Tuna: Omega-3 vs Mercury Trade-Off
Every can of tuna delivers two things in the same bite: long-chain omega-3 fatty acids (EPA and DHA) that the cardiovascular and central nervous systems require, and methylmercury that the marine food web concentrated from coal-fired power plant emissions. The trade-off is not philosophical — it is quantitative. The 2021 FDA/EPA joint advisory translates the trade-off into weekly serving caps that differ for adults, pregnant women, and children, and that differ by tuna species by a factor of three or more. Two pivotal cohort studies (the Faroe Islands and the Seychelles) drew opposite conclusions about prenatal mercury harm at typical fish-eating exposures; the resolution involves understanding co-exposure to PCBs in pilot whale meat and the selenium-rich nature of ocean fish. This deep-dive walks through the numbers, the trials, and the practical heuristics for an evidence-based personal decision.
Table of Contents
- The Two Substances in Every Bite
- EPA and DHA: Mechanism and Clinical Effects
- Methylmercury: Mechanism and Neurotoxicity
- The 2021 FDA / EPA Joint Advisory
- Faroese vs Seychelles: Two Cohorts, Two Conclusions
- Selenium-Mercury Antagonism
- The Hair Mercury Test as Biomarker
- Practical Heuristics by Population
- Key Research Papers
- Connections
- Featured Videos
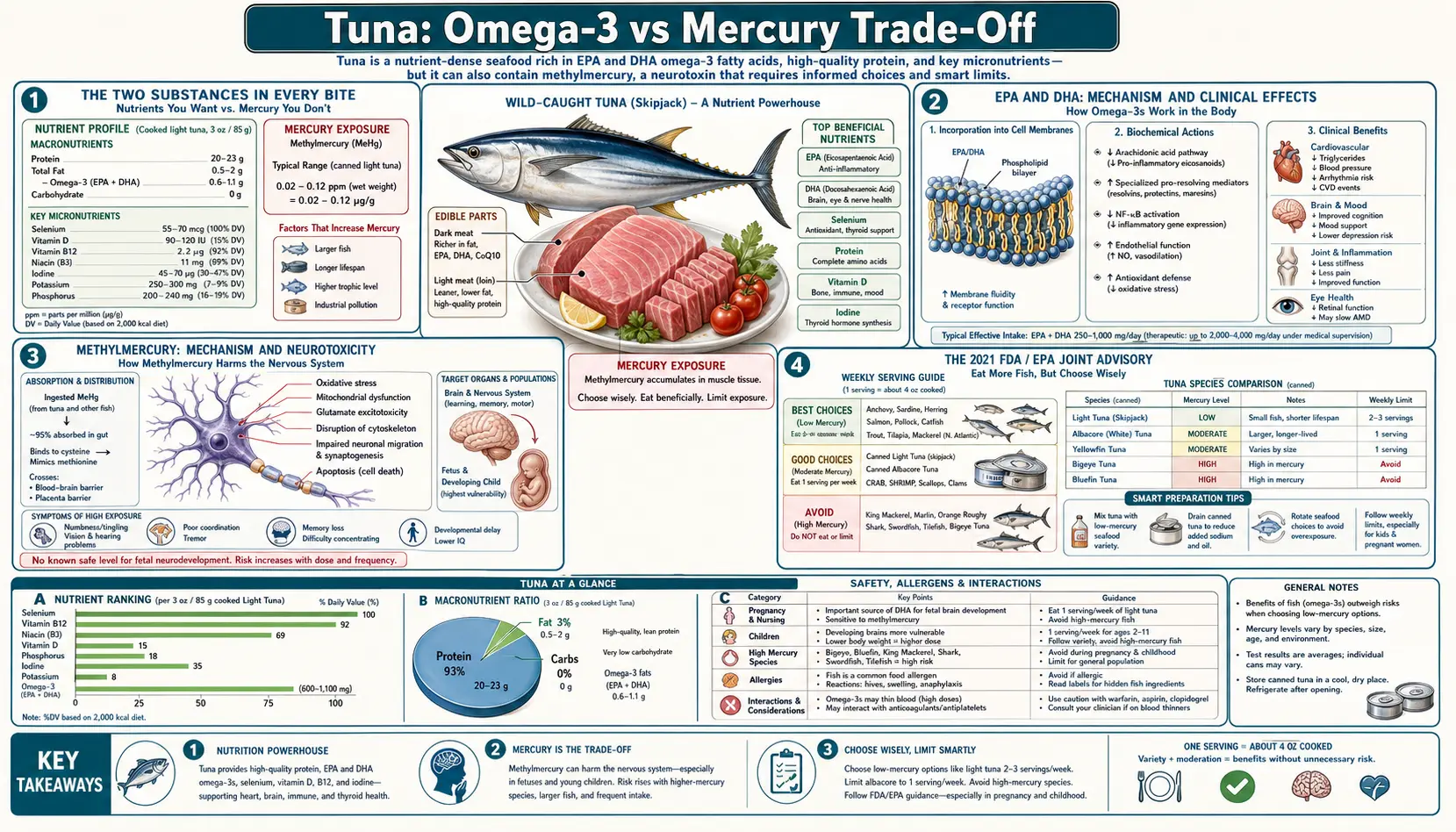
The Two Substances in Every Bite
A 3-oz serving of canned light tuna in water contains approximately:
- Omega-3 fatty acids (EPA + DHA): 230-280 mg
- Methylmercury: 35-45 µg (based on average skipjack mercury concentration ~0.13 ppm)
- Selenium: 60-90 µg (substantially exceeding mercury on a molar basis)
- Protein: 22 g complete protein
The same 3-oz serving of canned white (albacore) tuna contains:
- Omega-3 fatty acids (EPA + DHA): 700-800 mg (~3× light)
- Methylmercury: 100-110 µg (based on average albacore mercury concentration ~0.36 ppm; ~3× light)
- Selenium: 60-90 µg (similar to light)
- Protein: 21 g complete protein
The math is not coincidental: a longer-lived larger predatory fish (albacore reaches 6-9 years and 60 lb; skipjack lives ~4-5 years and rarely exceeds 30 lb) accumulates both lipid-soluble omega-3 and methylmercury at roughly proportional rates. The omega-3 advantage of albacore is real, and so is the mercury penalty. The question is which side of the ledger weighs more for the consumer in front of you, and the answer depends on whether that consumer is a pregnant woman, a child under 11, or an adult outside those categories.
For a side-by-side species comparison including yellowfin and bluefin, see Light vs Albacore.
EPA and DHA: Mechanism and Clinical Effects
Eicosapentaenoic acid (EPA, 20:5n-3) and docosahexaenoic acid (DHA, 22:6n-3) are 20- and 22-carbon polyunsaturated fatty acids with five and six double bonds respectively. They are not strictly "essential" in the chemical sense (the body can theoretically synthesize them from the plant-source precursor alpha-linolenic acid, ALA), but the conversion is so inefficient in humans — less than 5% of dietary ALA reaches EPA, less than 0.5% reaches DHA — that practical adequacy depends on direct dietary intake or supplementation.
EPA and DHA serve at least four distinct biochemical roles:
- Membrane phospholipid composition — DHA in particular is highly concentrated in retinal photoreceptors and synaptic membranes in the brain. DHA is roughly 30-40% of the fatty acids in the gray matter of the prefrontal cortex.
- Eicosanoid substrate competition — EPA competes with arachidonic acid (the omega-6 precursor) for cyclooxygenase and lipoxygenase enzymes, producing series-3 prostaglandins and series-5 leukotrienes that are markedly less inflammatory than the series-2 and series-4 derivatives of arachidonic acid.
- Specialized pro-resolving mediators — EPA and DHA are substrates for resolvins, protectins, and maresins — lipid mediators that actively turn off acute inflammation rather than merely failing to start it. This is a distinct mechanism from anti-inflammatory drug action.
- Triglyceride-lowering via PPAR-alpha — pharmacologic doses (2-4 g/day) reduce serum triglycerides by 25-30% via PPAR-alpha activation in the liver.
The clinical evidence ladder is well-established: the AHA recommends 2 servings of fatty fish per week for primary prevention based on the GISSI-Prevenzione, JELIS, and pooled meta-analyses. The REDUCE-IT trial (Bhatt 2019 NEJM) showed a 25% relative-risk reduction in cardiovascular events with icosapent ethyl (pure EPA) 4 g/day in statin-treated patients with elevated triglycerides. For the broader omega-3 story including supplementation strategy, see Omega-3 Fatty Acids.
Methylmercury: Mechanism and Neurotoxicity
Mercury exists in three environmentally relevant forms: elemental (Hg-0), inorganic (Hg-2+ salts), and organic methylmercury (CH3-Hg+). The form that matters for tuna consumption is methylmercury, which is biosynthesized by sulfate-reducing bacteria in sediment from inorganic mercury deposited from atmospheric coal combustion emissions. Once in the marine food web, methylmercury bioaccumulates — each trophic level concentrates it roughly 10-fold over its prey, so a 4-trophic-level predator like tuna ends up with mercury concentrations 10,000× the seawater background.
Methylmercury is highly bioavailable: 95%+ is absorbed from the gut, vs ~10% for inorganic mercury salts. Once absorbed, methylmercury crosses two critical barriers that inorganic mercury does not:
- Blood-brain barrier — methylmercury complexes with the amino acid cysteine to form a structural analog of methionine, which is then transported across the BBB by the large-neutral amino acid transporter (LAT1).
- Placenta — methylmercury reaches the fetal circulation at concentrations equal to or greater than maternal blood, and accumulates in the developing fetal brain.
Inside cells, methylmercury binds with extraordinarily high affinity to thiol (-SH) groups, particularly cysteine residues on selenoproteins, on glutathione, and on tubulin. The dominant mechanism of neurotoxicity is currently thought to be inhibition of selenium-dependent antioxidant enzymes (glutathione peroxidase, thioredoxin reductase) in neurons, leading to oxidative stress and disruption of microtubule-dependent neuronal migration during fetal brain development.
Adult exposure at the levels typical of US fish consumers does not produce frank Minamata-disease-like symptoms (those required the much higher industrial methylmercury exposures of Minamata, Japan in the 1950s). The concerns at typical exposure are subtler: subclinical paresthesias, fine-motor coordination decrements measurable on neuropsychological testing, and possibly cardiovascular effects (a Finnish cohort found increased acute coronary events at the highest mercury exposure quartile). For more on mercury toxicology generally, see Mercury.
The 2021 FDA / EPA Joint Advisory
The current US guidance is the 2021 joint advisory from the FDA and EPA, which organizes commercial fish into three categories:
- "Best Choices" (2-3 servings per week): canned light tuna, salmon, sardines, anchovies, herring, tilapia, cod, catfish, shrimp, scallops, oysters — 70+ species total. Mercury concentration generally below 0.15 ppm.
- "Good Choices" (1 serving per week): canned white (albacore) tuna, fresh tuna (yellowfin), halibut, sea bass, snapper, mahi-mahi, monkfish. Mercury 0.15-0.45 ppm.
- "Choices to Avoid" during pregnancy, lactation, and for children: swordfish, shark, king mackerel, tilefish from the Gulf of Mexico, bigeye tuna, marlin, orange roughy. Mercury >0.45 ppm.
For canned tuna specifically:
- Adults (not pregnant or lactating): 2-3 servings/week of canned light tuna OR 1 serving/week of canned white (albacore) tuna OR a mix.
- Pregnant or lactating women: Up to 12 oz/week (3-4 servings) of canned light tuna, OR up to 4 oz/week (1 serving) of albacore. Avoid bigeye and bluefin entirely.
- Children 1-3: 1 oz/week of canned light tuna (one-third of an adult serving). Avoid albacore for children under 4.
- Children 4-7: 2 oz/week of canned light tuna OR 1 oz/week of albacore.
- Children 8-10: 2.5 oz/week.
- Children 11+: Adult portions.
The advisory explicitly notes that fish should not be eliminated from the diet of pregnant women or children — the omega-3 benefit for fetal neurodevelopment and childhood cognition outweighs the mercury risk when species selection follows the advisory. The Hibbeln ALSPAC analysis (2007 Lancet) demonstrated this clearly: maternal seafood intake above the FDA's then-recommended 12 oz/week cap was associated with better child neurocognitive outcomes at age 8, not worse.
Faroese vs Seychelles: Two Cohorts, Two Conclusions
The methylmercury-and-fetal-neurodevelopment literature is dominated by two large cohort studies that arrived at opposite conclusions and shaped two decades of regulatory debate.
The Faroe Islands Children's Health Study (Philippe Grandjean and colleagues, University of Southern Denmark, 1986 onward) followed approximately 1,000 Faroese children from birth. The Faroese diet is unusual: in addition to ocean fish, the population consumes pilot whale meat at substantial frequency. Pilot whale is highly contaminated with both methylmercury and persistent organic pollutants (PCBs and chlorinated pesticides). The Faroese cohort found dose-dependent neurodevelopmental decrements at age 7 (language, attention, memory) associated with prenatal mercury exposure measured in maternal hair and cord blood.
The Seychelles Child Development Study (Philip Davidson, Gary Myers and colleagues, University of Rochester, 1989 onward) followed approximately 700 children in the Republic of Seychelles, where ocean fish consumption averages 12 meals per week (vs ~2/week in the US). The Seychellois cohort found no association between prenatal mercury exposure and neurodevelopmental outcomes at multiple time points (24 months, 5.5 years, 9 years, 17 years).
The differences between the two cohorts are now understood as the explanation for the discrepancy:
- Co-exposure differences — Faroese children had substantial co-exposure to PCBs (from pilot whale blubber) that the Seychellois did not. PCBs are independent neurodevelopmental toxicants.
- Mercury exposure pattern — the Faroese had peak mercury exposures coinciding with pilot whale hunts (intermittent high doses); the Seychellois had steady daily fish-meal exposure (lower peaks).
- Nutritional context — the Seychellois cohort was eating ocean fish rich in selenium and omega-3 fatty acids, both of which appear to mitigate mercury neurotoxicity. The pilot whale meat in the Faroese diet does not have the same omega-3 profile.
The current synthesis (NRC 2000 report, EPA 2002, EFSA 2012) is that the Faroese results probably represent the worst-case exposure pattern, the Seychellois results represent the typical-fish-diet pattern, and the truth for US consumers eating ocean fish (not pilot whale) is closer to the Seychellois finding. The EPA Reference Dose of 0.1 µg methylmercury/kg/day is conservatively derived from the Faroese data with a 10× uncertainty factor.
Selenium-Mercury Antagonism
Selenium and mercury have an extraordinarily high binding affinity for each other — the formation constant for selenium-mercury complexes exceeds that of any other biologically relevant metal-mineral interaction. This has practical implications.
Methylmercury exerts most of its toxicity by binding to and inhibiting selenoenzymes (glutathione peroxidase, thioredoxin reductase, iodothyronine deiodinase). When dietary selenium is abundant, two protective mechanisms operate:
- Selenium intercepts methylmercury directly, forming biologically inert HgSe (mercury selenide) complexes that are sequestered and excreted without disrupting selenoenzyme function.
- Adequate dietary selenium supports replacement synthesis of selenoenzymes faster than methylmercury can inhibit them.
Ocean fish, including tuna, are unusually selenium-rich — the molar selenium content of nearly every ocean fish species exceeds its mercury content, often by a factor of 3-10. This is the basis for the "selenium health benefit value" (HBV-Se) proposed by Nicholas Ralston and Laura Raymond: an index defined as (Se-Hg)/Se, with positive values indicating net selenium surplus. By this index, skipjack, salmon, sardines, and most ocean fish have strongly positive HBV-Se values, while tilefish, swordfish, shark, and pilot whale have negative values (mercury exceeds selenium on a molar basis).
The HBV-Se framework is not currently used by FDA in advisories (which are based on total mercury), but it explains why the Seychelles cohort, eating mostly small-to-medium ocean fish, showed no neurodevelopmental harm despite mercury exposures that would have been concerning under a mercury-only framework. For more on selenium itself, see Selenium.
The Hair Mercury Test as Biomarker
For consumers (or clinicians) who want to verify that fish consumption is staying within safe limits, hair mercury testing is the standard biomarker. Hair grows approximately 1 cm/month and incorporates methylmercury into the keratin matrix at roughly 250× the steady-state blood concentration. A 1-cm hair segment closest to the scalp reflects approximately the previous month's exposure; longer segments give a longitudinal record.
Reference values for hair mercury:
- <1 µg/g — typical for low fish consumers in the US
- 1-2 µg/g — moderate fish consumer; well within EPA RfD-derived safety
- 2-5 µg/g — heavy fish consumer; approaching but not exceeding the EPA-derived safety threshold of approximately 4-5 µg/g in hair
- >5 µg/g — exceeds the EPA RfD-derived hair threshold; reduce high-mercury fish intake (swordfish, shark, tilefish, bigeye tuna, marlin) and recheck in 3-6 months
- >10 µg/g — substantial exceedance; clinical evaluation, complete dietary mercury restriction, and consideration of DMSA chelation in symptomatic cases
For pregnant women, the WHO benchmark for fetal effects is approximately 11 µg/g in maternal hair, with a 10× safety factor giving a target of <1 µg/g pre-conception and during pregnancy. Most US women fall below 1 µg/g; women who eat sushi-grade tuna or swordfish more than once a week sometimes exceed it.
Hair mercury testing is available through commercial labs (Quicksilver Scientific, Doctor's Data, Mosaic Diagnostics) for $30-100. Blood mercury is faster-responding (half-life ~50 days) but less stable. Whole-blood mercury >5.8 µg/L is the CDC-defined elevation threshold. For mercury testing options and interpretation, see Lab Tests.
Practical Heuristics by Population
- Average adult, not pregnant: 2-3 cans of light tuna per week is well within safety margins and provides ~700 mg/week omega-3. Substituting one albacore can in that mix increases omega-3 (~700 mg from one albacore) but also approximately doubles mercury intake. Either pattern is reasonable.
- Pregnant or trying to conceive: Stay strictly within the 12-oz light tuna OR 4-oz albacore per week guidance. Consider a hair mercury test pre-conception and at 12-16 weeks gestation. Aim for <1 µg/g.
- Children under 11: Use the age-specific limits in the FDA/EPA advisory (1-2.5 oz/week of light tuna). Avoid albacore for children under 4. Variety across low-mercury fish (salmon, sardines, anchovies, shrimp) is preferable to relying on tuna.
- Heavy sushi consumer (yellowfin, bluefin, bigeye 3+ times per week): Hair mercury test recommended. Most heavy sushi eaters fall in the 2-5 µg/g range; some exceed 10 µg/g and should reduce intake.
- Anyone with autoimmune disease, kidney disease, or unexplained neurological symptoms: Hair mercury test is reasonable as part of a broader workup, though mercury is rarely the primary driver.
- Concerned about both mercury and omega-3: Skipjack-only canned light tuna gives the best benefit/risk ratio of any tuna option. Salmon (wild Pacific or farmed Atlantic, both low-mercury, high-omega-3) and sardines are strong alternatives. EPA/DHA from a high-quality fish oil or algal oil supplement (mercury removed during manufacture) eliminates the trade-off entirely for the omega-3 portion of the diet.
For broader cardiovascular and cognitive context, see Cardiology and Neurology.
Key Research Papers
- Mozaffarian D, Rimm EB (2006). Fish intake, contaminants, and human health: evaluating the risks and the benefits. JAMA 296(15):1885-99. — PubMed PMID 17047219
- Hibbeln JR et al. (2007). Maternal seafood consumption in pregnancy and neurodevelopmental outcomes in childhood (ALSPAC study): an observational cohort study. Lancet 369(9561):578-85. — PubMed PMID 17307104
- Grandjean P et al. (1997). Cognitive deficit in 7-year-old children with prenatal exposure to methylmercury. Neurotoxicology and Teratology 19(6):417-28. — PubMed PMID 9392777
- Davidson PW et al. (1998). Effects of prenatal and postnatal methylmercury exposure from fish consumption on neurodevelopment: outcomes at 66 months of age in the Seychelles Child Development Study. JAMA 280(8):701-7. — PubMed PMID 9728641
- Myers GJ et al. (2003). Prenatal methylmercury exposure from ocean fish consumption in the Seychelles child development study. Lancet 361(9370):1686-92. — PubMed PMID 12767734
- Ralston NVC, Raymond LJ (2010). Dietary selenium's protective effects against methylmercury toxicity. Toxicology 278(1):112-23. — PubMed PMID 20561558
- Karimi R et al. (2014). A quantitative synthesis of mercury in commercial seafood and implications for exposure in the United States. Environmental Health Perspectives 122(11):1183-1188. — Search PubMed
- Mahaffey KR et al. (2011). Balancing the benefits of n-3 polyunsaturated fatty acids and the risks of methylmercury exposure from fish consumption. Nutrition Reviews 69(9):493-508. — PubMed PMID 21884130
- Strain JJ et al. (2008). Associations of maternal long-chain polyunsaturated fatty acids, methyl mercury, and infant development in the Seychelles Child Development Nutrition Study. Neurotoxicology 29(5):776-82. — PubMed PMID 18590765
- Choi AL et al. (2009). Methylmercury exposure and adverse cardiovascular effects in Faroese whaling men. Environmental Health Perspectives 117(3):367-72. — PubMed PMID 19337510
- Salonen JT et al. (1995). Intake of mercury from fish, lipid peroxidation, and the risk of myocardial infarction. Circulation 91(3):645-55. — PubMed PMID 7828289
- Bhatt DL et al. (2019). Cardiovascular risk reduction with icosapent ethyl for hypertriglyceridemia (REDUCE-IT). NEJM 380(1):11-22. — PubMed PMID 30415628
PubMed Topic Searches
- PubMed: Tuna omega-3 vs mercury
- PubMed: Methylmercury and neurodevelopment
- PubMed: Selenium-mercury antagonism
- PubMed: FDA/EPA fish advisory
- PubMed: Hair mercury biomarker
Connections
- Tuna (Main Page)
- Tuna Benefits Hub
- Lean Protein Profile
- Light vs Albacore
- Sustainability
- Omega-3 Fatty Acids
- Mercury (Toxin)
- Selenium
- Salmon
- Sardines
- Herring
- Cod
- Cardiology
- Neurology
- Lab Tests