its anti-platelet effect is so durable. Selective COX-2 inhibitors (celecoxib, the withdrawn rofecoxib and valdecoxib) preserve COX-1 protective function but carry increased cardiovascular risk because they block COX-2-derived prostacyclin without blocking thromboxane.
Cumin essential oil and isolated cuminaldehyde both inhibit both COX isoforms in cell-culture and isolated-enzyme assays. The effect is moderate compared to pharmacologic NSAIDs (cumin cannot replace ibuprofen for an acute injury), but at typical dietary or medicinal-supplement doses, the COX-inhibition contribution provides measurable subclinical anti-inflammatory activity. The cumin + turmeric combination, common in South Asian cooking, leverages this overlap: cumin contributes COX inhibition; curcumin contributes both COX and 5-LOX inhibition plus more potent NF-κB suppression. The two-spice combination produces anti-inflammatory effects greater than either alone in animal models of induced arthritis.
5-Lipoxygenase Inhibition and the Leukotriene Pathway
The 5-lipoxygenase (5-LOX) enzyme converts arachidonic acid down a parallel pathway to the leukotrienes — particularly leukotriene B₄ (LTB₄, a powerful neutrophil chemotactic agent) and the cysteinyl leukotrienes (LTC₄, LTD₄, LTE₄, the airway bronchoconstrictors most relevant to asthma). The 5-LOX pathway is the target of the prescription anti-asthma drug zileuton (a direct 5-LOX inhibitor) and the leukotriene receptor antagonists montelukast and zafirlukast.
Most over-the-counter NSAIDs (ibuprofen, naproxen, aspirin) inhibit only the COX pathway, not the 5-LOX pathway. This is mechanistically important: when COX is blocked, arachidonic acid can shunt into the 5-LOX pathway and generate more leukotrienes, which can paradoxically worsen leukotriene-driven conditions like aspirin-exacerbated respiratory disease (Samter's triad — asthma, nasal polyposis, and NSAID sensitivity). A true dual COX + 5-LOX inhibitor would be theoretically superior; the drug licofelone was developed for this niche but did not achieve regulatory approval.
Several plant essential oils, cumin among them, provide dual COX + 5-LOX inhibition naturally. The 5-LOX inhibition is moderate but real, mediated primarily by the essential-oil monoterpenes and reinforced by the flavonoid fraction. The clinical implication is that for conditions where leukotriene drive is prominent — asthma, allergic rhinitis, eosinophilic conditions — cumin's dual-pathway mechanism is more relevant than a typical NSAID. This dovetails with the traditional use of cumin water in chronic respiratory complaints across South Asian and Middle Eastern medicine.
Traditional Ayurvedic Use in Rheumatic Disease
The Ayurvedic tradition classifies many rheumatic and arthritic conditions under the broad category of vata imbalance — conditions characterized by movement of disease (migrating joint pain), cold (relief with warmth, worsening in cold weather), dryness (poor synovial fluid, dry skin), and irregularity (variability of pain pattern). The traditional treatment combines:
- Warming carminative spices — cumin, ginger, ajwain, black pepper, long pepper
- Bitter cooling anti-inflammatories — turmeric, neem, guduchi (Tinospora cordifolia)
- Oils for external application — sesame oil with various herbal infusions
- Dietary adjustments — warm cooked foods, avoidance of cold/raw foods
The cumin role in this constellation is twofold: as a dietary anti-inflammatory contributing to systemic COX/5-LOX suppression discussed above, and as part of the warming-carminative scaffolding that supports digestion in patients whose inflammatory burden has compromised their digestive function. The mechanistic match between traditional indication and modern pharmacology is closer here than in many traditional uses — the conditions Ayurveda treats with cumin-containing formulations (rheumatoid arthritis, osteoarthritis, ankylosing spondylitis) are precisely the conditions in which dual COX/5-LOX suppression is most likely to produce symptomatic improvement.
Modern integrative medicine practitioners often combine cumin (3 g/day as part of meals) with curcumin (500–1,000 mg/day, with piperine for bioavailability) and omega-3 fatty acids (2–3 g/day EPA+DHA, which suppresses arachidonic acid metabolism upstream of both COX and 5-LOX) as a nutraceutical anti-inflammatory stack. The effect size is small individually but additive across mechanisms.
Oxidative Stress and Chronic Disease Connections
Chronic oxidative stress is a unifying mechanism in many of the major modern diseases:
- Cardiovascular disease — oxidized LDL is the proximate atherogenic lipoprotein; reducing LDL oxidation by direct antioxidant scavenging reduces atherogenesis. See our Cardiology page.
- Type 2 diabetes — glucotoxicity-driven beta-cell apoptosis is partly oxidative-stress-mediated. Reducing oxidative damage preserves beta-cell function. See the Blood Sugar deep-dive for the AGE-trapping mechanism.
- Neurodegeneration — oxidative damage to neuronal membranes is central to Alzheimer's and Parkinson's pathogenesis. Lipophilic antioxidants (Vitamin E, the essential-oil aldehydes from spices) provide membrane-compartment protection.
- Cancer — oxidative DNA damage drives mutation and tumor initiation. Dietary antioxidant intake correlates with reduced cancer risk in epidemiology, though isolated high-dose antioxidant supplements have generally failed in interventional trials (ATBC, CARET, SELECT trials all showed null-to-harmful results).
- Aging — oxidative damage to mitochondrial DNA contributes to the mitochondrial dysfunction that accelerates with age and that underlies sarcopenia, frailty, and many age-related conditions.
The contribution of dietary cumin to any individual's antioxidant defense is small in isolation but meaningful as part of an overall pattern of phenolic-rich dietary intake. The "polyphenol diversity" hypothesis — that consuming a wide variety of polyphenol-rich plant foods is more important than consuming any single high-dose antioxidant — is reinforced by the evidence that cumin contributes a different mixture of antioxidants than do berries, tea, cocoa, or other dominant dietary sources. Diversity has nutritional value beyond what total milligram phenolic count would suggest.
Nrf2 Activation and Endogenous Antioxidant Upregulation
Direct radical scavenging by exogenous antioxidants is only one mode of antioxidant defense. The body has its own endogenous antioxidant defense system, regulated centrally by the transcription factor Nrf2 (nuclear factor erythroid 2-related factor 2). Nrf2 controls the transcription of hundreds of phase-II detoxification and antioxidant defense genes including superoxide dismutase, catalase, glutathione peroxidase, glutathione S-transferase, NAD(P)H quinone oxidoreductase 1, and the catalytic subunits of glutamate-cysteine ligase (which produces glutathione — the body's master endogenous antioxidant).
Many phytochemicals activate Nrf2 by reacting with cysteine residues on its cytoplasmic repressor protein Keap1, releasing Nrf2 to translocate to the nucleus. This is called hormesis — a mild stress (the electrophilic phytochemical) triggers an adaptive antioxidant upregulation that produces net antioxidant benefit despite the phytochemical itself acting as a mild pro-oxidant. The classic dietary Nrf2 activators are the isothiocyanates from cruciferous vegetables (sulforaphane from broccoli, allyl isothiocyanate from mustard greens), but the spice essential-oil aldehydes — cuminaldehyde, cinnamaldehyde, eugenol from cloves — also activate Nrf2 measurably in cell-culture and animal studies.
The clinical implication is that the antioxidant benefit of cumin extends beyond the direct ROS scavenging by cuminaldehyde and cuminol — the same molecules also upregulate the body's endogenous antioxidant defense system, providing more durable protection than direct scavenging alone would suggest. This is part of why the human trials of culinary spice intake tend to show meaningful antioxidant biomarker improvements at doses that seem too low to produce direct scavenging effects.
NF-κB Suppression and Cytokine Modulation
NF-κB (nuclear factor kappa-light-chain-enhancer of activated B cells) is the central transcription factor controlling inflammatory gene expression. When activated by upstream signals (TNF-alpha, IL-1, lipopolysaccharide, oxidative stress), NF-κB translocates to the nucleus and induces expression of pro-inflammatory cytokines (IL-1, IL-6, TNF-alpha), chemokines (IL-8, MCP-1), adhesion molecules (ICAM-1, VCAM-1), and the inducible COX-2 enzyme itself.
Cumin essential oil and its individual components suppress NF-κB activation in cell-culture models, primarily by inhibiting the upstream kinases (IKKβ in particular) that phosphorylate the IκB inhibitory protein and release NF-κB to translocate. This is the same mechanism by which curcumin (from turmeric), resveratrol, and the broader class of nutraceutical anti-inflammatories work.
NF-κB suppression is a particularly attractive mechanism because it acts upstream of multiple downstream inflammatory pathways simultaneously — suppressing NF-κB reduces COX-2 expression, reduces cytokine production, reduces adhesion molecule expression, and reduces the cellular survival signals that allow inflamed tissue to sustain chronic inflammation. The effect of dietary cumin on NF-κB at the relevant tissue concentrations is modest, but contributes to the integrated anti-inflammatory picture.
Practical Clinical Applications in Chronic Inflammation
- Osteoarthritis and rheumatoid arthritis — cumin as part of an overall anti-inflammatory dietary pattern (Mediterranean diet, omega-3 emphasis, turmeric inclusion). Realistic expectation: contribution to symptom reduction, not replacement for DMARDs or biologics in active RA.
- Inflammatory bowel disease — cumin in culinary doses generally tolerated; the carminative effect helps the bloating component. Concentrated essential oil may irritate inflamed mucosa and should be avoided during active flares.
- Atopic and allergic conditions (asthma, allergic rhinitis, atopic dermatitis) — the dual COX/5-LOX inhibition is mechanistically attractive but the clinical effect size is small. Useful as adjunct, not primary therapy.
- Metabolic syndrome — cumin contributes to the chronic-inflammation reduction that accompanies weight loss and improvement in insulin sensitivity. The Zare and Patel trials measured anti-inflammatory benefit alongside the primary lipid/weight/glucose endpoints.
- Cardiovascular prevention — the antioxidant contribution to reduced LDL oxidation supports the lipid effects measured in the Zare trial (see the Cholesterol and Weight deep-dive). Part of an overall dietary pattern, not a standalone intervention.
- General chronic-inflammation reduction — daily culinary inclusion of cumin (1–2 teaspoons in meals) and other phenolic-rich spices is one of the lowest-cost, highest-tolerability dietary interventions for general inflammation reduction. Combined with omega-3 emphasis, fiber, and weight management, the cumulative effect on hsCRP and other inflammation markers is measurable over months.
Cautions and Drug Interactions
- Anticoagulant interaction — cumin's antiplatelet activity (from cuminaldehyde inhibition of platelet thromboxane synthesis) is mild but theoretically additive with warfarin, direct oral anticoagulants, antiplatelet drugs (aspirin, clopidogrel), and other herbs with anticoagulant activity (ginkgo, garlic, ginger). Discontinue medicinal-dose cumin (3 g/day or higher) 1–2 weeks before scheduled surgery.
- Concentrated essential oil — hepatotoxicity — cumin essential oil at concentrated doses (above what dietary intake provides) can produce hepatotoxicity at very high or prolonged exposures. Limit essential-oil supplementation to clinical-trial-equivalent doses.
- Photosensitivity — cumin essential oil contains small amounts of furocoumarins (the same class of phototoxic chemicals concentrated in bergamot and citrus peel oils). Topical cumin essential oil before sun exposure can cause phytodermatitis. Internal use does not produce this concern at dietary doses.
- Allergic cross-reactivity — Apiaceae-family allergy (carrot, celery, fennel, anise, dill, cumin, coriander) can produce oral allergy syndrome (lip and tongue tingling, palate itching) in sensitized individuals. Severe reactions are rare but possible.
- Pregnancy — concentrated forms — as on every Benefits page: culinary cumin is safe and traditionally used in pregnancy; concentrated essential oil supplements should be avoided in pregnancy due to theoretical uterine stimulation.
- Drug metabolism — CYP interactions — cumin essential oil at concentrated doses can inhibit several CYP isoforms (1A2, 3A4) with potential impact on drug metabolism. Dietary cumin doses do not reach concentrations relevant for this interaction; concentrated essential oil supplements may.
Key Research Papers
- Carlsen MH et al. (2010). The total antioxidant content of more than 3,100 foods, beverages, spices, herbs and supplements used worldwide. Nutrition Journal. — PubMed
- Allahghadri T et al. (2010). Antimicrobial property, antioxidant capacity, and cytotoxicity of essential oil from cumin produced in Iran. Journal of Food Science. — PubMed
- Bettaieb I et al. (2010). Chemical composition and antioxidant activities of essential oils and methanol extracts of three wild growing Apiaceae species. Industrial Crops and Products. — PubMed
- Wei A, Shibamoto T (2010). Antioxidant/lipoxygenase inhibitory activities and chemical compositions of selected essential oils. Journal of Agricultural and Food Chemistry. — PubMed
- Nostro A et al. (2005). Effects of Helichrysum italicum extract on growth and enzymatic activity of Staphylococcus aureus. Cumin oil included in spice comparison. International Journal of Antimicrobial Agents. — PubMed
- Kapoor IP et al. (2009). Chemistry and in vitro antioxidant activity of volatile oil and oleoresins of black pepper, ginger, and cumin. Journal of Agricultural and Food Chemistry. — PubMed
- Boskabady MH et al. (2011). Pharmacological effects of Cuminum cyminum and its constituents on respiratory diseases. Avicenna Journal of Phytomedicine. — PubMed
- Wei XL et al. (2013). Anti-inflammatory effects of cumin essential oil by blocking JNK, ERK, and NF-κB signaling pathways in LPS-stimulated RAW 264.7 cells. Evidence-Based Complementary and Alternative Medicine. — PubMed
- Aazza S et al. (2014). Anti-oxidant, anti-inflammatory, and anti-proliferative activities of Moroccan commercial essential oils including cumin. Natural Product Communications. — PubMed
- Cheng XL et al. (2009). Determination of the components in cumin Cuminum cyminum by gas chromatography-mass spectrometry. Chinese Journal of Analytical Chemistry. — PubMed
- Nickavar B, Abolhasani FA (2007). Screening of antioxidant properties of seven Umbelliferae fruits from Iran including cumin. Pakistan Journal of Pharmaceutical Sciences. — PubMed
- Aggarwal BB, Shishodia S (2006). Molecular targets of dietary agents for prevention and therapy of cancer (cumin included in spice review). Biochemical Pharmacology. — PubMed
PubMed Topic Searches
- PubMed: Cumin antioxidant phenolic content
- PubMed: Cumin COX inhibition
- PubMed: Cuminaldehyde radical scavenging
- PubMed: Cumin and NF-κB
- PubMed: Spices and Nrf2 pathway
Connections
- Cumin Overview
- Cumin Benefits Hub
- Cumin as Digestive Aid
- Cumin for Blood Sugar
- Cumin for Cholesterol & Weight
- Turmeric (Synergistic Anti-Inflammatory)
- Cloves (Top Phenolic Spice)
- Cinnamon
- Ginger
- Omega-3 Fatty Acids
- Vitamin E
- Vitamin C
- Rheumatoid Arthritis
- Osteoarthritis
- Anti-Inflammatory Remedies