Ajwain Antimicrobial — Thymol, Carvacrol, and the Gut Dysbiosis Adjunct
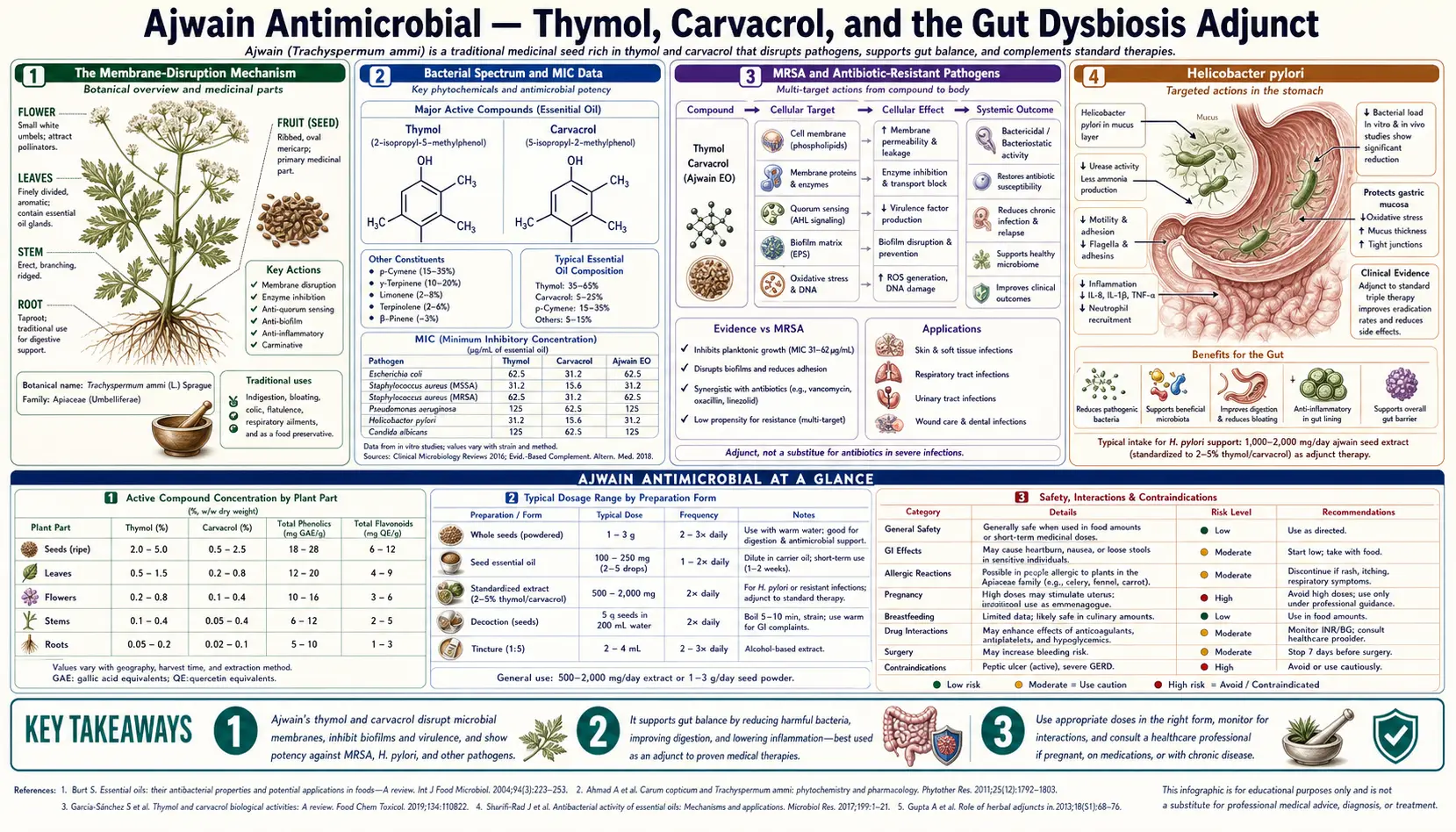
The antimicrobial profile of ajwain (Trachyspermum ammi) is the best-documented part of its pharmacology. Dozens of in vitro studies have measured minimum inhibitory concentrations (MIC) of ajwain essential oil and its isolated constituents (thymol, carvacrol, p-cymene, gamma-terpinene) against bacteria, fungi, parasites, and biofilms relevant to both food spoilage and human infection. The mechanism is consistent across pathogens: thymol and carvacrol insert into the microbial cell membrane, increase permeability, collapse the proton motive force, and kill the organism. Susceptible pathogens at clinically achievable concentrations include Escherichia coli, Staphylococcus aureus (including MRSA isolates), Salmonella, Listeria, Helicobacter pylori, and Candida albicans. The traditional culinary use of ajwain in spiced pickles and ghee preparations was almost certainly preservation-driven long before the antimicrobial mechanism was characterized; the modern research interest is in repurposing the same activity as a complementary intervention for gut dysbiosis, SIBO, and small-intestinal Candida overgrowth.
Table of Contents
- The Membrane-Disruption Mechanism
- Bacterial Spectrum and MIC Data
- MRSA and Antibiotic-Resistant Pathogens
- Helicobacter pylori
- Antifungal Activity (Candida, Dermatophytes, Molds)
- Food Preservation: The Original Antimicrobial Use
- Gut Dysbiosis, SIBO, and Candida Overgrowth Adjunct
- Oral Cavity and Dental Antimicrobial Use
- Antiparasitic and Anthelmintic Activity
- Biofilm Disruption
- Cautions: Microbiome Selectivity and Long-Term Use
- Key Research Papers
- Connections
- Featured Videos
The Membrane-Disruption Mechanism
The antimicrobial mechanism of thymol and carvacrol is one of the cleaner mechanistic stories in plant pharmacology. Both molecules are small, lipophilic, amphiphilic phenols. They partition readily into the lipid bilayer of bacterial and fungal cell membranes, where they:
- Disorganize the lipid packing — the bulky aromatic ring inserts between fatty acid tails, fluidizing the membrane and disrupting the orderly packing required for normal membrane function.
- Increase membrane permeability — the disorganized bilayer becomes leaky to ions, ATP, nucleotides, and small metabolites. Intracellular contents leak out and external materials leak in.
- Collapse the proton motive force — the electrochemical gradient across the bacterial inner membrane that powers ATP synthesis and active transport is dissipated as protons leak across the now-permeable membrane.
- Disrupt membrane-embedded enzymes — many critical bacterial enzymes (electron transport chain components, membrane-bound transporters) require the ordered lipid environment to function. The disorganized membrane impairs these enzymes directly.
- At higher concentrations, cause complete lysis — the membrane integrity is lost entirely and the cell ruptures.
The mechanism is non-specific in a useful sense: it doesn't target a single bacterial enzyme or pathway that can be bypassed by resistance mutations. The membrane itself is the target. This is the same reason why bacterial resistance to thymol and carvacrol develops more slowly than resistance to conventional antibiotics — there is no easy mutational escape from a mechanism that disrupts the lipid bilayer as a physical structure.
The same mechanism explains why thymol and carvacrol are broad-spectrum: gram-positive bacteria, gram-negative bacteria, yeasts, and filamentous fungi all have lipid membranes susceptible to the same disorganizing effect. Gram-negative bacteria are slightly less susceptible because their outer lipopolysaccharide membrane provides a partial barrier to the phenolic compound reaching the inner membrane, but the effect is dose-dependent rather than absolute.
Bacterial Spectrum and MIC Data
Published minimum inhibitory concentration (MIC) data for ajwain essential oil and its isolated constituents against common pathogens. MIC values vary considerably between studies depending on the essential-oil composition (thymol percentage varies with cultivar, geography, and harvest time) and the susceptibility-testing methodology. Approximate consensus ranges:
| Organism | Ajwain essential oil MIC (mcg/ml) | Isolated thymol MIC (mcg/ml) |
|---|---|---|
| Escherichia coli | 100-500 | 50-250 |
| Staphylococcus aureus | 50-300 | 30-150 |
| Staphylococcus aureus (MRSA isolates) | 100-400 | 60-200 |
| Salmonella species | 100-500 | 50-200 |
| Listeria monocytogenes | 50-300 | 30-150 |
| Pseudomonas aeruginosa | 500-2000 | 250-1000 |
| Helicobacter pylori | 50-200 | 25-100 |
| Candida albicans | 100-500 | 50-250 |
| Aspergillus species | 200-1000 | 100-500 |
The general pattern is that gram-positive bacteria (S. aureus, Listeria) tend to be more susceptible than gram-negative bacteria (E. coli, Salmonella, Pseudomonas), and that pathogens with naturally permeable outer membranes (H. pylori, Listeria) are particularly susceptible. Pseudomonas aeruginosa is the most resistant common pathogen due to its multilayered outer-membrane structure and active efflux pumps — ajwain is not a useful intervention for Pseudomonas infection.
The clinically achievable concentrations of thymol in the human gut after a culinary or therapeutic dose of ajwain seed are in the low end of the in-vitro MIC range. This means ajwain is unlikely to be bactericidal in the systemic circulation, but can achieve inhibitory concentrations in the gut lumen where the seed essential oil is released and where the membrane mechanism can act directly on luminal pathogens. The respiratory route via steam inhalation can also achieve locally effective concentrations on the bronchial mucosa for surface-colonizing pathogens.
MRSA and Antibiotic-Resistant Pathogens
One of the more interesting threads in modern ajwain research is the activity against antibiotic-resistant bacterial strains. Multiple published studies have measured MIC values of ajwain essential oil against methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant enterococci (VRE), and extended-spectrum beta-lactamase (ESBL)-producing Enterobacteriaceae — finding susceptibilities similar to or only modestly worse than the corresponding non-resistant strains.
The reason is the membrane mechanism. Methicillin resistance in S. aureus is driven by the altered penicillin-binding protein PBP2a, which gives resistance to beta-lactam antibiotics that target the bacterial cell wall. Thymol does not work through the cell wall; it works through the cell membrane. The PBP2a mechanism that confers methicillin resistance is irrelevant to thymol's mechanism of action, so MRSA is roughly as susceptible to thymol as is non-resistant S. aureus.
The same logic applies to many other resistance mechanisms. Beta-lactamases hydrolyze beta-lactam antibiotics — irrelevant to thymol. Vancomycin resistance changes the bacterial cell wall peptidoglycan structure — irrelevant to thymol. Efflux pump overexpression confers resistance to many antibiotics by pumping them out faster than they can act — partially relevant to thymol (efflux pumps can remove some thymol), but the membrane-disruption mechanism is so non-specific that pump-based resistance provides only partial protection.
This does not mean ajwain is a substitute for antibiotics in serious infection. The clinical context is much narrower: ajwain might serve as a complementary topical or oral preparation in mild skin and soft tissue infection, as an adjunct in food-preservation contexts, or as part of an integrative protocol for gut decolonization of MRSA carriage. Serious antibiotic-resistant infections (MRSA bacteremia, VRE endocarditis, ESBL pyelonephritis) require definitive antibiotic therapy by infectious disease specialists; ajwain is not part of that picture.
Helicobacter pylori
Helicobacter pylori is the gastric pathogen causally associated with peptic ulcer disease and gastric adenocarcinoma. Standard treatment is multi-antibiotic combination therapy (the so-called triple or quadruple therapy regimens), which is increasingly limited by rising clarithromycin and metronidazole resistance rates worldwide.
Ajwain's in vitro activity against H. pylori is reasonably well-documented. MIC values of ajwain essential oil are in the 50-200 mcg/ml range, similar to thyme essential oil and oregano essential oil. The mechanism is the same membrane disruption, and H. pylori is more susceptible than many gram-negative bacteria because of its relatively thin outer membrane.
The clinical translation has not yet been done in randomized trial form. The proposed application is as a complementary intervention either before or after standard antibiotic eradication therapy: ajwain water or ground ajwain with meals over several weeks may reduce H. pylori burden in carriers who are not yet candidates for full eradication therapy, or may support post-eradication suppression in patients with high recurrence risk. This is hypothesis-generating rather than evidence-based clinical recommendation. The relevant clinical management framework is on our Helicobacter pylori page.
The observed gastroprotective effect of ajwain in animal peptic ulcer models discussed in the Digestive Aid page may overlap mechanistically with the H. pylori activity: the same membrane-disrupting effect that suppresses the bacterium may also contribute to the mucosal protection seen in those experimental ulcer studies.
Antifungal Activity (Candida, Dermatophytes, Molds)
The antifungal activity of ajwain essential oil and thymol is broad-spectrum and well-documented. Susceptible organisms include:
- Candida albicans and other Candida species (C. tropicalis, C. krusei, C. glabrata). MIC values in the 100-500 mcg/ml range for essential oil, 50-250 mcg/ml for isolated thymol.
- Dermatophyte fungi (Trichophyton, Microsporum, Epidermophyton) responsible for ringworm, athlete's foot, and onychomycosis. Comparable MIC values to Candida.
- Aspergillus species, including A. flavus (the aflatoxin producer in food contamination) and A. niger.
- Fusarium and Penicillium species relevant to food spoilage and mycotoxin production.
- Cryptococcus neoformans, a yeast-form fungus relevant in immunocompromised hosts (though clinical translation here is purely hypothetical).
The mechanism is the same membrane disruption as for bacteria. Fungal cells have lipid membranes that thymol can insert into and disorganize. The fungal cell wall (containing chitin and beta-glucan in addition to the lipid membrane) provides some additional barrier but does not prevent the eventual membrane effect at therapeutic concentrations.
The clinical applications include traditional use of ajwain water or paste topically for fungal skin infections (the powdered seed mixed with a small amount of water or coconut oil makes a paste applied to the affected area), and oral ajwain as a complementary intervention in intestinal Candida overgrowth syndromes. For systemic invasive fungal infections, ajwain has no role — conventional antifungal therapy by infectious disease specialists is the only appropriate intervention.
Food Preservation: The Original Antimicrobial Use
The traditional culinary use of ajwain in spiced pickles, ghee preparations, and dry spice blends was preservation-driven long before refrigeration. The thymol-rich essential oil released from ajwain seeds during cooking and storage suppresses growth of food-spoilage organisms and food-borne pathogens in the prepared food, extending shelf life and reducing food-poisoning risk in tropical climates where ambient food spoilage is rapid.
Modern food-science research has documented several practical applications:
- Ground meat preservation — ajwain essential oil added at 0.1-0.5% by weight extends refrigerated shelf life of ground meat preparations and reduces growth of Salmonella, Listeria, and E. coli O157:H7 in challenge studies.
- Fresh produce washing — ajwain essential oil at low concentrations (50-200 ppm) in produce wash water reduces surface microbial load and extends refrigerated shelf life of leafy greens and fresh-cut fruits.
- Bread and baked goods — ajwain incorporated into flour for paratha, naan, and Indian flatbreads contributes to the antimicrobial spice profile that allows these breads to be stored at room temperature for hours without refrigeration in traditional household use.
- Fermented dairy — ajwain at very low concentrations (below the level that would inhibit starter cultures) extends shelf life of refrigerated yogurt and labneh preparations.
- Pickle preservation — ajwain is a traditional component of Indian achaar (oil-based pickles) where the combination of mustard oil, salt, turmeric, and ajwain creates a multi-mechanism preservation system that allows months of shelf-stable storage.
- Aflatoxin suppression in stored grains — ajwain essential oil suppresses growth of Aspergillus flavus and the subsequent aflatoxin production in stored cereals and pulses, a meaningful application in tropical-grain-storage settings where aflatoxin contamination is a chronic public health concern. See our Aflatoxin page for more context.
Gut Dysbiosis, SIBO, and Candida Overgrowth Adjunct
The contemporary clinical interest in ajwain has shifted toward its use as a complementary intervention in functional gut conditions characterized by microbial dysbiosis. The relevant clinical contexts:
- Small Intestinal Bacterial Overgrowth (SIBO) — the abnormal proliferation of colonic-type bacteria in the small intestine, presenting with bloating, gas, and altered stool. Standard treatment is the antibiotic rifaximin, often combined with herbal antimicrobial protocols that include thymol-containing herbs (oregano, thyme, ajwain) as primary or supportive agents. The relapse rate after rifaximin is high, and ajwain may serve as part of post-antibiotic suppression. See our SIBO page.
- Small Intestinal Fungal Overgrowth (SIFO) — the fungal analog of SIBO, where Candida or other fungi proliferate in the small intestine. Standard treatment is the antifungal nystatin or fluconazole. Ajwain's anti-Candida activity makes it a reasonable complementary agent, particularly for the maintenance phase.
- Intestinal Candida overgrowth syndrome — a more general category of gut dysbiosis with Candida prominence, characterized by sweet cravings, gas, bloating, brain fog, and sometimes vaginal yeast recurrences in women. The clinical entity is debated; ajwain has been used as part of empirical anti-Candida protocols.
- Post-antibiotic dysbiosis — the disrupted microbial ecosystem that follows broad-spectrum antibiotic therapy. Ajwain water taken during the post-antibiotic recovery period is the traditional Ayurvedic intervention; the modern interpretation is that ajwain's broad antimicrobial activity may help suppress opportunistic overgrowth (Candida, C. difficile in some patients) while the protective commensal flora is repopulating.
- Traveler's diarrhea prevention — the traditional use of ajwain as a digestive prophylactic in regions with high enteric pathogen exposure aligns with the documented activity against E. coli (the most common cause of traveler's diarrhea) and Salmonella.
The practical protocol in these contexts is typically ajwain water (one teaspoon of seeds soaked overnight in 200 ml water, sipped on rising) plus a small dose of toasted seeds with each main meal, continued for two to four weeks. This is integrated with standard medical treatment of the underlying condition, not used as a substitute.
Oral Cavity and Dental Antimicrobial Use
The thymol in ajwain is the same molecule that gives the antiseptic mouthwash Listerine its core antimicrobial activity (Listerine's formula combines thymol with eucalyptol, methyl salicylate, and menthol). Ajwain has analogous traditional use for oral antimicrobial purposes:
- Chewing toasted ajwain as a traditional alternative to commercial breath fresheners. The thymol reduces oral bacterial load including the anaerobes that produce volatile sulfur compounds (the molecular basis of bad breath).
- Ajwain water as oral rinse for mild gingivitis, post-extraction socket care, and oral aphthous ulcers. Cool ajwain water held in the mouth for thirty seconds and either swallowed or spat out, two or three times daily.
- Ajwain paste for toothache — traditional first-line household analgesic for toothache, where the thymol provides both antimicrobial activity and a mild local anesthetic effect on the inflamed pulp and gum tissue. Not a substitute for definitive dental treatment.
- Oral candidiasis (thrush) — the anti-Candida activity of ajwain extends to the oral cavity. Used adjunctively in adult thrush in immunocompetent patients; standard antifungal therapy remains primary in immunocompromised hosts.
Antiparasitic and Anthelmintic Activity
Traditional Ayurvedic medicine classifies ajwain as a krimi-ghna (worm-killing) herb. Modern research has documented in vitro activity against several parasitic organisms:
- Ascaris lumbricoides (intestinal roundworm) — ajwain essential oil immobilizes and kills adult worms in laboratory exposure studies.
- Hookworm species — similar laboratory activity documented.
- Giardia lamblia — the protozoan cause of giardiasis is susceptible to ajwain essential oil in vitro.
- Entamoeba histolytica — in vitro activity against the protozoan cause of amebic dysentery.
- Trichomonas vaginalis — in vitro susceptibility documented.
The clinical translation is limited. For confirmed parasitic infection, conventional antiparasitic therapy (albendazole, mebendazole, metronidazole, tinidazole) is far better characterized and more reliably effective. Ajwain may have a complementary role in suppressing subclinical parasitic burden or supporting recovery after definitive antiparasitic treatment, but is not a substitute for diagnosis and targeted treatment in symptomatic infection. The traditional use was largely in settings where parasitic burden was high and pharmaceutical antiparasitic therapy was unavailable — a context that no longer applies for patients with access to modern diagnostics and treatment.
Biofilm Disruption
An emerging area of antimicrobial research is the activity of plant essential oils against bacterial and fungal biofilms — the structured communities of organisms embedded in extracellular polymer matrix that resist both host immunity and antibiotic penetration. Biofilms are clinically important in dental plaque, chronic wound infection, urinary catheter colonization, prosthetic device infection, and the persistent gut microbial colonization seen in SIBO and IBS.
Thymol and carvacrol have documented biofilm-disrupting activity that exceeds the activity of many conventional antibiotics in biofilm-protected populations:
- Prevention of biofilm formation — subinhibitory concentrations of thymol that do not kill free-swimming bacteria can still prevent the initial surface attachment and matrix synthesis that begins biofilm formation.
- Disruption of established biofilms — higher concentrations of thymol penetrate the extracellular polymer matrix more effectively than many antibiotics and reach the embedded bacterial cells.
- Synergy with conventional antibiotics — thymol pretreatment of biofilms can dramatically lower the antibiotic concentration required to kill the embedded bacteria, restoring effectiveness of antibiotics that would otherwise be ineffective against the biofilm form.
- Dental plaque applications — this is the basis for the thymol content of commercial mouthwashes; the same activity is present in traditional ajwain-water oral rinse.
The clinical translation of biofilm-disrupting activity into routine practice is still evolving, but the mechanism is plausible and the in vitro evidence is consistent.
Cautions: Microbiome Selectivity and Long-Term Use
- Broad-spectrum antimicrobial activity is not selective — ajwain's thymol affects beneficial commensal bacteria as well as pathogens. The traditional culinary use (small doses with food) is unlikely to meaningfully disrupt the commensal flora, but sustained high-dose use (concentrated essential oil capsules taken for months) might. The reasonable approach is to use ajwain in courses (two to four weeks of therapeutic dosing followed by a break) rather than continuous high-dose intake, and to combine with prebiotic and probiotic support during and after the treatment course. See our Probiotics page.
- Concentrated essential oil internal use — concentrated ajwain essential oil should not be taken internally except under professional Ayurvedic or naturopathic supervision. Hepatotoxicity at high doses, mucosal irritation, and dose miscalculation are real risks. Whole seed and ajwain water preparations are far safer.
- Pregnancy and infant safety — culinary doses are considered safe; therapeutic dosing for antimicrobial purposes should be deferred until postpartum and beyond infancy.
- Allergic sensitization to thymol — rare but reported. Patients with documented thyme or oregano allergy may cross-react with ajwain.
- Drug interactions — theoretical additive antimicrobial effect with concurrent antibiotic therapy (usually beneficial in the dysbiosis-adjunct context, but worth disclosing to the prescribing physician). Theoretical interaction with anticoagulants via mild platelet-inhibitory effect.
- Not a substitute for definitive treatment of serious infection — the recurring caution. Pneumonia, urinary tract infection, skin and soft tissue infection requiring antibiotics, parasitic infection requiring antiparasitic therapy, fungal infection requiring antifungal therapy — all need definitive conventional treatment. Ajwain is a complementary intervention in dysbiosis and mild conditions, not a primary antimicrobial in serious infection.
Key Research Papers
- Singh G et al. (2004). Antimicrobial and antifungal activities of essential oil and various oleoresins of Trachyspermum ammi. — PubMed
- Burt S (2004). Essential oils: their antibacterial properties and potential applications in foods — a review. International Journal of Food Microbiology. — PubMed
- Lambert RJ et al. (2001). A study of the minimum inhibitory concentration and mode of action of oregano essential oil, thymol and carvacrol. Journal of Applied Microbiology. — PubMed
- Marsik P et al. (2005). In vitro inhibitory effects of thymol and quinones from Trachyspermum ammi. — PubMed
- Hassanshahian M, Bayat Z, Saeidi S, Shiri Y (2014). Antimicrobial activity of Trachyspermum ammi essential oil against human bacterial pathogens. — PubMed
- Khan R et al. (2010). Antimicrobial activity of five herbal extracts against multi-drug-resistant clinical bacterial isolates (including T. ammi). — PubMed
- Sharifi-Rad J et al. (2018). Carvacrol and human health: a comprehensive review. Phytotherapy Research. — PubMed
- Nagoor Meeran MF et al. (2017). Pharmacological properties and molecular mechanisms of thymol: prospects for its therapeutic potential. Frontiers in Pharmacology. — PubMed
- Falsafi T, Moradi P, Mahboubi M et al. (2015). Chemical composition and anti-Helicobacter pylori effect of Satureja and related thymol-rich essential oils. — PubMed
- Bukhari IA et al. (2008). Anti-inflammatory and analgesic effects of Trachyspermum ammi in animal models. — PubMed
- Bakkali F, Averbeck S, Averbeck D, Idaomar M (2008). Biological effects of essential oils — a review. Food and Chemical Toxicology. — PubMed
- Chouhan S, Sharma K, Guleria S (2017). Antimicrobial activity of some essential oils — present status and future perspectives. Medicines. — PubMed
PubMed Topic Searches
- PubMed: Ajwain antimicrobial activity
- PubMed: Thymol + carvacrol membrane mechanism
- PubMed: Ajwain antifungal + Candida
- PubMed: Thymol against MRSA
- PubMed: Essential oils against H. pylori
Connections
- Ajwain Overview
- Ajwain Benefits Hub
- Ajwain for Digestion
- Ajwain for Respiratory Health
- Ajwain for Pain & Inflammation
- SIBO
- Helicobacter pylori
- Aflatoxin
- Oregano (Carvacrol Source)
- Thyme (Thymol Source)
- Garlic (Allicin)
- Turmeric
- Probiotics
- Gut Healing
- Bloating