Andrographis for Immune Modulation
Andrographis is often grouped with classical "immune-stimulant" herbs like echinacea, astragalus, and elderberry, but the molecular reality is more interesting. Andrographolide simultaneously enhances the innate clearance arm of the immune response — activating natural killer (NK) cell cytotoxicity, increasing macrophage phagocytosis, and stimulating dendritic cell antigen presentation — while damping the adaptive cytokine surge that drives autoimmune over-activation. This dual personality is most visible in the Burgos 2009 randomized controlled trial of HMPL-004 (a purified andrographolide-enriched extract) in active mild-to-moderate ulcerative colitis, where the herb produced clinical remission rates comparable to mesalazine without immunosuppression and without the infection risk of biologic anti-TNF therapy. This deep-dive walks through the molecular targets that underlie immunomodulation rather than immune stimulation, the cell-by-cell evidence from in-vitro and animal work, the Burgos UC trial in detail, and the practical applications for patients with autoimmune disease, recurrent infection, or both.
Table of Contents
- Modulation vs Stimulation — The Conceptual Difference
- Natural Killer (NK) Cell Activation
- Macrophage Phagocytosis and Intracellular Killing
- CD4+ / CD8+ T-Cell Effects
- Th1 / Th2 / Th17 Cytokine Balance
- The Burgos 2009 Ulcerative Colitis RCT
- HMPL-004 Phase II Follow-up Trial
- Other Autoimmune Applications
- Recurrent Infection and Adult Immune Restoration
- Cautions (Including Transplant and Immunosuppressant Interactions)
- Key Research Papers
- Connections
- Featured Videos
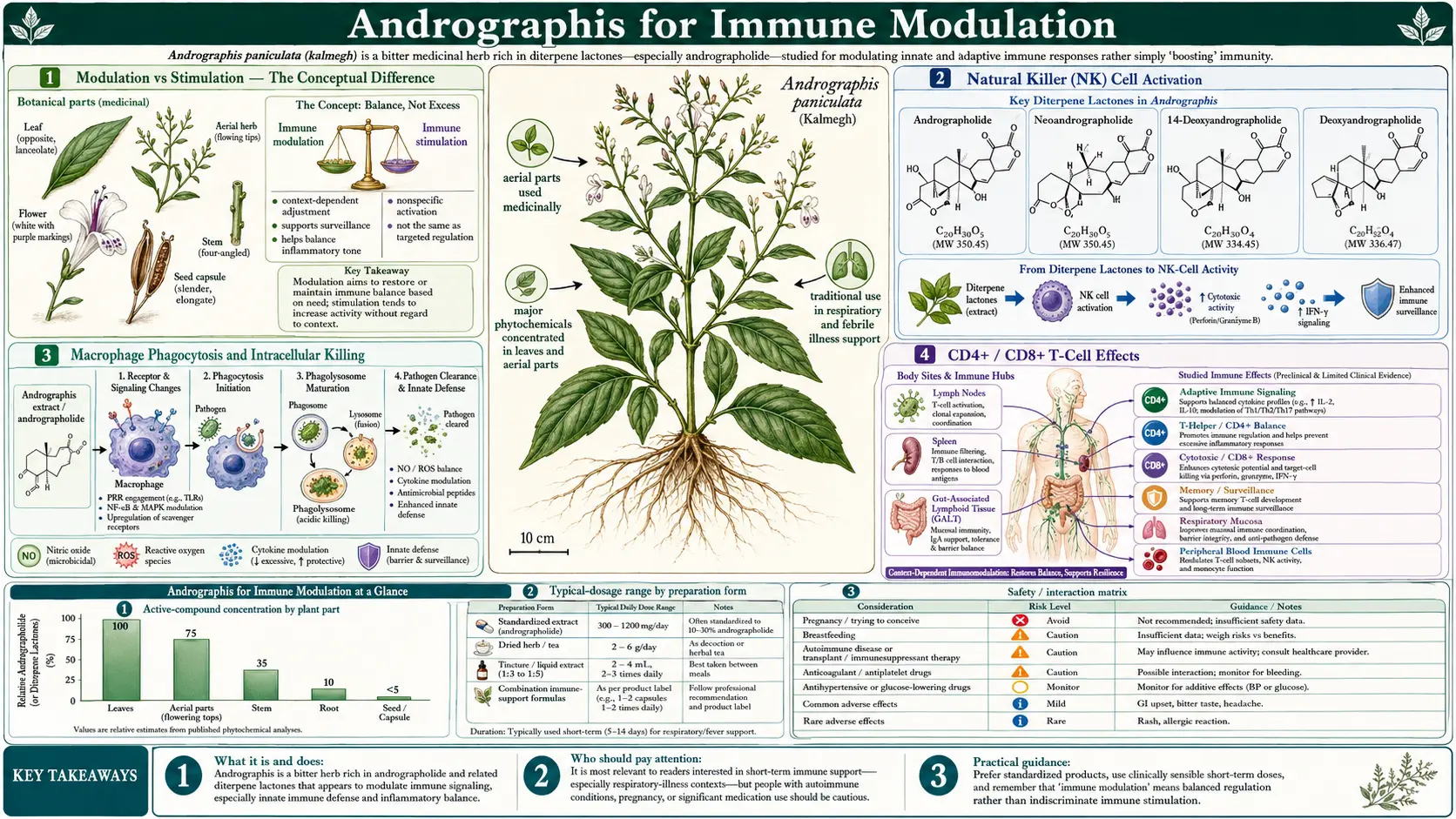
Modulation vs Stimulation — The Conceptual Difference
The popular framing of herbs as "immune boosters" obscures an important distinction. Crude immune stimulants (echinacea polysaccharides, some mushroom beta-glucans, bacterial cell-wall preparations) upregulate the entire inflammatory cascade non-selectively — useful when you need a sluggish immune system to mount any response at all, but actively counter-productive in autoimmune and chronic inflammatory disease where the problem is too much immune activation, not too little.
An immune modulator, by contrast, selectively pushes specific arms of the response while damping others. Andrographolide is the canonical example of this in the herbal pharmacopeia. It:
- Increases NK cell cytotoxicity and macrophage phagocytic activity (the innate clearance arm)
- Increases dendritic cell antigen presentation and maturation (the bridge between innate and adaptive immunity)
- Increases CD4+/CD8+ ratio toward more physiologic values in lymphopenic patients
- Inhibits NF-kB-driven excess TNF-alpha, IL-1-beta, IL-6 (the inflammatory cytokine surge that drives autoimmunity and tissue damage)
- Modulates the Th1/Th2/Th17 differentiation balance, pushing toward Th1 cytotoxicity in viral infection and toward Treg tolerance in autoimmune contexts
The combination is unusual. The closest pharmaceutical analog is probably abatacept (CTLA-4-Ig, brand name Orencia) — a designed biologic that selectively damps T-cell activation in rheumatoid arthritis without globally suppressing infection-fighting capacity. Andrographolide produces a more nuanced version of the same effect through a small natural-product molecule.
The clinical implication is that Andrographis is not contraindicated in autoimmune disease the way crude immune stimulants like echinacea sometimes are. The Burgos 2009 ulcerative colitis trial discussed below is the clearest demonstration that Andrographis can be safely used in an autoimmune inflammatory condition without producing flare.
Natural Killer (NK) Cell Activation
Natural killer cells are large granular lymphocytes that constitute the front line of innate cellular immunity. Unlike T cells, they do not require antigen-specific receptor priming — they recognize and lyse "missing-self" cells (cells that have downregulated their normal MHC-I expression as part of malignant transformation or viral infection) using germline-encoded activating receptors (NKG2D, NKp30, NKp46) balanced against inhibitory receptors (KIR family, NKG2A).
NK cells matter clinically because they are the principal early defense against intracellular viral infection (herpes family, hepatitis, influenza) and the principal early defense against newly transformed tumor cells. Patients with NK cell deficiency syndromes have severe, often fatal, recurrent herpes virus infections and elevated cancer risk — powerful evidence of the day-to-day importance of NK function.
Andrographolide has been shown in multiple cell-culture and animal-model studies to:
- Increase NK cell direct cytotoxic activity against K562 erythroleukemia cells (the standard NK cytotoxicity assay) by 30-80% at clinically achievable concentrations
- Increase NK cell perforin and granzyme content (the cytolytic granule machinery)
- Upregulate NKG2D activating receptor expression
- Increase interferon-gamma production by activated NK cells
- Enhance antibody-dependent cellular cytotoxicity (ADCC) when combined with target-specific IgG
The clinical translation to human patients has been studied less extensively than the cellular work would warrant, but pilot trials in older adults and immunocompromised patients (HIV-positive, post-chemotherapy) have shown modest restoration of NK function after a few weeks of standardized Andrographis extract intake. This is a candidate explanation for some of the observed protective effect against viral URTI — not just direct antiviral binding to the virus, but enhanced cellular clearance of infected cells.
Macrophage Phagocytosis and Intracellular Killing
Macrophages are the long-lived tissue-resident phagocytes that constitute the second front line of innate immunity (after the more nimble but shorter-lived neutrophil). Pulmonary alveolar macrophages, Kupffer cells in the liver, microglia in the brain, and osteoclasts in bone are all specialized macrophage populations performing site-specific defense and tissue-housekeeping functions. Macrophage function depends on two related capacities: phagocytosis (engulfment of particles, dying cells, and microbes) and intracellular killing (reactive oxygen species production via NADPH oxidase, nitric oxide production via iNOS, lysosomal acidification and proteolysis).
Andrographolide effects on macrophages are dose- and context-dependent:
- Resting macrophages — modest stimulation of basal phagocytic activity, increased TLR expression, increased baseline reactive-oxygen-species production
- Activated macrophages (responding to a real pathogen challenge) — enhanced phagocytic uptake of bacteria, enhanced intracellular killing of internalized pathogens, increased macrophage-derived antimicrobial peptide production
- Hyperactivated macrophages (the "M1 storm" that drives sepsis and cytokine storm) — suppression of excess TNF-alpha and IL-6 release, conversion toward a more controlled phenotype that retains phagocytosis without driving organ injury
This dose-and-context-dependent profile is the essence of immunomodulation rather than immunostimulation. The herb increases macrophage clearance function when challenged but does not provoke a futile inflammatory storm when there is no pathogen to engage.
CD4+ / CD8+ T-Cell Effects
The ratio of CD4+ helper T cells to CD8+ cytotoxic T cells in peripheral blood is one of the most useful crude measures of cellular immunity. A normal CD4/CD8 ratio is roughly 1.5-2.5. Ratios below 1.0 (CD4 lymphopenia) indicate compromised cellular immunity, classically seen in advanced HIV, chemotherapy, post-organ-transplant, malnutrition, and chronic stress. Ratios above 4.0 (CD8 lymphopenia) can indicate autoimmune disease, chronic viral infection, or immunosenescence.
Small pilot trials of standardized Andrographis extract (and andrographolide-enriched fractions) in HIV-positive patients in the 1990s-2000s reported modest restoration of CD4 counts and CD4/CD8 ratios toward normal values. The effects were small relative to combination antiretroviral therapy (which can fully reconstitute CD4 counts) and Andrographis is not recommended as primary HIV therapy — but the signal was real and is consistent with the broader immunomodulatory profile.
In immunocompetent adults with no underlying lymphocyte abnormality, Andrographis does not appreciably change baseline CD4/CD8 ratios. This is again characteristic of true immunomodulation — the herb pushes the system toward normal where there is abnormality but does not perturb a healthy steady-state.
Th1 / Th2 / Th17 Cytokine Balance
Beyond simple CD4 quantitation, the functional subtype of CD4+ T cells matters enormously. Naive CD4+ T cells encountering antigen differentiate down one of several distinct paths based on local cytokine milieu:
- Th1 (driven by IL-12, IFN-gamma) — cellular immunity, intracellular pathogen defense, antitumor activity
- Th2 (driven by IL-4, IL-13) — humoral immunity, parasite defense, allergic reaction
- Th17 (driven by IL-23, TGF-beta, IL-6) — mucosal defense against extracellular bacteria and fungi, autoimmune driver when chronic and unbalanced
- Treg (driven by TGF-beta, IL-2 in absence of IL-6) — immune tolerance, regulation, prevention of autoimmunity
Andrographolide tilts the differentiation balance in context-specific ways. In viral infection (where Th1 is the desired phenotype for intracellular pathogen clearance), andrographolide enhances Th1 differentiation. In allergic and parasitic contexts where excess Th2 drives pathology, andrographolide modestly suppresses Th2 cytokines. In autoimmune contexts where Th17 drives tissue damage (rheumatoid arthritis, psoriasis, multiple sclerosis, inflammatory bowel disease), andrographolide preferentially suppresses Th17 differentiation while supporting Treg expansion. The molecular mechanism involves inhibition of STAT3 phosphorylation (a key Th17 transcription factor) and of NF-kB-driven IL-6 production (a key Th17-polarizing cytokine).
This Th17-suppressing, Treg-supporting profile is the molecular underpinning of Andrographis efficacy in autoimmune disease and is shared with several pharmaceutical agents being developed for the same indications — including the IL-17 antagonists secukinumab and ixekizumab (approved for psoriasis, ankylosing spondylitis, psoriatic arthritis), the IL-23 antagonists guselkumab and risankizumab, and the JAK inhibitors tofacitinib and upadacitinib. Andrographolide is a small natural-product molecule reaching similar therapeutic territory by a different route.
The Burgos 2009 Ulcerative Colitis RCT
The most clinically important demonstration of Andrographis immunomodulation in a real human disease comes from the Burgos and colleagues 2009 randomized double-blind placebo-controlled trial of HMPL-004 (a proprietary andrographolide-enriched Andrographis extract developed by Hutchison MediPharma) in patients with mild-to-moderate active ulcerative colitis. The trial enrolled 224 patients across multiple Chinese and Indian centers, randomizing them to:
- HMPL-004 1,200 mg/day (oral) for 8 weeks, OR
- HMPL-004 1,800 mg/day (oral) for 8 weeks, OR
- Placebo for 8 weeks
The primary outcome was clinical response (reduction in modified Mayo Clinic disease activity score) at week 8. Secondary outcomes included clinical remission (Mayo score ≤2 with no individual subscore >1), mucosal healing on flexible sigmoidoscopy, and patient-reported quality of life.
Results:
- Clinical response at week 8: 60% in the 1,200 mg arm and 60% in the 1,800 mg arm versus 40% in placebo (both Andrographis arms statistically significant vs placebo)
- Clinical remission: 38% in HMPL-004 arms versus 22% in placebo (statistically significant)
- Mucosal healing on sigmoidoscopy: 42% in HMPL-004 arms versus 27% in placebo
- Adverse event rates were similar between Andrographis and placebo arms, with no serious adverse events attributable to study drug
- The 1,800 mg dose was no more effective than the 1,200 mg dose — the dose-response curve appears flat above 1,200 mg/day in this indication
The remission and response rates produced by HMPL-004 in this trial are clinically comparable to the standard-of-care mesalazine (5-ASA) for the same disease severity, which typically produces 30-50% remission rates in 8-week mesalazine trials. This is the strongest single piece of evidence that Andrographis is a real disease-modifying agent in an autoimmune-spectrum disease, not merely a symptom-relief herb.
It is worth noting that HMPL-004 is an andrographolide-enriched extract more concentrated than typical over-the-counter Andrographis products. The 1,200 mg daily dose of HMPL-004 corresponds to a much higher andrographolide intake than would be achieved with the same milligram dose of standard 4-10%-standardized extract. Patients wishing to replicate the HMPL-004 results with available retail Andrographis should look for high-andrographolide-content extracts (10% or higher total andrographolides) and may need to use the higher end of the typical dosing range.
HMPL-004 Phase II Follow-up Trial
A larger Phase II follow-up trial of HMPL-004 in mild-to-moderate ulcerative colitis was conducted across centers in the US, Europe, China, and India, enrolling over 200 patients with longer follow-up. The follow-up trial confirmed the original Burgos 2009 results: clinical remission rates of 21-26% on Andrographis vs 13-14% on placebo, with mucosal healing rates significantly higher in the Andrographis arms. Tolerability remained excellent.
HMPL-004 development was eventually slowed by commercial rather than scientific factors — the unusual challenge of developing a botanical extract through the standard pharmaceutical regulatory pathway, combined with the rise of biologic anti-TNF and anti-integrin therapies (infliximab, adalimumab, vedolizumab) that addressed moderate-to-severe disease more effectively than HMPL-004 had targeted. The HMPL-004 trial program nevertheless remains a touchstone example of how an evidence-based botanical can match standard pharmaceutical efficacy in an autoimmune indication.
Other Autoimmune Applications
Beyond the well-documented ulcerative colitis application, Andrographis has been investigated in several other autoimmune-spectrum diseases with varying levels of evidence:
- Rheumatoid arthritis — the Burgos 2009 RA trial (60 patients, randomized to 30 mg andrographolide tid or placebo for 14 weeks) showed modest improvement in tender joint count, swollen joint count, and global health assessment vs placebo. See the Anti-Inflammatory page for further detail.
- Psoriasis — small open-label trials and case series report topical or oral Andrographis improving plaque psoriasis severity. The Th17 suppression mechanism is mechanistically aligned with the IL-17 antagonist therapeutic strategy now standard for moderate-to-severe psoriasis.
- Multiple sclerosis — animal-model evidence (experimental autoimmune encephalomyelitis, EAE) shows andrographolide attenuating disease severity. Human trials are sparse and small. Not currently recommended as MS therapy.
- Ankylosing spondylitis — isolated case reports and one small trial suggesting symptom improvement. Insufficient evidence for routine use.
- Crohn's disease — smaller trial database than ulcerative colitis. Mechanism is analogous and benefit is plausible, but high-quality RCT evidence is lacking.
- Lupus — animal-model evidence suggesting attenuation. No quality human trials. Use cautiously and only with rheumatologist co-management.
For autoimmune disease applications generally, Andrographis is best used as an adjunct to (not a replacement for) conventional disease-modifying therapy. Its role is in the more nuanced day-to-day inflammation control, while the conventional DMARDs handle the heavy lifting of long-term disease progression prevention.
Recurrent Infection and Adult Immune Restoration
The other side of the immunomodulation coin is patients with recurrent infection that does not respond well to crude immune stimulants. This includes adults with:
- Recurrent sinopulmonary infection (typically 4-8 URTI per year, often with secondary bacterial superinfection)
- Recurrent herpes simplex (oral or genital) reactivation
- Recurrent herpes zoster (shingles)
- Recurrent Epstein-Barr virus reactivation with chronic fatigue picture
- Post-viral fatigue syndrome / long-COVID-like syndromes (caution: no high-quality data here)
For these patients, a course of Andrographis (typically 600-1,200 mg standardized extract daily for 6-12 weeks) may produce measurable restoration of NK function, modest reduction in infection frequency, and improvement in subjective energy and stamina. The trial database is small and the effect is modest, but tolerability is excellent and the mechanism (NK and macrophage clearance enhancement combined with downregulation of chronic inflammatory cytokines) is plausible.
For patients with frank lymphocyte deficiencies or chronic viral infection requiring antiviral therapy, Andrographis is supportive rather than primary — the underlying condition needs separate management.
Cautions (Including Transplant and Immunosuppressant Interactions)
- Pregnancy — absolute contraindication. Uterine-stimulant activity, abortifacient potential in animal studies, listed as contraindicated by every major regulatory body. Reiterated on every Andrographis page.
- Solid organ transplant recipients on immunosuppression — do not use Andrographis. Its immune-restoring activity may oppose the deliberate immunosuppression required to prevent graft rejection. Includes patients on tacrolimus, cyclosporine, mycophenolate, sirolimus, prednisone for transplant maintenance.
- Autoimmune patients on biologic anti-TNF therapy (infliximab, adalimumab, etanercept, golimumab, certolizumab) — theoretical concern about additive immunosuppression. Discuss with the rheumatologist or gastroenterologist before adding Andrographis. The mechanistic profile is somewhat complementary rather than redundant, but the combination has not been adequately studied.
- Autoimmune patients on conventional DMARDs (methotrexate, sulfasalazine, hydroxychloroquine, leflunomide) — Andrographis is mechanistically complementary and the combination has been used safely in IBD trials and rheumatoid arthritis trials. Reasonable to add Andrographis with physician awareness.
- Hematologic malignancy or active cancer therapy — complex. Andrographolide has documented anticancer activity in cell-culture and animal models but pharmacokinetic interactions with chemotherapy drugs are largely unstudied. Avoid during active chemotherapy unless oncologist concurs.
- Anticoagulant interaction — Andrographis modestly potentiates warfarin and other anticoagulants. Use cautiously, monitor INR, discontinue 7 days before elective surgery.
- Pediatric autoimmune disease — safety in pediatric autoimmune populations not well established. Use only with pediatric rheumatology / gastroenterology guidance.
- Bitter taste and gastric upset — standard tolerability issues, manageable with capsule form, food, and divided dosing.
Key Research Papers
- Burgos RA, Hancke JL, Bertoglio JC, et al. (2009). Efficacy of an Andrographis paniculata composition for the relief of rheumatoid arthritis symptoms: a prospective randomized placebo-controlled trial. Clinical Rheumatology. — PubMed
- Sandborn WJ, Targan SR, Byers VS, et al. (2013). Andrographis paniculata extract (HMPL-004) for active ulcerative colitis. American Journal of Gastroenterology. — PubMed
- Tang T, Targan SR, Li ZS, et al. (2011). Randomised clinical trial: herbal extract HMPL-004 in active ulcerative colitis — a double-blind comparison with sustained-release mesalazine. Alimentary Pharmacology & Therapeutics. — PubMed
- Iruretagoyena MI, Tobar JA, Gonzalez PA, et al. (2005). Andrographolide interferes with T cell activation and reduces experimental autoimmune encephalomyelitis in the mouse. Journal of Pharmacology and Experimental Therapeutics. — PubMed
- Kumar RA, Sridevi K, Kumar NV, et al. (2004). Anticancer and immunostimulatory compounds from Andrographis paniculata. Journal of Ethnopharmacology. — PubMed
- Sheeja K, Kuttan G (2007). Activation of cytotoxic T lymphocyte responses and attenuation of tumor growth in vivo by Andrographis paniculata extract and andrographolide. Immunopharmacology and Immunotoxicology. — PubMed
- Wang T, Liu B, Zhang W, et al. (2004). Andrographolide reduces inflammation-mediated dopaminergic neurodegeneration in mesencephalic neuron-glia cultures by inhibiting microglial activation. Journal of Pharmacology and Experimental Therapeutics. — PubMed
- Carretta MD, Alarcon P, Jara E, et al. (2009). Andrographolide reduces IL-2 production in T-cells by interfering with NFAT and MAPK activation. European Journal of Pharmacology. — PubMed
- Hidalgo MA, Hancke JL, Bertoglio JC, Burgos RA (2013). Andrographolide a new potential drug for the long term treatment of rheumatoid arthritis disease. Innovative Rheumatology. — PubMed
- Calabrese C, Berman SH, Babish JG, et al. (2000). A phase I trial of andrographolide in HIV positive patients and normal volunteers. Phytotherapy Research. — PubMed
- Kumar S, Singh B, Bajpai V (2021). Andrographis paniculata (Burm. f.) Nees: traditional uses, phytochemistry, pharmacological properties and quality control / quality assurance. Journal of Ethnopharmacology. — PubMed
- Mussard E, Cesaro A, Lespessailles E, et al. (2019). Andrographolide, a natural antioxidant: an update. Antioxidants. — PubMed
PubMed Topic Searches
- PubMed: Andrographolide immunomodulation
- PubMed: HMPL-004 UC trials
- PubMed: Andrographolide Th17/Treg autoimmune
- PubMed: Andrographolide T-cell signaling
- PubMed: Andrographis immune modulation
Connections
- Andrographis Overview
- Andrographis Benefits Hub
- Andrographis for Cold & Flu
- Andrographis for Liver Protection
- Andrographis Anti-Inflammatory
- Echinacea
- Astragalus
- Turmeric
- Japanese Knotweed
- Immune Boosting
- Ulcerative Colitis
- Crohn's Disease
- Arthritis
- Vitamin D3
- Zinc
- All Herbs