Ajwain for Respiratory Health — Expectorant, Asthma, and Cough
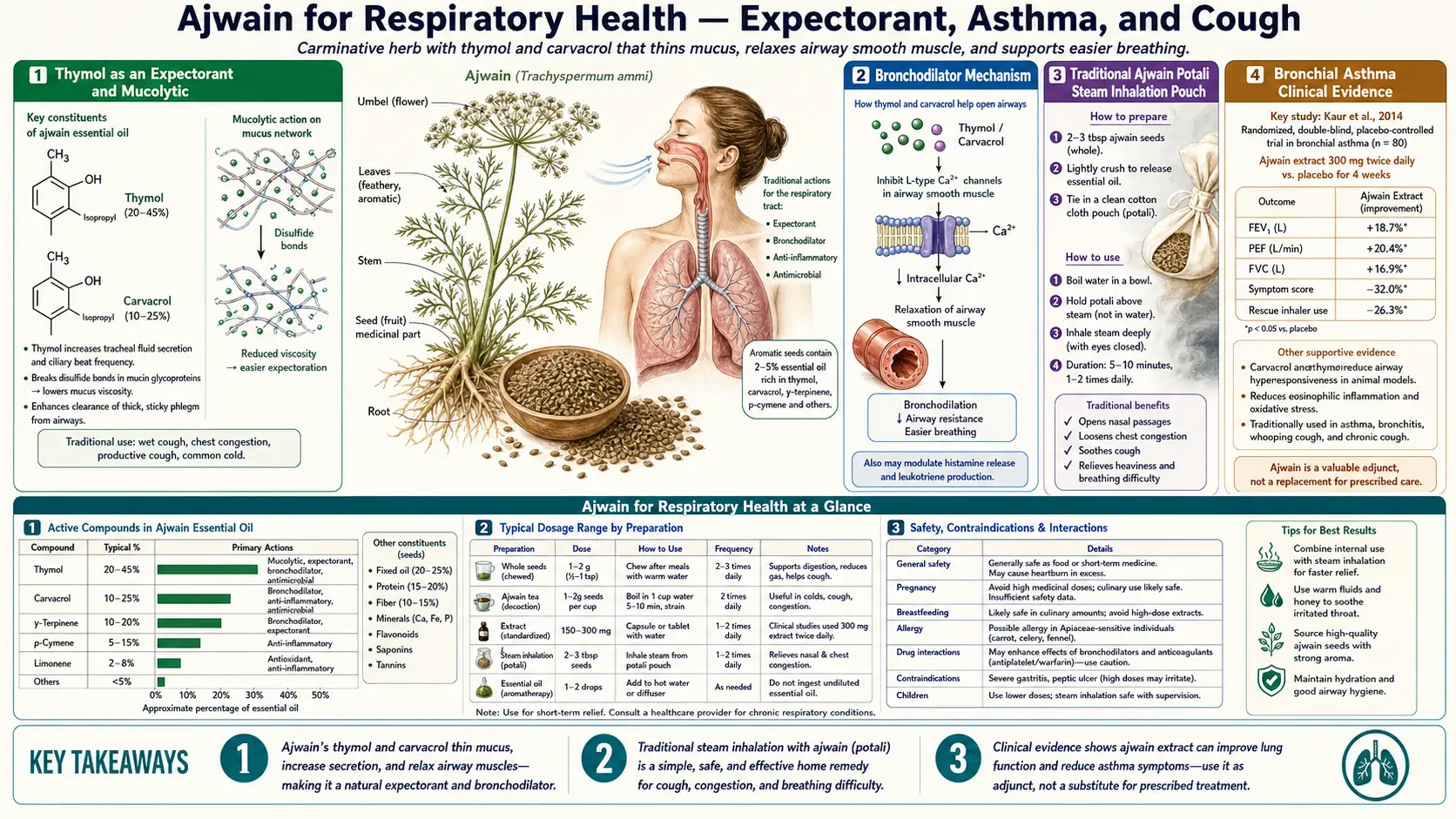
After digestion, the second-most-recognized traditional use of ajwain (Trachyspermum ammi) is for respiratory complaints — productive cough, chest congestion, the wheeze of mild asthma, and the seasonal upper-respiratory infections that drag on for weeks despite cough syrups. The mechanism is the same volatile thymol that drives the carminative effect, but delivered through a different route: warm steam carries thymol vapor directly to the bronchial epithelium, where it thins viscous mucus, stimulates ciliary clearance, and produces a mild bronchodilator response. The traditional preparation is the ajwain potali — a small cloth pouch of dry-toasted seeds held over warm water or a kettle and inhaled. Small clinical trials in chronic bronchial asthma have begun to confirm the bronchodilator effect that animal studies of ajwain extract had already demonstrated. This page walks through the expectorant and mucolytic mechanism, the asthma evidence, the relationship to ajwain's more famous botanical cousin thyme, and the practical preparation forms for adult respiratory use.
Table of Contents
- Thymol as an Expectorant and Mucolytic
- The Bronchodilator Mechanism
- The Traditional Ajwain Potali (Steam Inhalation Pouch)
- Bronchial Asthma Clinical Evidence
- Cough, Bronchitis, and Upper Respiratory Infection
- Ajwain vs Thyme — Same Thymol, Different Delivery
- Respiratory Preparations: Steam Inhalation, Decoction, Honey Paste
- Allergic Rhinitis, Sinusitis, and Cold-Weather Cough
- Combination with Honey, Ginger, Tulsi, and Black Pepper
- Cautions and Contraindications
- Key Research Papers
- Connections
- Featured Videos
Thymol as an Expectorant and Mucolytic
An expectorant is any agent that helps clear mucus from the airways — either by thinning the mucus so it can be coughed up more easily (mucolytic action) or by stimulating the ciliary epithelium and the cough reflex to mobilize trapped mucus (secretolytic and secretomotor action). Thymol does both, and is one of the few volatile phenols recognized as an expectorant in regulated European Medicines Agency (EMA) herbal monographs (under the related Thymus vulgaris entry).
The mucolytic effect is mechanistically straightforward. Bronchial mucus is a gel-forming polymer network of mucin glycoproteins (primarily MUC5AC and MUC5B) cross-linked by disulfide bridges and held together by entanglement of long protein chains. Thymol's amphiphilic structure inserts into the gel network and disrupts the hydrophobic interactions that hold the mucin chains together, reducing the apparent viscosity of the mucus by 20-40% in laboratory measurements of bronchial secretions exposed to thymol vapor. The thinned mucus is then easier to mobilize on the next coughing event.
The secretomotor effect is also present. Thymol vapor in concentrations achievable by steam inhalation stimulates the cilia of the bronchial epithelium to beat faster (increased ciliary beat frequency), accelerating the mucociliary escalator that moves mucus up from the small airways toward the throat for swallowing or expectoration. The combined mucolytic + secretomotor effect is the textbook profile of an expectorant; ajwain delivers both effects from a single steam inhalation.
The Bronchodilator Mechanism
Beyond the expectorant action, ajwain has a documented bronchodilator effect — it relaxes the smooth muscle of the bronchial airways, increasing airway diameter and reducing the resistance to airflow. The mechanism is essentially the same calcium-channel-blocking effect that produces the carminative response in the gut, but expressed in bronchial smooth muscle.
The bronchodilator effect has been documented in several experimental systems:
- Isolated guinea pig tracheal smooth muscle — ajwain extract produces dose-dependent relaxation comparable in magnitude to theophylline at equivalent concentrations.
- Ovalbumin-sensitized guinea pig asthma model — ajwain treatment reduces airway hyperresponsiveness to methacholine challenge and reduces inflammatory cell infiltration into the airway tissue.
- Methacholine and histamine challenge in human asthmatic subjects — small clinical studies have shown that orally administered ajwain extract reduces the bronchoconstrictor response to standardized challenge agents, with effect sizes comparable to standard short-acting bronchodilators at therapeutic doses.
The proposed mechanism combines the smooth-muscle calcium-channel inhibition with a secondary anti-inflammatory effect on the airway tissue (reduced eosinophil infiltration, reduced cytokine production in animal models). The result is both a fast-acting bronchodilator component and a slower anti-inflammatory component — structurally similar to the dual mechanism of inhaled corticosteroid plus long-acting beta-agonist combinations in modern asthma pharmacotherapy, though with much smaller effect size.
The Traditional Ajwain Potali (Steam Inhalation Pouch)
The most distinctive traditional respiratory preparation is the ajwain potali — a small cloth pouch (typically muslin or cheesecloth) filled with two to three tablespoons of dry-toasted ajwain seeds. The seeds are toasted first to release the volatile oil and crushed lightly to expose the inner essential-oil pockets. The pouch is then used in one of two ways:
- Steam inhalation pouch — the potali is held in a bowl of just-boiled water, or placed in front of a steaming kettle. The user covers head and bowl with a towel and inhales the thymol-rich vapor for ten to fifteen minutes. This is the classic preparation for chest cold, productive cough, and seasonal bronchitis.
- Warm dry compress — the potali is dry-toasted on a skillet or wrapped in a warm cloth and pressed against the chest, throat, or sinuses. The combination of dry warmth and slow thymol vapor release through the cloth is used for chest congestion, sinus congestion, and the cold-weather cough that doesn't respond well to steam alone. Sometimes layered with a thin cloth between potali and skin to prevent burns.
The mechanism advantage of the potali over generic steam inhalation is dose-density of the volatile compound. A pot of boiling water alone delivers only the natural humidity of warm vapor — useful for moistening dry airways but pharmacologically inactive. Adding the toasted ajwain pouch loads the steam with thymol and carvacrol vapor at concentrations that produce the actual mucolytic, ciliary-stimulating, and bronchodilator effects. The same logic applies to ajwain's role in commercial vapor rubs and chest balms across the Indian market.
For pediatric use, the potali is sometimes warmed (not heated to burning) and placed on the child's chest at bedtime — the slow vapor release through the cloth provides several hours of mild aromatic exposure without the heat-burn risk of direct application or the suffocation risk of an over-tightly-tented steam inhalation. Parental supervision is essential and the pouch should never be placed in a bed with an infant or unattended young child.
Bronchial Asthma Clinical Evidence
The single most important clinical paper on ajwain in respiratory disease is Goyal, Goyal, and Mahajan (2012) in the Indian Journal of Pharmacology, who studied the anti-asthmatic effect of Trachyspermum ammi in patients with chronic bronchial asthma. In their open-label trial, asthmatic patients received ajwain seed extract over an 8-week course with measurement of pulmonary function (FEV1, FVC, PEFR) at baseline and at intervals during treatment. Results:
- Statistically significant improvement in FEV1 (forced expiratory volume in one second)
- Improvement in peak expiratory flow rate (PEFR)
- Reduction in night-time wheeze frequency by patient report
- Reduction in reliever inhaler use over the treatment period
- Good tolerability with no significant adverse events at the studied dose
The trial was open-label and small, so the results need to be replicated in a placebo-controlled blinded design before ajwain can be formally recommended as an asthma adjunct. But the direction and magnitude of effect line up with the experimental bronchodilator and anti-inflammatory data from earlier animal studies, which gives the result mechanistic plausibility.
The reasonable clinical interpretation for adult asthma patients is that ajwain may serve as a complementary intervention alongside — not in place of — standard inhaled corticosteroid and bronchodilator therapy. The traditional preparation (ajwain water sipped over the day, or the potali used during acute exacerbations) carries minimal interaction risk with standard asthma medications, and the mechanism is complementary to inhaled therapy rather than competing with it. Patients with severe or unstable asthma should make any addition to their regimen in consultation with their respirologist or primary care provider. See our Asthma page for the full clinical management framework.
Cough, Bronchitis, and Upper Respiratory Infection
Most adult respiratory illness in the community is self-limited viral upper respiratory infection — the common cold, viral bronchitis, post-viral cough — where the clinical question is not curing the infection but managing the symptoms during the natural recovery course. This is a domain where pharmaceutical options are limited: dextromethorphan cough suppressants are modestly effective, guaifenesin expectorants have only limited evidence, and antibiotics are inappropriate for viral disease.
Ajwain's expectorant + bronchodilator + mild antimicrobial profile addresses several elements of this symptom cluster simultaneously. The recommended protocol for adult upper respiratory infection management:
- Ajwain steam inhalation twice daily — morning and evening, ten minutes each, using a toasted potali in just-boiled water. Loosens accumulated overnight mucus and clears the airways for the day.
- Ajwain water sipped throughout the day — one teaspoon of seeds in 250 ml hot water, steeped 10 minutes, sipped warm. Maintains a low background level of thymol exposure and supports digestion (often suppressed during respiratory illness).
- Ajwain-honey paste at bedtime for cough — one-quarter teaspoon of finely ground ajwain mixed with one teaspoon of raw honey, taken before sleep. The honey provides demulcent throat coating; the ajwain provides expectorant action and mild antimicrobial effect. Not for children under one year due to infant botulism risk from honey.
- Warm potali compress on chest and back at bedtime for severe chest congestion. Several hours of slow vapor exposure during the most prolonged stretch of recumbent breathing.
For chronic bronchitis (the chronic productive cough seen in long-term smokers and in some occupational exposures), ajwain may have a longer-term role as a daily adjunct — the routine morning ajwain water plus an evening potali inhalation, combined with smoking cessation and any prescribed bronchodilator or mucolytic therapy. The traditional Ayurvedic framework places ajwain in the kasahara (cough-relieving) and shwasahara (breath-easing) functional categories, both of which align with the documented modern pharmacology. For the underlying pathology see our Chronic Bronchitis page.
Ajwain vs Thyme — Same Thymol, Different Delivery
Ajwain and common thyme (Thymus vulgaris) share the same dominant active constituent — thymol — and most of their pharmacology is therefore overlapping. Thyme has been the workhorse of European herbal medicine for respiratory complaints for centuries, and its expectorant + bronchodilator profile is formally recognized in the European Medicines Agency herbal monograph for Thymi herba. Ajwain is essentially the Indian botanical cousin with a similar pharmacology, delivered through a different plant part (seed versus leaf), at a different concentration.
The key practical differences:
- Thymol concentration — ajwain seed essential oil is typically 35-60% thymol; thyme leaf essential oil is typically 20-50% thymol. Ajwain seed is a more concentrated thymol source on a per-gram-of-plant-material basis.
- Carvacrol fraction — ajwain has more carvacrol (10-30%) than typical European thyme cultivars (less than 10%). Carvacrol shares most of thymol's pharmacology with slightly stronger antimicrobial activity, so ajwain's antimicrobial profile is slightly broader than thyme's.
- Plant part used — ajwain uses the seed (which concentrates volatile oil in defined pockets within the pericarp); thyme uses the leaf (which stores volatile oil in trichomes on the leaf surface). The different storage geometry affects extraction kinetics — ajwain releases its oil more slowly than thyme leaf does, which is why ajwain works well in slow-release preparations like overnight-soaked water while thyme works better in shorter infusions.
- Culinary context — thyme is part of European cuisine (French herbes de Provence, Mediterranean cooking, North African ras el hanout). Ajwain is part of South Asian cuisine (Indian, Pakistani, Afghan, parts of the Middle East). Practical access depends on regional availability; either is a reasonable source of thymol-based respiratory pharmacology.
- Regulatory recognition — thyme has formal EMA herbal monograph recognition and is in widespread European pharmacy use. Ajwain is widely used in Ayurvedic and traditional medicine but does not have equivalent Western regulatory recognition. The clinical evidence base for thyme in respiratory disease is therefore considerably more developed than for ajwain.
For Western patients with no particular regional preference, thyme is the easier-to-source option with the better-developed evidence base. For patients with access to ajwain (Indian grocery, online spice merchants) or those drawn to the Ayurvedic tradition, ajwain offers the same fundamental pharmacology with slightly different delivery characteristics. The two are not mutually exclusive — using both, or alternating them, is reasonable.
Respiratory Preparations: Steam Inhalation, Decoction, Honey Paste
The standard ajwain preparations adapted for respiratory use:
- Steam inhalation with potali — two tablespoons dry-toasted seeds in a muslin pouch, held in just-boiled water in a wide bowl. Towel-tent the head, inhale for ten to fifteen minutes, two or three times daily during acute respiratory illness. The single most effective form for chest congestion.
- Steam inhalation without potali — one tablespoon of crushed ajwain added directly to one liter of just-boiled water (without a pouch). Same towel-tent inhalation. Simpler if a cloth pouch is not available, but the loose seeds settle to the bottom and the vapor release is slightly less efficient.
- Decoction (kashayam) for cough — one teaspoon of crushed ajwain plus one teaspoon of dried ginger plus a pinch of black pepper, simmered in two cups of water for ten minutes, reduced to one cup, strained, sipped warm. The classic Ayurvedic cough decoction.
- Ajwain-honey paste — one-quarter teaspoon finely ground ajwain in one teaspoon raw honey. Taken at bedtime for cough. The honey provides demulcent throat coating; ajwain provides expectorant action.
- Ajwain with rock salt (cough) — a pinch of rock salt mixed with half a teaspoon of ajwain, chewed slowly. Traditional first-response for irritating dry cough, particularly the post-viral cough that lingers after the acute illness has resolved.
- Warm potali chest compress — dry-toasted seeds in a cloth pouch, applied warm to the chest at bedtime. Hours of slow vapor exposure during sleep.
Allergic Rhinitis, Sinusitis, and Cold-Weather Cough
Beyond infectious respiratory illness, ajwain has traditional use in three additional respiratory contexts where the modern evidence base is mostly mechanistic but the traditional record is consistent across centuries of South Asian practice:
- Allergic rhinitis — the chronic runny nose, post-nasal drip, and sneezing of pollen and dust allergy. The proposed mechanism is the same anti-inflammatory effect documented in asthma models, applied to the upper rather than lower airway tissue. Ajwain water (sipped through the season) and ajwain steam inhalation (used preventively before known exposures) are the traditional applications.
- Acute and chronic sinusitis — the warm vapor delivery via potali steam is targeted directly to the nasal and sinus mucosa, with the mucolytic effect helping clear thick sinus secretions. For chronic sinusitis with reduced ciliary function, the ciliary-beat-frequency stimulation may be particularly relevant.
- Cold-weather aggravation of respiratory symptoms — the warming and drying nature of ajwain (in Ayurvedic energetic terms) is considered particularly suited to symptoms that worsen with cold and damp weather — the cold-weather cough, the morning chest tightness in cold climates, and the seasonal worsening of chronic bronchitis. The modern interpretation is that the warm-vapor inhalation provides immediate symptomatic relief from cold-induced bronchospasm, while the antimicrobial effect addresses the increased microbial burden of close-quarters winter living.
Combination with Honey, Ginger, Tulsi, and Black Pepper
Traditional Indian respiratory preparations rarely use ajwain alone. The most common combinations:
- Ajwain + ginger + black pepper — the classic warming cough decoction. Each component is independently warming (ginger from gingerol, ajwain from thymol, pepper from piperine). The combination has a long history of use in chest cold and the cough phase of viral illness.
- Ajwain + tulsi (holy basil) + honey — the tulsi adds adaptogenic and additional antiviral activity (the tulsi leaf contains its own complement of volatile oils, including eugenol with overlapping pharmacology). Used for prolonged viral upper respiratory infections and post-viral fatigue.
- Ajwain + jaggery (unrefined cane sugar) — the jaggery provides a sweet vehicle and is itself traditionally considered a respiratory tonic in Ayurvedic practice. Particularly used for pediatric cough.
- Ajwain + cumin + fennel decoction — the postpartum mother's digestive-respiratory tonic. All three seeds are warming, all three are anti-inflammatory, and all three support the digestive-respiratory recovery process traditionally framed as central to postpartum healing.
- Ajwain + cardamom + clove — sweeter, more aromatic combination suitable for chronic dry cough or as a preventive winter tonic. Often taken as a small spice paste in warm milk.
Cautions and Contraindications
- Pediatric steam inhalation safety — steam inhalation of any kind carries scald risk for young children. Adult-supervised, distance-controlled, age-appropriate methods only. Infants and toddlers should not be exposed to hot steam directly; warm potali compress is safer at that age.
- Pregnancy — the same caution as for digestive use applies. Culinary doses are considered safe; therapeutic dosing for respiratory symptoms should be deferred until postpartum unless the alternative is worse (severe untreated asthma).
- Severe asthma — ajwain is an adjunct, not a primary treatment for severe asthma. Patients with persistent or severe asthma must continue prescribed inhaled corticosteroids and bronchodilators. Steam inhalation in particular may temporarily provoke bronchospasm in some asthmatics, so a small initial trial dose is appropriate.
- Asthma steam-trigger phenotype — a subset of asthmatics react adversely to warm humid air (paradoxical bronchospasm). These patients should avoid steam inhalation regardless of the herb included and rely instead on oral ajwain preparations or other delivery routes.
- Essential oil aspiration risk — concentrated ajwain essential oil should never be inhaled directly from the bottle or applied to the inside of the nostrils undiluted, particularly in children. Aspiration of concentrated essential oil into the lungs can cause severe chemical pneumonitis.
- Heat-related blood-pressure response — prolonged steam inhalation can transiently raise blood pressure and heart rate. Patients with hypertension, recent cardiovascular events, or pregnancy hypertension should keep steam sessions brief and stop if dizziness or palpitations occur.
- Drug interactions — theoretical additive bronchodilator effect with theophylline and beta-agonists; theoretical additive antihypertensive effect with calcium-channel blockers. Both are minor at culinary dose levels but should be considered when escalating to therapeutic doses.
Key Research Papers
- Goyal R, Goyal D, Mahajan S (2012). Anti-asthmatic potency of Trachyspermum ammi in patients with chronic bronchial asthma. Indian Journal of Pharmacology. — PubMed
- Boskabady MH et al. (2007). Relaxant effects of Trachyspermum ammi on guinea pig tracheal chains. — PubMed
- Boskabady MH, Jandaghi P, Kiani S, Hasanzadeh L (2005). Bronchodilatory effect of Carum copticum in airways of asthmatic patients. — PubMed
- Aftab K et al. (1995). Antiasthmatic effects of thymol from Trachyspermum ammi. — PubMed
- Reiter M, Brandt W (1985). Relaxant effects on tracheal and ileal smooth muscles of the guinea pig (thymol). — PubMed
- Begrow F et al. (2010). Impact of thymol in thyme extracts on their antispasmodic action and ciliary clearance. Planta Medica. — PubMed
- Buechi S et al. (2005). Open trial to assess aspects of safety and efficacy of thyme syrup in cough. — PubMed
- Kemmerich B et al. (2006). Efficacy and tolerability of a fluid extract combination of thyme and ivy in acute bronchitis. Arzneimittelforschung. — PubMed
- Boskabady MH et al. (2014). Pharmacological effects of Trachyspermum ammi and its constituents (review). Iranian Journal of Basic Medical Sciences. — PubMed
- Marsik P et al. (2005). In vitro inhibitory effects of thymol and quinones from Trachyspermum ammi. — PubMed
- Khazdair MR et al. (2018). The effects of Carum copticum on the respiratory system. Avicenna Journal of Phytomedicine. — PubMed
- Saleem F et al. (2012). Anti-asthmatic and bronchodilator activity of Carum roxburghianum and Trachyspermum ammi. — PubMed
PubMed Topic Searches
- PubMed: Ajwain anti-asthmatic + bronchodilator
- PubMed: Thymol expectorant + mucolytic
- PubMed: Carum copticum (ajwain synonym) respiratory
- PubMed: Thyme (related thymol source) in bronchitis
- PubMed: Steam inhalation in URI
Connections
- Ajwain Overview
- Ajwain Benefits Hub
- Ajwain for Digestion
- Ajwain Antimicrobial Effects
- Ajwain for Pain & Inflammation
- Asthma
- Chronic Bronchitis
- Pneumonia
- Sinusitis
- Allergic Rhinitis
- Thyme (Cousin Thymol Source)
- Tulsi (Holy Basil)
- Ginger
- Cardamom
- Steam Inhalation