Bitter Melon for Diabetes Complications
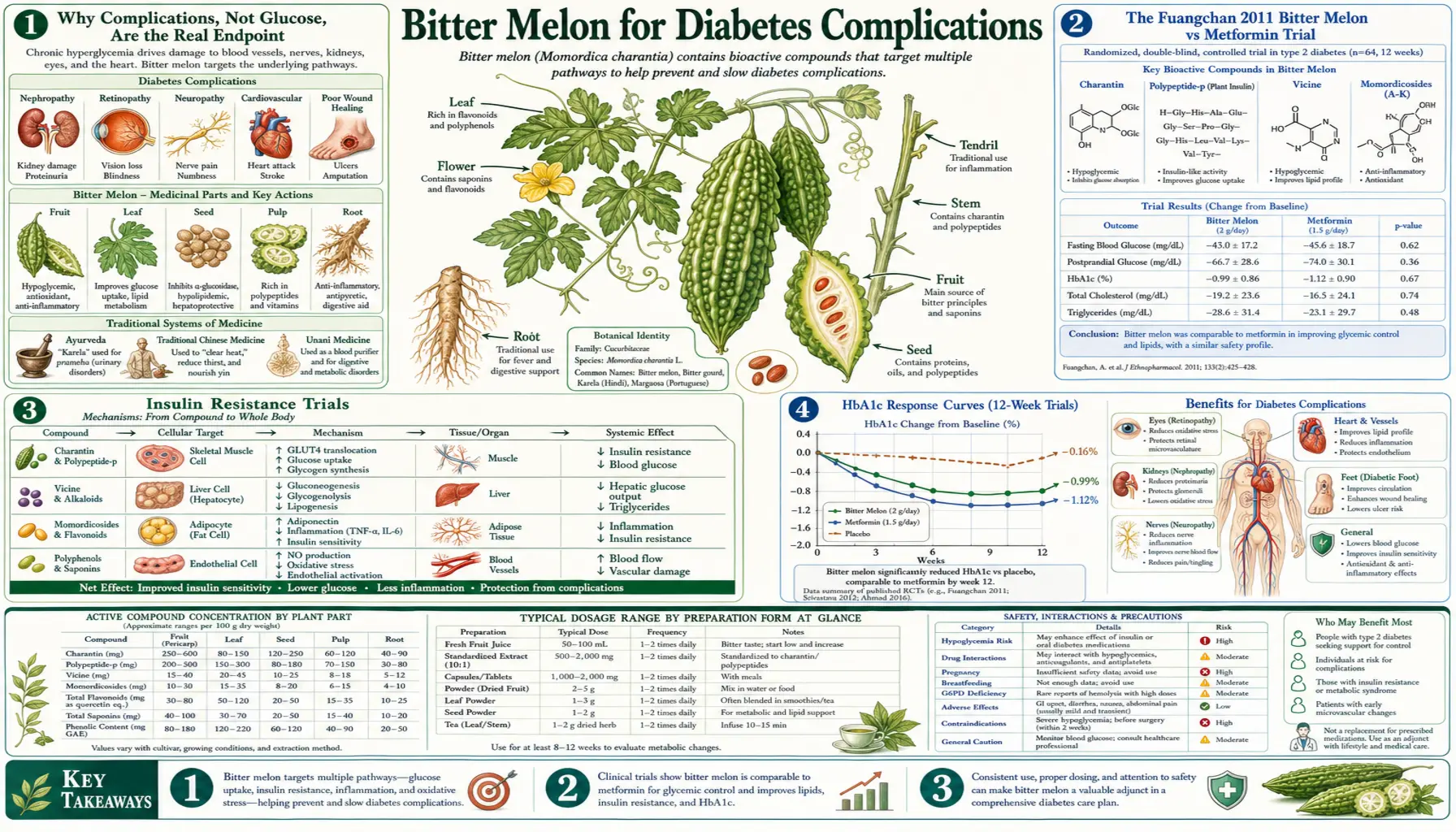
The case for bitter melon shifts when we move past simple glycemic control and into the broader question of preventing or slowing the downstream microvascular and macrovascular complications of long-standing diabetes — retinopathy, nephropathy, neuropathy, atherosclerosis, and the foot ulcers that can spiral into amputation. Here the clinical data are weaker and the comparative story is unflattering: the seminal Fuangchan et al. 2011 head-to-head randomized trial of bitter melon versus pharmaceutical metformin in newly diagnosed type 2 diabetics in Thailand found that 1 g/day metformin produced significantly greater HbA1c reduction than 2 g/day bitter melon, with no convergence at four weeks. The honest read of the comparative literature is that bitter melon does not match pharmaceutical metformin in glycemic potency, and therefore by extension does not match it for prevention of microvascular complications — which depend on cumulative HbA1c exposure (the UKPDS and DCCT trials are the foundational evidence). Where bitter melon does have a legitimate place is as an early-stage adjunct in prediabetes and well-controlled type 2 diabetes, as a vehicle for the insulin-sensitizing effect that reduces the dose of pharmaceutical agents required, and as part of a comprehensive metabolic plan that includes diet, exercise, and pharmaceutical therapy together rather than as alternatives.
Table of Contents
- Why Complications, Not Glucose, Are the Real Endpoint
- The Fuangchan 2011 Bitter Melon vs Metformin Trial
- Insulin Resistance Trials
- HbA1c Response Curves
- Indian Charantia Trials in Newly Diagnosed Type 2 Diabetes
- Retinopathy: The Eye Complication
- Nephropathy: The Kidney Complication
- Neuropathy: The Nerve Complication
- Macrovascular Disease and Cardiovascular Risk
- Bitter Melon as an Adjunct, Not a Substitute
- Cautions and Practical Guidance
- Key Research Papers
- Connections
- Featured Videos
Why Complications, Not Glucose, Are the Real Endpoint
Glucose is a surrogate marker. The reason we worry about elevated glucose is not because the number on a meter is large; it is because chronic hyperglycemia damages tissues through several well-characterized molecular pathways — the formation of advanced glycation end products (AGEs), oxidative stress from mitochondrial superoxide overproduction in vascular endothelium, polyol pathway activation, and protein kinase C pathway dysregulation. These molecular insults, accumulated over years, produce the microvascular complications (retinopathy, nephropathy, neuropathy) and macrovascular complications (atherosclerosis, myocardial infarction, stroke) that cause the morbidity and mortality of diabetes.
The two foundational trials of glycemic control and complication prevention are the United Kingdom Prospective Diabetes Study (UKPDS) for type 2 diabetes and the Diabetes Control and Complications Trial (DCCT) for type 1 diabetes. Both trials demonstrated that tight glycemic control significantly reduces microvascular complications, with the effect approximately linear in cumulative HbA1c exposure over time — an effect sometimes called “metabolic memory” because it persists for years after a period of better control.
The implication for bitter melon: any agent that meaningfully lowers HbA1c will, over time, reduce microvascular complication risk in proportion to the magnitude of HbA1c reduction. A 0.3-0.5 percentage point HbA1c reduction from bitter melon (per the Yin meta-analysis) translates to a measurable but modest reduction in projected complication risk. A 1.5-2.0 percentage point HbA1c reduction from pharmaceutical metformin (or insulin in advanced disease) translates to a much larger reduction. The relative magnitudes matter for clinical decision-making.
The Fuangchan 2011 Bitter Melon vs Metformin Trial
The most important head-to-head comparison is Fuangchan A, Sonthisombat P, Seubnukarn T, et al., “Hypoglycemic effect of bitter melon compared with metformin in newly diagnosed type 2 diabetes patients,” published in Journal of Ethnopharmacology in 2011. The trial was conducted at Naresuan University Hospital in Phitsanulok, Thailand, and enrolled 143 newly diagnosed type 2 diabetic patients who had not previously taken pharmaceutical diabetes therapy.
Patients were randomized to one of four arms:
- Bitter melon 500 mg/day (low dose)
- Bitter melon 1,000 mg/day (mid dose)
- Bitter melon 2,000 mg/day (high dose)
- Metformin 1,000 mg/day (reference arm)
The primary endpoint was the change in fructosamine (a 2-3 week glycemic marker, used because the trial was only 4 weeks) from baseline. Results:
- Bitter melon 2,000 mg/day — small but statistically significant fructosamine reduction
- Bitter melon 500 mg/day and 1,000 mg/day — no statistically significant effect
- Metformin 1,000 mg/day — significantly greater fructosamine reduction than any bitter melon dose
The Fuangchan trial is the most-cited comparative clinical study of bitter melon and is the source of the now-standard statement in the integrative-medicine literature that “bitter melon is less effective than 1 g/day metformin.” The trial has been criticized for short duration (4 weeks may not capture maximal bitter melon effect) and for using a relatively low metformin reference dose (most diabetics on metformin take 1,500-2,000 mg/day, not 1,000 mg/day). But even with those caveats, the magnitude of the effect-size difference was large enough that no plausible follow-up trial has reversed the conclusion: pharmaceutical metformin is the more potent agent.
The honest clinical reading: for a patient with newly diagnosed type 2 diabetes who can tolerate metformin, metformin should be the first-line agent. Bitter melon is reasonable as an adjunct or as an alternative for the patient who declines or cannot tolerate metformin, but it is not a metformin substitute.
Insulin Resistance Trials
The bitter melon literature includes a smaller set of trials focused specifically on insulin resistance — the underlying metabolic disturbance that precedes overt type 2 diabetes by years to decades. Insulin resistance is typically quantified by the HOMA-IR (Homeostatic Model Assessment of Insulin Resistance) index, calculated from fasting glucose and fasting insulin.
Bitter melon trials measuring HOMA-IR have generally shown 10-20% reductions over 8-12 weeks of standardized extract supplementation, comparable in magnitude to lifestyle interventions and to lower-dose metformin. The mechanism is the AMPK activation discussed in the Blood Sugar deep-dive — AMPK activation increases insulin-independent glucose uptake into muscle, suppresses hepatic glucose output, and over time improves insulin signaling at the receptor level.
For patients with prediabetes (fasting glucose 100-125 mg/dL, HbA1c 5.7-6.4%, or impaired glucose tolerance on OGTT), bitter melon is a reasonable trial as part of a broader insulin-sensitizing plan that includes:
- Carbohydrate moderation, particularly reduction of refined-carbohydrate and added-sugar intake
- Regular aerobic and resistance exercise (both directly activate AMPK)
- Adequate sleep (insufficient sleep is independently insulin-desensitizing)
- Stress management (chronic cortisol elevation drives insulin resistance)
- Often berberine or pharmaceutical metformin if metabolic markers do not improve with lifestyle alone
For the broader picture of insulin resistance management, see our Insulin Resistance page.
HbA1c Response Curves
Across the bitter melon RCT literature, the HbA1c response shows characteristic features that are useful to understand for setting realistic patient expectations:
- Onset — measurable HbA1c change typically requires 8-12 weeks. The shorter Fuangchan trial used fructosamine because 4 weeks is too brief for HbA1c to fully respond (red cell turnover takes ~120 days, so HbA1c reflects roughly the past 3 months).
- Magnitude — per the Yin 2014 meta-analysis, typical reduction is 0.2-0.5 percentage points at 12 weeks. A baseline HbA1c of 8.0% might fall to 7.5-7.8%. This is enough to be meaningful for projected complication risk but is smaller than the typical response to metformin (1.0-1.5 percentage points).
- Plateau — effect appears to plateau at 3-6 months. Continued use sustains the reduction but does not produce further gains.
- Dose-response — weakly dose-dependent up to about 2,000 mg/day of standardized extract; higher doses do not appear to produce proportionally larger effects and may increase gastrointestinal adverse events.
- Baseline-dependent — larger absolute HbA1c reduction in patients with higher baseline HbA1c (a common finding in glycemic-control studies because there is more “room to fall”). Patients with HbA1c above 8.5% see proportionally larger reductions than patients near the diabetes diagnostic threshold of 6.5%.
For the deeper interpretation of HbA1c and its relationship to projected complication risk, see our HbA1c page and the A1c, Fructosamine, and Glycation Markers deep-dive.
Indian Charantia Trials in Newly Diagnosed Type 2 Diabetes
A substantial fraction of the bitter melon clinical trial literature comes from the Indian subcontinent, where bitter melon (karela) has been a staple of both Ayurvedic and modern integrative diabetes practice for generations. These trials are conducted at Indian medical schools and Ayurvedic research centers, and they are sometimes overlooked in Western reviews because of journal-indexing and language considerations — but they constitute an important body of evidence.
Representative trials include:
- Ahmed et al. (1999, Bangladesh) — bitter melon extract reduced both fasting and postprandial glucose in NIDDM (non-insulin-dependent diabetes mellitus) patients
- Srivastava et al. (1993) — bitter melon juice produced modest reductions in fasting glucose and glycosylated hemoglobin in type 2 diabetic patients
- Multiple Indian studies of standardized Momordica extracts — consistently showing modest fasting glucose and HbA1c reductions, with effect sizes broadly comparable to the Yin meta-analysis pooled estimate
The Indian trial literature is generally consistent with the broader meta-analytic findings — bitter melon is a real but modest hypoglycemic agent, well-tolerated at typical doses, and a reasonable adjunct in early-stage type 2 diabetes management. Where Indian trials sometimes diverge from Western trials is in the formulation: many Indian trials use fresh juice or unprocessed fruit powder, while many Western trials use standardized extracts. The fresh-juice trials tend to report somewhat larger acute glycemic effects (consistent with the Welihinda 1986 OGTT findings), while the extract trials show more consistent but smaller chronic HbA1c effects.
Retinopathy: The Eye Complication
Diabetic retinopathy is the leading cause of new-onset blindness in working-age adults in the developed world. Chronic hyperglycemia damages retinal capillaries through the AGE, oxidative-stress, and polyol-pathway mechanisms discussed above, producing microaneurysms, hemorrhages, exudates, neovascularization (proliferative diabetic retinopathy), and eventually retinal detachment or vitreous hemorrhage.
There are no large randomized controlled trials of bitter melon for retinopathy prevention. The reasonable extrapolation is that whatever HbA1c reduction bitter melon produces will translate to a proportional reduction in retinopathy risk over time — per the UKPDS, every 1.0 percentage point reduction in mean HbA1c corresponds to roughly 35% reduction in microvascular endpoint risk. A 0.3-0.5 percentage point reduction from bitter melon would therefore correspond to roughly 10-17% relative risk reduction for retinopathy, all else being equal.
This is meaningful but small relative to what metformin or insulin can deliver in patients with higher baseline HbA1c. For the patient at risk for diabetic retinopathy, the priority is comprehensive glycemic control by whatever combination of lifestyle and pharmaceutical agents is needed; bitter melon is a reasonable adjunct that may contribute to that overall control. For deeper exploration of the retinopathy mechanism, see the Complications: Retinopathy, Nephropathy, Neuropathy deep-dive.
Nephropathy: The Kidney Complication
Diabetic nephropathy is the leading cause of end-stage renal disease in the United States and most of the developed world. It begins with hyperfiltration and glomerular hypertrophy, progresses through microalbuminuria (30-300 mg/g creatinine), then macroalbuminuria (above 300 mg/g), and eventually to falling glomerular filtration rate and need for dialysis or transplantation.
Animal-model studies of bitter melon in diabetic nephropathy have shown reductions in proteinuria and improvements in renal histology, attributable to the underlying glucose reduction plus possible direct effects of bitter melon polyphenols on glomerular oxidative stress. Human trials are sparse and small.
A practical caveat: bitter melon's effect on renal function in humans with advanced chronic kidney disease is not well-characterized. Patients with CKD stage 3 or worse should discuss bitter melon with their nephrologist before starting, particularly because most bitter melon supplements have not been formally evaluated for renal safety, and because added hypoglycemic effect in CKD patients (who often have unpredictable insulin and sulfonylurea pharmacokinetics) can be particularly risky.
The first-line renoprotective interventions for diabetic nephropathy remain ACE inhibitors or ARBs, SGLT2 inhibitors (which have substantial outcome trial evidence for renal protection independent of glucose lowering), and aggressive blood pressure and HbA1c control. Bitter melon is not a renoprotective drug in the sense that SGLT2 inhibitors are; it is a glucose-lowering plant that may contribute incrementally to the underlying glycemic control upon which renoprotection depends. See the Cardio-Renal Protection: SGLT2 and GLP-1 deep-dive for the modern pharmacological renoprotective strategy.
Neuropathy: The Nerve Complication
Diabetic peripheral neuropathy affects approximately 50% of patients with long-standing diabetes and is a leading cause of foot ulcers, falls, chronic neuropathic pain, and lower-extremity amputation. The pathology involves damage to small unmyelinated nerve fibers from the same hyperglycemia-driven mechanisms (AGE formation, oxidative stress, polyol pathway) that damage retinal and renal microvasculature.
Bitter melon has not been studied as a primary intervention for established diabetic neuropathy. The reasonable expectation is that whatever HbA1c reduction bitter melon provides will, over years, slow the progression of neuropathy in patients who do not yet have advanced disease — the same general logic as for retinopathy and nephropathy.
For patients with established diabetic neuropathy, more directly evidence-based interventions include:
- Alpha-lipoic acid (600-1,800 mg/day) — the most studied neuroprotective antioxidant, with the German ALADIN, ORPIL, and SYDNEY trials supporting symptomatic and possibly disease-modifying effect
- Benfotiamine (fat-soluble vitamin B1 derivative) — reduces AGE formation and shows symptomatic benefit in clinical trials
- Vitamin B12 (especially methylcobalamin) — particularly important for patients on long-term metformin, which depletes B12 stores
- Standard pharmacological options — gabapentin, pregabalin, duloxetine for symptomatic neuropathic pain
Bitter melon's role in the neuropathy story is upstream — reducing the chronic hyperglycemic exposure that drives nerve damage in the first place — rather than treating established neuropathy directly.
Macrovascular Disease and Cardiovascular Risk
The macrovascular complications of diabetes — coronary artery disease, cerebrovascular disease, peripheral arterial disease — are statistically the leading cause of death in patients with type 2 diabetes. The mechanism is accelerated atherosclerosis, driven by the combination of hyperglycemia, insulin resistance, dyslipidemia (the diabetic triad of elevated triglycerides, low HDL, and small-dense LDL), hypertension, and the prothrombotic state of poorly controlled diabetes.
Bitter melon has been studied for its lipid-modifying effects, with most trials reporting modest improvements in total cholesterol, LDL, and triglycerides, plus modest increases in HDL, over 8-12 weeks of supplementation. The mechanism is partly attributed to the seed-derived conjugated linolenic acids, which activate PPAR-alpha and PPAR-gamma, the same nuclear receptors targeted by the fibrate and thiazolidinedione drug classes.
The cardiovascular outcome trial data — the gold standard evidence for whether an intervention actually prevents heart attacks and strokes — do not exist for bitter melon. The realistic interpretation is that bitter melon contributes to a more favorable metabolic profile (modestly lower glucose, modestly better lipids, modest improvement in insulin sensitivity), which over years would be expected to translate to incrementally reduced macrovascular risk, but the magnitude is modest. The interventions with proven cardiovascular outcome benefit in type 2 diabetes are pharmaceutical: SGLT2 inhibitors (empagliflozin, dapagliflozin, canagliflozin), GLP-1 agonists (semaglutide, liraglutide), and aggressive treatment of hypertension and dyslipidemia.
Bitter Melon as an Adjunct, Not a Substitute
The unifying theme across all of these complication categories is that bitter melon is a reasonable adjunct in a comprehensive metabolic management plan but should not be considered a substitute for evidence-based pharmaceutical therapy in patients who need it. The appropriate framing for different patient categories:
- Prediabetes (fasting glucose 100-125 mg/dL, HbA1c 5.7-6.4%) — bitter melon is a reasonable lifestyle-tier intervention alongside dietary modification and exercise; many patients can normalize metabolic markers with this combination and avoid progression to overt diabetes. Berberine is a more potent alternative in this category and is often preferred for patients who want a single-agent botanical with greater potency.
- Newly diagnosed type 2 diabetes (HbA1c 6.5-7.5%, no complications) — metformin is the first-line pharmaceutical agent (cheap, effective, well-tolerated, cardioprotective). Bitter melon can be added as a complementary intervention if HbA1c is not at target on metformin alone, or if the patient declines metformin and is willing to attempt an intensive lifestyle plus botanical strategy with close monitoring.
- Established type 2 diabetes on multiple agents — bitter melon is a reasonable add-on but unlikely to substantively change the medication regimen. Modest HbA1c reduction may permit modest reduction in some medication doses, but the patient should be in routine endocrinology follow-up and changes should be guided by the prescribing physician.
- Type 1 diabetes — bitter melon cannot replace insulin. The pancreatic beta cells are absent or destroyed; no oral hypoglycemic agent (botanical or pharmaceutical) addresses that. Bitter melon may modestly reduce insulin requirements through the peripheral mechanisms (GLUT4, AMPK) but is not a substitute for insulin therapy.
- Established microvascular or macrovascular complications — the appropriate management is intensive evidence-based therapy targeting the specific complication (ACE inhibitor/ARB and SGLT2 inhibitor for nephropathy, alpha-lipoic acid and pharmacological pain management for neuropathy, ophthalmology referral and intravitreal therapy for proliferative retinopathy, statin and antihypertensive for macrovascular risk). Bitter melon is an upstream adjunct, not a treatment for the complications themselves.
Cautions and Practical Guidance
- G6PD deficiency — absolute contraindication for the seeds (vicine content); test if of Mediterranean, African, Middle Eastern, or South/Southeast Asian ancestry
- Pregnancy — absolute contraindication; uterine-stimulating activity
- Combination with sulfonylureas, insulin, meglitinides — additive hypoglycemic effect; monitor glucose closely and reduce medication dose as needed under prescriber supervision
- Combination with metformin — mild additive effect; usually well-tolerated but worth monitoring for the first 2-4 weeks
- Chronic kidney disease stage 3 or worse — discuss with nephrologist before starting; bitter melon's renal safety in advanced CKD is not well-characterized
- Not a metformin substitute — Fuangchan 2011 established that pharmaceutical metformin is more potent; the appropriate framing is adjunct, not alternative
- Not a treatment for established complications — retinopathy, advanced nephropathy, and symptomatic neuropathy require condition-specific evidence-based therapy under specialist management
Key Research Papers
- Fuangchan A, Sonthisombat P, Seubnukarn T, Chanouan R, Chotchaisuwat P, Sirigulsatien V, Ingkaninan K, Plianbangchang P, Haines ST (2011). Hypoglycemic effect of bitter melon compared with metformin in newly diagnosed type 2 diabetes patients. Journal of Ethnopharmacology 134(2):422-428. — PubMed
- Yin RV, Lee NC, Hirpara H, Phung OJ (2014). The effect of bitter melon (Mormordica charantia) in patients with diabetes mellitus: a systematic review and meta-analysis. Nutrition & Diabetes 4(12):e145. — PubMed
- UK Prospective Diabetes Study (UKPDS) Group (1998). Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). The Lancet 352(9131):837-853. — PubMed
- Diabetes Control and Complications Trial Research Group (1993). The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. NEJM 329(14):977-986. — PubMed
- Stratton IM et al. (2000). Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35). BMJ 321(7258):405-412. — PubMed
- Welihinda J, Karunanayake EH, Sheriff MH, Jayasinghe KS (1986). Effect of Momordica charantia on the glucose tolerance in maturity onset diabetes. Journal of Ethnopharmacology 17(3):277-282. — PubMed
- Ahmed I, Adeghate E, Sharma AK, Pallot DJ, Singh J (1998). Effects of Momordica charantia fruit juice on islet morphology in the pancreas of the streptozotocin-diabetic rat. Diabetes Research and Clinical Practice 40(3):145-151. — PubMed
- Srivastava Y, Venkatakrishna-Bhatt H, Verma Y, Venkaiah K, Raval BH (1993). Antidiabetic and adaptogenic properties of Momordica charantia extract: an experimental and clinical evaluation. Phytotherapy Research 7(4):285-289. — PubMed
- Tongia A, Tongia SK, Dave M (2004). Phytochemical determination and extraction of Momordica charantia fruit and its hypoglycemic potentiation of oral hypoglycemic drugs in diabetes mellitus (NIDDM). Indian Journal of Physiology and Pharmacology 48(2):241-244. — PubMed
- Dans AM, Villarruz MV, Jimeno CA, Javelosa MA, Chua J, Bautista R, Velez GG (2007). The effect of Momordica charantia capsule preparation on glycemic control in type 2 diabetes mellitus needs further studies. Journal of Clinical Epidemiology 60(6):554-559. — PubMed
- John AJ, Cherian R, Subhash HS, Cherian AM (2003). Evaluation of the efficacy of bitter gourd (Momordica charantia) as an oral hypoglycemic agent — a randomized controlled clinical trial. Indian Journal of Physiology and Pharmacology 47(3):363-365. — PubMed
- Inayat-ur-Rahman, Malik SA, Bashir M, Khan R, Iqbal M (2009). Serum sialic acid changes in non-insulin-dependent diabetes mellitus (NIDDM) patients following bitter melon (Momordica charantia) and rosiglitazone (Avandia) treatment. Phytomedicine 16(5):401-405. — PubMed
PubMed Topic Searches
- PubMed: Bitter melon vs metformin
- PubMed: Bitter melon HOMA-IR / insulin resistance
- PubMed: Bitter melon lipid profile
- PubMed: Bitter melon diabetic nephropathy
- PubMed: Bitter melon microvascular complications
Connections
- Bitter Melon (Main Page)
- Bitter Melon Benefits Hub
- Bitter Melon for Blood Sugar
- Bitter Melon for Weight Loss
- Bitter Melon Cancer Cell Studies
- Berberine
- Gymnema
- Diabetes
- Insulin Resistance
- Diabetes Complications: Retinopathy, Nephropathy, Neuropathy
- Cardio-Renal Protection: SGLT2 and GLP-1
- A1c, Fructosamine, and Glycation Markers
- Peripheral Neuropathy
- Alpha-Lipoic Acid for Diabetic Neuropathy
- Benfotiamine for Diabetic Neuropathy
- HbA1c
- Fasting Insulin
- Blood Sugar Management
- Metformin — the pharmaceutical comparator that beat every bitter melon dose in the Fuangchan 2011 head-to-head trial.