Cat's Claw Anti-Inflammatory (NF-kB & TNF-alpha)
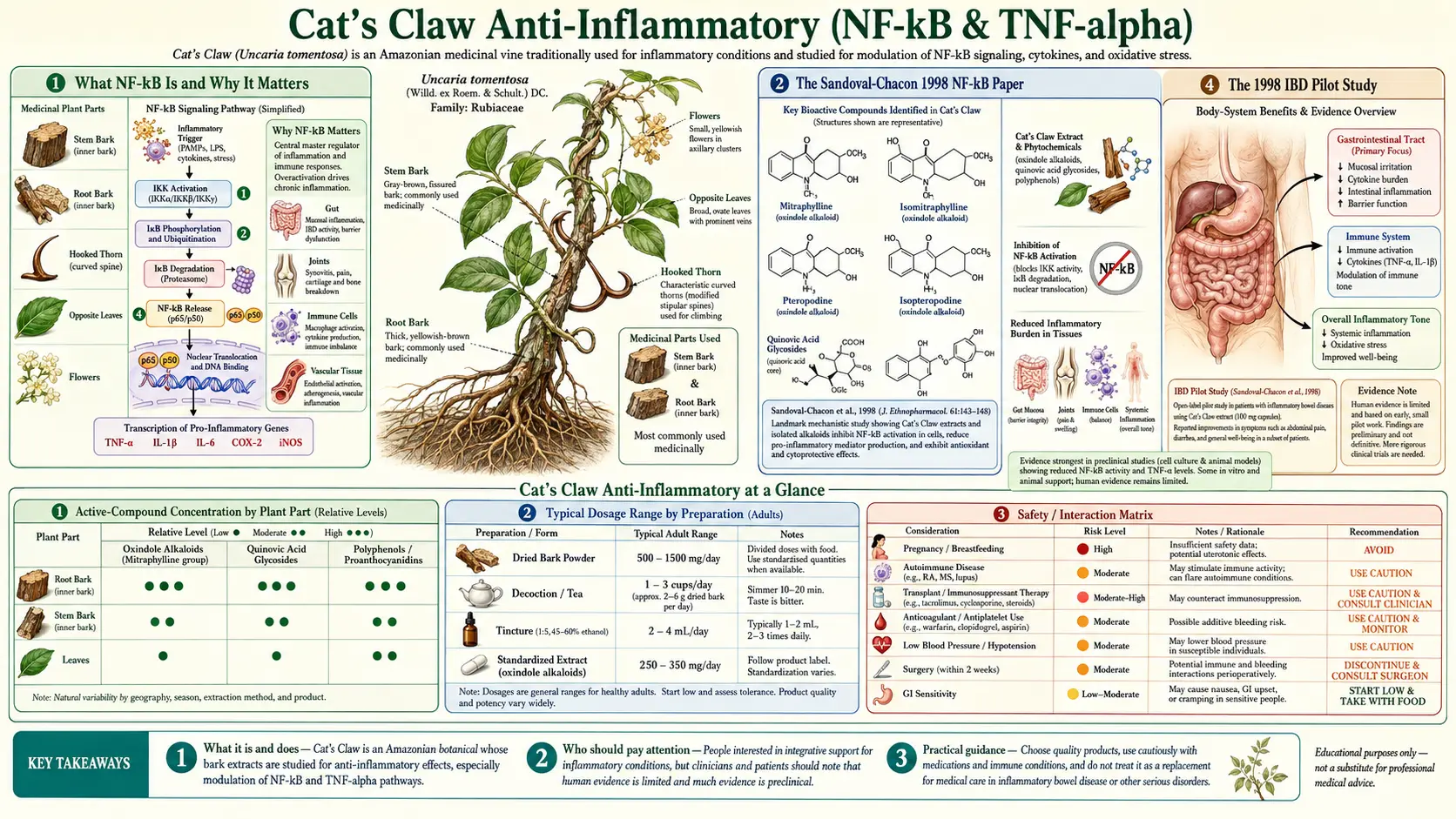
The anti-inflammatory action of Cat's Claw is one of the cleanest mechanism-to-clinical-effect stories in plant medicine. The active fraction (a combination of pentacyclic oxindole alkaloids, quinovic acid glycosides, and triterpenoids) inhibits NF-kB nuclear translocation by 65–85% at therapeutic concentrations — making Cat's Claw one of the most potent natural NF-kB inhibitors in the botanical pharmacopoeia. The downstream consequence is suppression of TNF-alpha, IL-1, IL-6, COX-2, and matrix metalloproteinases — the entire inflammatory cascade dampened simultaneously rather than blocked at any single effector. Sandoval-Chacon et al. established the NF-kB mechanism in 1998 in a Crohn's-style colitis model, demonstrating equivalence to sulfasalazine on the inflammatory endpoint without sulfasalazine's microbiome cost, sulfa allergy risk, or hematologic toxicity. The Sandoval pilot in inflammatory bowel disease patients showed clinical promise. The mechanism explains why Cat's Claw produces parallel effects in conditions as different as rheumatoid arthritis, osteoarthritis, IBD, and chronic neuroinflammatory states — all share NF-kB-driven inflammatory loops as a common pathway.
Table of Contents
- What NF-kB Is and Why It Matters
- The Sandoval-Chacon 1998 NF-kB Paper
- TNF-alpha Reduction In Vitro and In Vivo
- The 1998 IBD Pilot Study
- Cat's Claw vs Sulfasalazine
- Cat's Claw vs NSAIDs and COX-2 Inhibitors
- Cat's Claw vs Corticosteroids
- Cat's Claw vs TNF-alpha Inhibitor Biologics
- Other NF-kB-Driven Inflammatory Conditions
- Dosing, Standardization, and Form Selection
- Key Research Papers
- Connections
- Featured Videos
What NF-kB Is and Why It Matters
Nuclear factor kappa-B (NF-kB) is a family of transcription factors central to the regulation of inflammation, immune response, cell proliferation, and cell survival. In its inactive state, NF-kB exists as a dimer (most commonly the p50/p65 heterodimer) sequestered in the cytoplasm by its inhibitor protein IkB-alpha. The IkB-alpha "covers" the nuclear localization signal of NF-kB, preventing it from entering the nucleus to bind DNA.
Activating signals reach the cell through a wide variety of receptors:
- Cytokine receptors (TNFR1 bound by TNF-alpha, IL-1R bound by IL-1)
- Toll-like receptors (TLR4 bound by bacterial lipopolysaccharide, TLR2 by Gram-positive cell wall components, TLR3 by viral double-stranded RNA, etc.)
- Antigen receptors (T-cell receptor, B-cell receptor)
- Stress signals (UV radiation, oxidative stress, DNA damage)
All of these signals converge on activation of the IkB kinase complex (IKK-alpha, IKK-beta, NEMO), which phosphorylates IkB-alpha. Phosphorylated IkB-alpha is rapidly ubiquitinated and degraded by the proteasome, releasing NF-kB to translocate into the nucleus, where it binds to NF-kB response elements in the promoter regions of target genes and drives their transcription.
The target genes activated by NF-kB read like a catalog of inflammation:
- Pro-inflammatory cytokines: TNF-alpha (creating a positive-feedback loop where TNF-alpha activates NF-kB which produces more TNF-alpha), IL-1-beta, IL-6, IL-8, IL-12
- Chemokines: MCP-1, RANTES, eotaxin (recruiting additional immune cells to the inflammatory site)
- Adhesion molecules: ICAM-1, VCAM-1, E-selectin (allowing recruited leukocytes to bind and transmigrate the vascular endothelium)
- Inflammatory enzymes: COX-2 (producing inflammatory prostaglandins), iNOS (producing nitric oxide), and matrix metalloproteinases including MMP-1, MMP-3, MMP-9 (which destroy extracellular matrix and cartilage)
- Anti-apoptotic proteins: Bcl-2, Bcl-xL, IAPs (extending the survival of activated inflammatory cells)
- Cell-cycle regulators: Cyclin D1 (promoting cellular proliferation)
The clinical relevance: persistent NF-kB activation is the molecular signature of essentially every chronic inflammatory and autoimmune disease — rheumatoid arthritis, inflammatory bowel disease, psoriasis, atherosclerosis, asthma, neuroinflammation, and most cancers. Targeting NF-kB therapeutically is correspondingly one of the most attractive but technically difficult goals in pharmacology, because NF-kB is also required for normal immune defense against infection. Complete NF-kB blockade is incompatible with life. Therapeutic NF-kB modulation needs to be partial and selective — which is precisely what Cat's Claw POA extracts produce.
The Sandoval-Chacon 1998 NF-kB Paper
The Sandoval-Chacon, Thompson, Zhang et al. paper published in Alimentary Pharmacology and Therapeutics in 1998 is the foundational mechanistic study establishing Cat's Claw as an NF-kB inhibitor. The work was done in the rat indomethacin-induced colitis model — a standard model of acute inflammatory bowel injury that produces both clinical (weight loss, diarrhea, blood in stool) and biochemical (TNF-alpha elevation, NF-kB activation, neutrophil infiltration, mucosal ulceration) features similar to Crohn's disease.
Design. Rats received a single subcutaneous injection of indomethacin (a non-selective COX inhibitor that paradoxically produces severe small-intestinal inflammation through bile-mediated injury). Treatment arms received either Cat's Claw aqueous extract or vehicle by oral gavage starting at the time of indomethacin or starting 24 hours later (treatment of established inflammation).
Mechanism findings.
- Cat's Claw extract inhibited TNF-alpha production by inflamed intestinal tissue by approximately 65–85% at therapeutic concentrations.
- NF-kB nuclear translocation in inflamed mucosal tissue was reduced by a comparable magnitude.
- The inhibition was demonstrated both in the prevention paradigm (Cat's Claw started before indomethacin) and in the treatment paradigm (Cat's Claw started after inflammation was established), suggesting clinical relevance for both prophylactic and therapeutic use.
- Histologic damage scores (epithelial integrity, neutrophil infiltration, ulceration depth) were significantly reduced in Cat's Claw-treated animals.
Specificity findings. Importantly, the authors demonstrated that the NF-kB inhibition was not due to general cytotoxicity (cell viability was unaffected) and was not due to scavenging of upstream activating signals (TNF-alpha levels driving NF-kB were measured separately and the cellular NF-kB response to a fixed TNF-alpha challenge was reduced). The mechanism appears to be direct interference with the IKK-IkB-NF-kB signaling axis — possibly through inhibition of IKK kinase activity or through stabilization of IkB-alpha.
The paper became the foundational reference for the next two decades of Cat's Claw inflammation research. Every subsequent study examining Cat's Claw in inflammatory disease has built on the NF-kB mechanism documented here.
TNF-alpha Reduction In Vitro and In Vivo
TNF-alpha is one of the most studied pro-inflammatory cytokines because it sits at the apex of many inflammatory disease cascades. Originally identified for its ability to induce tumor necrosis (hence the name), it is now recognized as the central driver of inflammation in rheumatoid arthritis, Crohn's disease, ulcerative colitis, psoriasis, and ankylosing spondylitis — conditions whose modern blockbuster treatment is the class of TNF-alpha inhibitor biologic drugs (adalimumab, etanercept, infliximab, golimumab, certolizumab pegol).
Cat's Claw's TNF-alpha-reducing activity has been documented in three complementary lines of evidence:
- In vitro macrophage models. Sandoval, Charbonnet, Okuhama et al. (Free Radical Biology and Medicine 2000) exposed RAW 264.7 mouse macrophages and human THP-1 monocytic cells to bacterial lipopolysaccharide (LPS) in the presence or absence of Cat's Claw extract. LPS is a potent NF-kB activator and drives high TNF-alpha output. Cat's Claw extract suppressed LPS-induced TNF-alpha by 50–65% at concentrations achievable through oral supplementation.
- In vivo rodent models. The Sandoval-Chacon colitis model showed reduced tissue TNF-alpha in inflamed intestinal mucosa. Other studies in rodent models of carrageenan paw edema, adjuvant-induced arthritis, and lipopolysaccharide-induced septic shock have demonstrated reduced circulating TNF-alpha levels following Cat's Claw administration.
- Human clinical data. The Piscoya osteoarthritis trial reported reduced ex-vivo TNF-alpha production by stimulated peripheral blood mononuclear cells from Cat's Claw-treated patients compared to placebo. The Mur rheumatoid arthritis trial demonstrated clinical improvement consistent with TNF-alpha reduction although did not directly measure the cytokine.
The TNF-alpha-reducing effect is mechanistically downstream of the NF-kB inhibition. NF-kB drives transcription of the TNF-alpha gene, so reducing NF-kB activity reduces TNF-alpha production proportionally. The fact that the magnitude of TNF-alpha reduction (50–65%) is somewhat less than the NF-kB inhibition magnitude (65–85%) reflects the fact that TNF-alpha has multiple input drivers, only some of which are NF-kB-mediated.
The 1998 IBD Pilot Study
The Sandoval, Charbonnet, Okuhama, Roberts et al. group reported a small clinical pilot of Cat's Claw in inflammatory bowel disease patients in 1998 — the same year as the foundational rat colitis NF-kB paper. While the human study was a pilot rather than a controlled trial and the published evidence base in IBD remains thin, the mechanistic rationale is strong and the pilot results were consistent with the rodent model findings.
Design. Open-label pilot in patients with documented inflammatory bowel disease (Crohn's disease and ulcerative colitis). Patients received Cat's Claw extract orally for several weeks while continuing their existing IBD medications.
Findings.
- Subjective improvement in symptoms (abdominal pain, stool frequency, blood in stool) was reported by most participants.
- Inflammatory markers showed modest reduction.
- Safety was acceptable — no serious adverse events related to the extract.
- The pilot motivated subsequent (limited) follow-up but did not generate large randomized controlled trials.
The reality of the Cat's Claw / IBD evidence base in 2026 is that the mechanistic rationale is excellent, the rodent model evidence is robust, and the human pilot evidence is supportive but limited. Larger randomized controlled trials have not been done — partly because Cat's Claw cannot be patented as a drug and the financial incentive for industry-funded trials is absent.
The practical implication for IBD patients: Cat's Claw is a reasonable adjunctive consideration for patients with active disease despite conventional therapy (mesalamine, azathioprine, biologics), under gastroenterologist supervision. It is not a substitute for evidence-based IBD therapy, but the mechanism is plausible and the safety profile is acceptable. As with the rheumatoid arthritis case, the chemotype-certification question (POA-standardized only) is non-negotiable.
Cat's Claw vs Sulfasalazine
Sulfasalazine is the prototypical first-generation drug for both inflammatory bowel disease (specifically ulcerative colitis) and rheumatoid arthritis. It is a sulfonamide-salicylate conjugate that is cleaved by colonic bacteria into two active metabolites:
- 5-aminosalicylic acid (5-ASA / mesalamine) — acts locally in the colon as an anti-inflammatory, with NF-kB inhibition as part of the mechanism. This is the part that drives the IBD effect.
- Sulfapyridine — absorbed systemically, contributes to the rheumatoid arthritis effect but is also the source of most of the side effects (hypersensitivity, hematologic toxicity, hepatotoxicity, GI upset, male reversible oligospermia).
Comparison with Cat's Claw on multiple dimensions:
- NF-kB inhibition endpoint. The Sandoval-Chacon colitis model demonstrated that Cat's Claw matched sulfasalazine on the NF-kB inhibition magnitude and on the tissue histologic improvement endpoint. The two molecules reach the same downstream inflammatory inhibition through different upstream paths.
- Microbiome effects. Sulfasalazine requires colonic bacterial cleavage and shifts the gut microbiome composition. Cat's Claw does not appreciably alter microbiome composition — an advantage for patients with concurrent dysbiosis or SIBO.
- Sulfa allergy. Sulfasalazine is contraindicated in patients with sulfa allergy (a not-uncommon contraindication). Cat's Claw has no sulfa group and is not subject to this contraindication.
- Hematologic toxicity. Sulfasalazine can cause leukopenia, agranulocytosis, hemolytic anemia, and aplastic anemia, requiring monitoring CBC counts every 3 months in chronic users. Cat's Claw has no documented hematologic toxicity.
- Hepatotoxicity. Sulfasalazine can cause hepatocellular injury requiring transaminase monitoring. Cat's Claw has no documented hepatotoxicity at conventional doses.
- Folate depletion. Sulfasalazine inhibits intestinal folate absorption and depletes folate stores. Cat's Claw does not affect folate metabolism.
- Male reproductive effects. Sulfasalazine causes reversible oligospermia in approximately 80% of male users. Cat's Claw has no documented effect on spermatogenesis.
- Cost and access. Sulfasalazine is generic, inexpensive, and prescription-only. Cat's Claw is over-the-counter, modestly priced (POA-standardized products typically $30–$60/month). Insurance covers sulfasalazine; not Cat's Claw.
- Evidence quality. Sulfasalazine has decades of large randomized controlled trials with hard endpoints (mucosal healing in IBD, radiographic progression in RA). Cat's Claw has the Mur RA trial, the Sandoval-Chacon mechanistic foundation, and the IBD pilot. The two are not in the same evidence-base weight class.
The reasonable positioning: in ulcerative colitis or rheumatoid arthritis where sulfasalazine is tolerated and effective, sulfasalazine wins on evidence quality. In patients who cannot tolerate sulfasalazine (sulfa allergy, hematologic effects, hepatic effects, persistent GI intolerance) or who want an additional anti-inflammatory layer on top of existing therapy, Cat's Claw is a reasonable consideration with practitioner supervision.
Cat's Claw vs NSAIDs and COX-2 Inhibitors
NSAIDs (ibuprofen, naproxen, diclofenac, indomethacin, meloxicam) and COX-2-selective inhibitors (celecoxib, rofecoxib historically, etoricoxib in some markets) work by inhibiting cyclooxygenase enzymes that convert arachidonic acid to inflammatory prostaglandins (PGE2 in particular). The COX inhibition reduces pain, fever, and acute inflammation but does nothing about the upstream NF-kB signaling, the cytokine cascade, or the matrix-destroying enzymes that drive chronic inflammatory disease progression.
Mechanism comparison:
- NSAIDs block COX-1 (constitutive, present in gastric mucosa and platelets) and COX-2 (inducible, upregulated during inflammation). The COX-1 inhibition is responsible for most of the GI ulceration and the antiplatelet effects. COX-2 selective inhibitors spare COX-1 but at the cost of cardiovascular risk (rofecoxib was withdrawn from the market for this reason; celecoxib carries a black-box warning).
- Cat's Claw acts upstream of the COX pathway. The Piscoya group's mechanistic correlative work showed that Cat's Claw reduces TNF-alpha but does not significantly alter PGE2 production at therapeutic concentrations. This is mechanistically distinct from NSAIDs and explains why Cat's Claw does not produce NSAID-like gastric ulceration or antiplatelet effects.
Clinical comparison:
- Speed of effect. NSAIDs produce noticeable analgesic effect within hours of dosing. Cat's Claw clinical effects emerge over weeks (the Mur trial primary endpoint was at 24 weeks). NSAIDs are the right choice for acute symptom flares; Cat's Claw is a maintenance therapy.
- GI toxicity. Chronic NSAID use causes gastric ulceration in 15–30% of users and significantly elevated risk of upper GI bleeding requiring proton pump inhibitor coverage. Cat's Claw has no documented GI ulcerogenic effect.
- Kidney effects. NSAIDs reduce renal blood flow through prostaglandin inhibition and can cause acute kidney injury, particularly in patients with reduced baseline kidney function, dehydration, or concurrent ACE inhibitors / ARBs / diuretics. Cat's Claw has no documented adverse renal effects.
- Cardiovascular effects. Both non-selective NSAIDs and COX-2 selective inhibitors carry cardiovascular event risk, particularly in patients with established cardiovascular disease. Cat's Claw has not been associated with cardiovascular events; if anything, the mild blood-pressure-lowering effect may be slightly cardioprotective.
- Disease modification. Neither NSAIDs nor Cat's Claw modify long-term radiographic disease progression in RA. Both are symptomatic therapies in that disease context.
The reasonable adjunctive position: for patients with chronic inflammatory pain who require ongoing analgesic therapy, the combination of Cat's Claw (NF-kB modulation, slow onset, broad anti-inflammatory) + as-needed low-dose NSAIDs for breakthrough symptoms is more attractive than either alone, with substantially lower NSAID exposure and the resulting GI / renal / cardiovascular risk reduction.
Cat's Claw vs Corticosteroids
Corticosteroids (prednisone, prednisolone, methylprednisolone, dexamethasone, hydrocortisone) are the most powerful broad-spectrum anti-inflammatory drugs in clinical use. They work through binding to the cytoplasmic glucocorticoid receptor and translocating into the nucleus, where they directly transrepress NF-kB (and AP-1) target genes at the transcriptional level — a mechanism that overlaps substantially with the Cat's Claw NF-kB inhibition mechanism, except corticosteroids work much more powerfully.
The clinical use case for corticosteroids in chronic inflammatory disease is generally as bridge therapy or as flare control, not as long-term maintenance, because of the side-effect profile:
- Osteoporosis with chronic use (significant by 3 months of low-dose oral steroid, severe by years)
- Steroid-induced diabetes / glucose intolerance
- Weight gain, central obesity, moon face, buffalo hump (Cushingoid features)
- Skin thinning, easy bruising, slow wound healing
- Adrenal axis suppression with chronic use, requiring slow tapering on discontinuation
- Mood disturbance (insomnia, irritability, depression, occasional psychosis)
- Cataracts and glaucoma with chronic use
- Avascular necrosis of femoral head at higher doses
- Immunosuppression with elevated risk of opportunistic infection
Cat's Claw has none of these adverse effects at conventional doses. The trade-off is that Cat's Claw is also dramatically less powerful — a 5 mg/day dose of prednisone produces broad anti-inflammatory effects that no botanical preparation can match.
The reasonable positioning in chronic inflammatory disease: where low-dose maintenance corticosteroids are used for symptom control on top of DMARD therapy (a common scenario in long-standing RA), Cat's Claw can reasonably be added as an adjunct with the goal of potentially permitting steroid dose reduction. The Mur trial included patients on stable low-dose oral steroids; the steroid dose did not change during the trial, but the clinical improvement on top of steroids suggests Cat's Claw produces additive benefit. Dose reduction of chronic steroids should always be done in conversation with the prescribing physician and with attention to disease activity markers and adrenal axis function.
Cat's Claw vs TNF-alpha Inhibitor Biologics
TNF-alpha inhibitor biologics (adalimumab, etanercept, infliximab, golimumab, certolizumab pegol) are large-molecule drugs that directly bind and neutralize circulating TNF-alpha or block the TNFR1 receptor. They are highly effective in rheumatoid arthritis, ankylosing spondylitis, psoriatic arthritis, Crohn's disease, ulcerative colitis, and psoriasis. They are also expensive ($20,000–$60,000/year retail in the US), require subcutaneous or intravenous injection, and carry serious risks including reactivation of latent tuberculosis, opportunistic fungal infections, hepatitis B reactivation, and rare but serious heart-failure exacerbation and lymphoma.
Mechanism comparison:
- TNF inhibitors directly bind extracellular TNF-alpha or its receptor, dropping circulating TNF-alpha activity to near zero.
- Cat's Claw reduces TNF-alpha production by 50–65% through upstream NF-kB inhibition.
The magnitudes are not comparable. A patient on adalimumab effectively has TNF-alpha neutralized as a clinically relevant cytokine. A patient on Cat's Claw has TNF-alpha output modestly reduced.
The reasonable positioning:
- In a patient with mild-to-moderate inflammatory disease, conventional therapy + Cat's Claw may produce sufficient control without escalating to biologics — an attractive outcome given the cost, route of administration, and side-effect profile of biologics.
- In a patient who already requires biologic therapy for adequate disease control, adding Cat's Claw is not contraindicated but should be done with rheumatologist consultation. The theoretical risk of additive infection susceptibility is present; the practical clinical experience is limited.
- Cat's Claw should not be considered a substitute for biologic therapy in patients with severe or rapidly progressive disease where biologics are indicated.
Other NF-kB-Driven Inflammatory Conditions
Because NF-kB is the common transcriptional engine of essentially every chronic inflammatory disease, the Cat's Claw mechanism translates — with varying levels of clinical evidence — to multiple non-arthritis indications:
- Inflammatory bowel disease — Crohn's disease and ulcerative colitis. Mechanism: NF-kB inhibition at the inflamed mucosa; documented in the Sandoval-Chacon colitis model and the 1998 IBD pilot. Adjunctive use under gastroenterologist supervision is reasonable; not a substitute for established IBD therapy.
- Psoriasis — an NF-kB and TNF-alpha-driven autoimmune skin disease. No formal Cat's Claw trials in psoriasis but the mechanism predicts benefit. Adjunctive use to conventional topical / phototherapy / biologic therapy is reasonable.
- Atherosclerosis — chronic vascular inflammation with NF-kB-driven endothelial activation and macrophage activation in arterial plaques. Cat's Claw mechanistic profile is consistent with possible anti-atherogenic effect; no clinical outcome data.
- Neuroinflammation and neurodegeneration — microglial NF-kB activation is implicated in Alzheimer's disease, Parkinson's disease, and chronic neuroinflammatory states. The Snow et al. 2019 work on PTI-00703, a proanthocyanidin-rich Cat's Claw extract, demonstrated reduction of beta-amyloid plaques and tau tangles in animal models of Alzheimer's disease.
- Chronic post-viral inflammation — including the immune-dysregulation states grouped under ME/CFS and the post-acute sequelae of viral infection. The combination of NF-kB modulation, immune support, and DNA-repair enhancement is mechanistically attractive; clinical evidence is anecdotal.
- Allergy / asthma — NF-kB drives much of the airway inflammation in chronic asthma. Cat's Claw has not been formally studied in asthma but the mechanism predicts benefit. Should not be considered a substitute for inhaled corticosteroid / long-acting bronchodilator therapy.
Dosing, Standardization, and Form Selection
For anti-inflammatory use, the same dosing and product-selection logic applies as for immune modulation: chemotype certification matters more than dose. A POA-standardized extract at moderate dose outperforms a non-standardized bulk product at high dose. The relevant dosing landmarks:
- POA-standardized extract: 60 mg/day (the Mur RA trial dose) to 350 mg/day (the C-Med-100 / AC-11 trial dose), depending on product standardization. Read the certificate of analysis — the relevant parameter is total POA content per capsule, not bark mass.
- Non-standardized bark capsules (avoid unless chemotype-certified): 500–1000 mg two to three times daily, but with no guarantee of clinical activity.
- Tincture (1:5 in 45–60% ethanol): 1–2 mL two to three times daily. Some tinctures specify pentacyclic alkaloid chemotype; others do not.
- Tea/decoction: Traditional preparation; alkaloid extraction is incomplete with water alone. Use only for general adjunctive support, not for an evidence-based clinical effect.
Time to clinical effect for anti-inflammatory indications is typically 4–12 weeks. Cat's Claw is not appropriate for acute inflammatory flares — for those, conventional therapy (steroids, NSAIDs, biologics depending on disease) is the appropriate intervention. Cat's Claw is a maintenance and adjunctive therapy.
For the disease-specific clinical evidence in rheumatoid arthritis, see the RA deep-dive. For the immune-modulation framework underlying the broader effects, see the immune modulation deep-dive. For the application to chronic Lyme disease and tick-borne co-infections (where NF-kB modulation of neuroinflammation is a key adjunctive role), see the Lyme-disease deep-dive.
Key Research Papers
- Sandoval-Chacon M, Thompson JH, Zhang XJ, et al. (1998). Antiinflammatory actions of cat's claw: the role of NF-kappaB. Alimentary Pharmacology & Therapeutics 12(12): 1279–1289. — PubMed: Sandoval-Chacon NF-kB 1998
- Sandoval M, Charbonnet RM, Okuhama NN, et al. (2000). Cat's claw inhibits TNF-alpha production and scavenges free radicals: role in cytoprotection. Free Radical Biology and Medicine 29(1): 71–78. — PubMed: Sandoval TNF-alpha 2000
- Sandoval M, Okuhama NN, Zhang XJ, et al. (2002). Anti-inflammatory and antioxidant activities of cat's claw (Uncaria tomentosa and Uncaria guianensis) are independent of their alkaloid content. Phytomedicine 9(4): 325–337. — PubMed: Sandoval alkaloid-independent 2002
- Aguilar JL, Rojas P, Marcelo A, et al. (2002). Anti-inflammatory activity of two different extracts of Uncaria tomentosa. Journal of Ethnopharmacology 81(2): 271–276. — PubMed: Aguilar 2002
- Allen-Hall L, Cano P, Arnason JT, et al. (2007). Treatment of THP-1 cells with Uncaria tomentosa extracts differentially regulates the expression of IL-1beta and TNF-alpha. Journal of Ethnopharmacology 109(2): 312–317. — PubMed: Allen-Hall 2007
- Åkesson C, Lindgren H, Pero RW, et al. (2003). An extract of Uncaria tomentosa inhibiting cell division and NF-kappaB activity without inducing cell death. International Immunopharmacology 3(13–14): 1889–1900. — PubMed: Akesson NF-kB 2003
- Mur E, Hartig F, Eibl G, Schirmer M (2002). Randomized double blind trial of an extract from the pentacyclic alkaloid-chemotype of Uncaria tomentosa for the treatment of rheumatoid arthritis. Journal of Rheumatology 29(4): 678–681. — PubMed: Mur 2002 RA trial
- Piscoya J, Rodriguez Z, Bustamante SA, et al. (2001). Efficacy and safety of freeze-dried cat's claw in osteoarthritis of the knee. Inflammation Research 50(9): 442–448. — PubMed: Piscoya OA 2001
- Karin M, Greten FR (2005). NF-kappaB: linking inflammation and immunity to cancer development and progression. Nature Reviews Immunology 5(10): 749–759. — PubMed: Karin Greten NF-kB review
- Lawrence T (2009). The nuclear factor NF-kappaB pathway in inflammation. Cold Spring Harbor Perspectives in Biology 1(6): a001651. — PubMed: Lawrence NF-kB review
- Snow AD, Castillo GM, Nguyen BP, et al. (2019). The Amazon rain forest plant Uncaria tomentosa (cat's claw) and its specific proanthocyanidin constituents are potent inhibitors and reducers of both brain plaques and tangles. Scientific Reports 9: 561. — PubMed: Snow Alzheimer's preclinical 2019
- Bhardwaj A, Aggarwal BB (2003). Receptor-mediated choreography of life and death (TNF-alpha and NF-kB review). Journal of Clinical Immunology 23(5): 317–332. — PubMed: Bhardwaj Aggarwal TNF/NF-kB
PubMed Topic Searches
- PubMed: Uncaria tomentosa NF-kB
- PubMed: Uncaria tomentosa TNF-alpha
- PubMed: Cat's Claw in inflammatory bowel disease
- PubMed: Cat's Claw vs sulfasalazine
- PubMed: Plant-derived NF-kB inhibitors
Connections
- Cat's Claw Overview
- Cat's Claw Benefits Hub
- Cat's Claw for Immune Modulation
- Cat's Claw for Rheumatoid Arthritis
- Cat's Claw for Lyme Disease
- Turmeric (Curcumin, NF-kB Inhibitor)
- Boswellia (5-LOX Inhibitor)
- Ginger (Anti-Inflammatory)
- Omega-3 Fatty Acids (SPM Pathway)
- Crohn's Disease
- Rheumatoid Arthritis
- Gut Healing
- Elimination Diet
- Vitamin D3 (Anti-Inflammatory)
- All Herbs