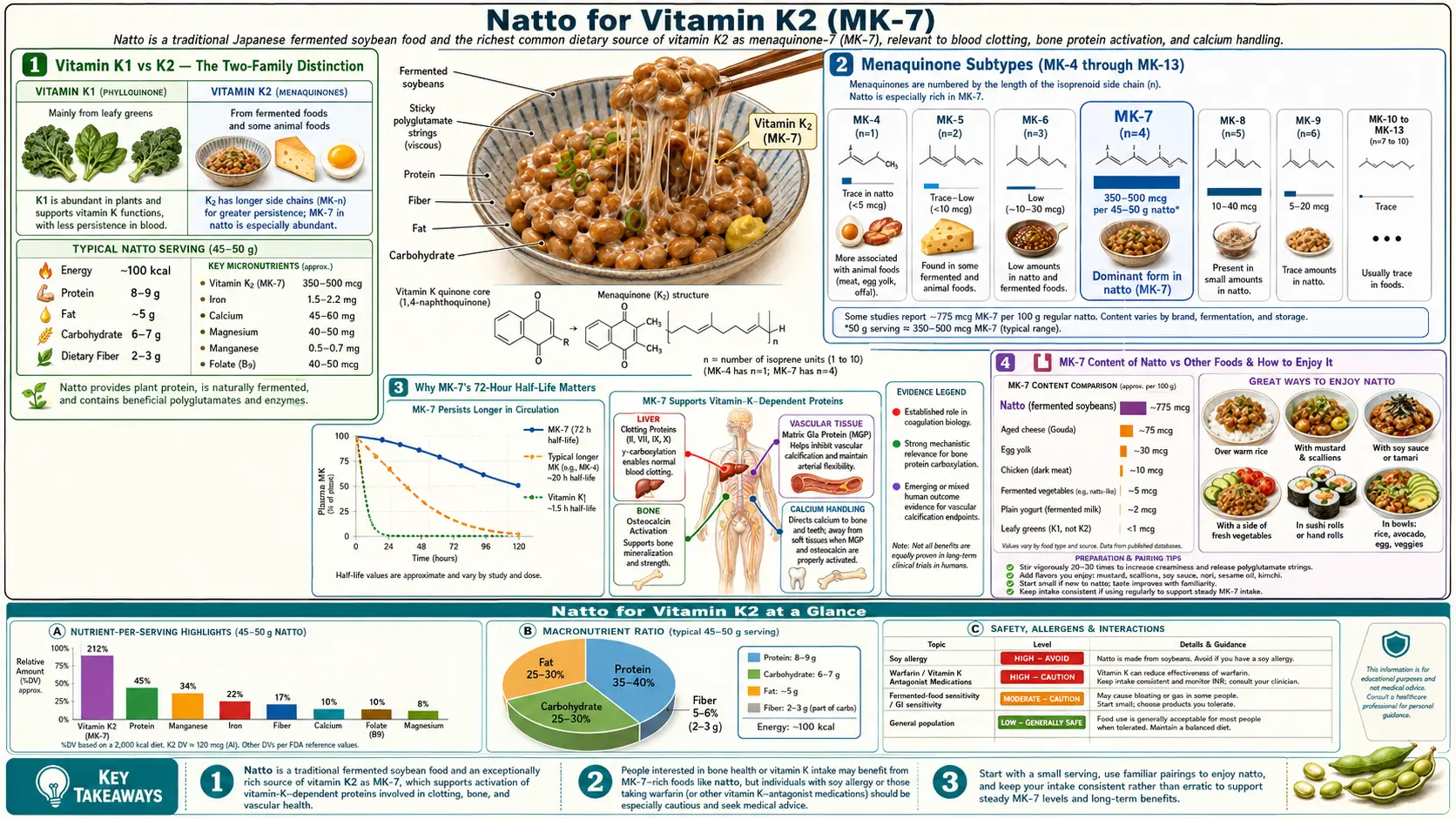
Natto for Vitamin K2 (MK-7)
A single 50-gram serving of natto delivers approximately 500 micrograms of menaquinone-7 (MK-7) — roughly five times the upper-tier dose used in published clinical trials, and two to three orders of magnitude more bioavailable Vitamin K2 than any other natural food. The seven-isoprene side chain that defines MK-7 produces a 72-hour serum half-life (versus 1-2 hours for the MK-4 form found in butter, egg yolk, and liver), enough to maintain steady-state gamma-carboxylation of osteocalcin in bone and matrix Gla protein in the arterial wall on once-daily food intake. This page walks through the menaquinone biochemistry that makes MK-7 unique, the Rotterdam Study and Beulens coronary-calcification data, the Knapen postmenopausal bone trials, dosing equivalence between food natto and isolated MK-7 supplements, and the warfarin interaction that requires careful management.
Table of Contents
- Vitamin K1 vs K2 — The Two-Family Distinction
- Menaquinone Subtypes (MK-4 through MK-13)
- Why MK-7's 72-Hour Half-Life Matters
- MK-7 Content of Natto vs Other Foods
- Osteocalcin Gamma-Carboxylation (Bone Mineralization)
- Matrix Gla Protein (Arterial Calcification Prevention)
- Rotterdam Study and Coronary Heart Disease
- Dosing — Food vs Supplement Equivalence
- Warfarin Interaction (Critical Caution)
- Key Research Papers
- Connections
- Featured Videos
Vitamin K1 vs K2 — The Two-Family Distinction
Vitamin K is not a single molecule but a family of structurally related naphthoquinone compounds, divided into two principal subgroups. Vitamin K1 (phylloquinone) is synthesized by plants and is the dominant form in green leafy vegetables — kale, spinach, collards, broccoli. K1 has a single phytyl side chain and is involved primarily in the synthesis of hepatic clotting factors II, VII, IX, and X. Most dietary K intake in Western populations is K1.
Vitamin K2 (menaquinone) is synthesized by bacteria, including the bacteria in fermented foods and the symbiotic flora of the human large intestine. The K2 side chain is an isoprenoid (rather than a saturated phytyl chain), and the number of isoprene units defines the specific menaquinone subtype — MK-4 has four units, MK-7 has seven, MK-9 has nine, and so on. Different bacteria produce different menaquinone subtypes; the Bacillus subtilis var. natto strain used in natto fermentation is unusually efficient at producing MK-7 specifically.
The clinical significance is that K1 and K2 are not freely interconvertible in human tissue. The liver preferentially takes up K1 for clotting-factor synthesis, leaving little K1 available for extra-hepatic tissues. K2 (particularly the long-chain MK-7 form) escapes hepatic first-pass uptake and reaches osteocalcin in bone osteoblasts and matrix Gla protein in arterial smooth muscle cells. This is why supplementing K1 alone — or eating only leafy greens — produces only limited extra-hepatic Vitamin K-dependent protein activation, while supplementing K2 (or eating natto) produces robust activation of bone and arterial proteins.
The 2012 Theuwissen study quantified this directly: 180 micrograms per day of MK-7 fully activated extra-hepatic osteocalcin within 8 weeks in healthy adults, while equivalent doses of K1 did not, despite raising plasma phylloquinone levels.
Menaquinone Subtypes (MK-4 through MK-13)
Within the K2 menaquinone family, the side-chain length determines pharmacokinetics. Short-chain menaquinones are absorbed and cleared rapidly; long-chain menaquinones persist much longer in circulation.
- MK-4 (menatetrenone) — four isoprene units. Found in animal products: butter, egg yolk, liver, chicken. Half-life is approximately 1-2 hours. MK-4 can also be synthesized endogenously from K1 by conversion in peripheral tissues, particularly testes and arterial wall. Used pharmaceutically in Japan as menatetrenone (Glakay) at 45 mg/day for osteoporosis — a dose roughly 200 times higher than dietary MK-7 because of the short half-life.
- MK-7 — seven isoprene units. The dominant form in natto and in lesser quantities in some hard cheeses (Gouda, Edam) and in fermented dairy. Half-life approximately 72 hours. The long half-life means once-daily intake at modest doses (90-200 µg) maintains steady-state extra-hepatic activation.
- MK-9, MK-10, MK-11 — longer chains produced by some gut bacteria and present in trace amounts in fermented foods. Half-lives are similar to or longer than MK-7. The clinical evidence base is smaller because most trials have used MK-7 specifically.
- MK-13 — the longest naturally occurring menaquinone, produced by certain mycobacteria. Not relevant to nutrition.
Natto contains all three biologically significant menaquinones to varying degrees but is overwhelmingly dominated by MK-7. Schurgers and Vermeer's 2000 food-content analysis found natto contained approximately 998 µg MK-7 per 100 g, dwarfing all other tested foods. Gouda cheese, the next-highest food source, contained about 75 µg MK-7 per 100 g — over 13 times less. Hard egg yolk contained about 32 µg, and chicken liver about 9 µg.
Why MK-7's 72-Hour Half-Life Matters
The pharmacokinetic profile of a Vitamin K subtype determines whether dietary or supplemental intake can maintain steady-state activation of the Vitamin K-dependent extra-hepatic proteins (osteocalcin, matrix Gla protein, Gas6, periostin, and others). Activation requires the gamma-carboxylase enzyme to add a carboxyl group to specific glutamic acid residues, converting them to gamma-carboxyglutamate (Gla) residues. The Gla residues then bind calcium and execute the protein's biological function.
A Vitamin K subtype with a 1-2 hour half-life (like MK-4 or K1) is largely cleared from circulation within 4-8 hours of intake. To maintain steady-state gamma-carboxylation, the dose must be either very large (the Japanese 45 mg/day menatetrenone regimen) or split across multiple daily doses, neither of which is realistic for dietary intake.
MK-7's 72-hour half-life inverts this calculation. A single daily intake of 50 g natto (~500 µg MK-7) produces a serum MK-7 concentration that remains in the activation range for approximately three days. Even intake every 2-3 days maintains continuous gamma-carboxylation of bone and arterial Gla proteins. This is the pharmacokinetic foundation for why natto-eating populations achieve full activation of extra-hepatic Vitamin K-dependent proteins while populations relying on K1 from leafy greens or MK-4 from animal foods do not.
The Sato 2012 head-to-head bioavailability comparison made this dramatically explicit: 420 µg of MK-7 produced 7-8 times higher peak serum concentration and 10 times longer area-under-curve than the equivalent dose of MK-4, despite identical molar quantities. The same dose-response gradient is observed when MK-7 is given as the food natto versus as a synthetic supplement — bioavailability is similar, indicating the bacterial fermentation matrix does not impede absorption.
MK-7 Content of Natto vs Other Foods
For context, the following table summarizes approximate MK-7 content of major foods (data from Schurgers & Vermeer 2000 and subsequent food-composition databases):
- Natto, fermented soybean (Japan) — ~1,000 µg per 100 g (highest food source by an order of magnitude)
- Gouda cheese (aged) — ~75 µg per 100 g
- Edam cheese — ~65 µg per 100 g
- Hard cheese (Cheddar, Parmigiano) — ~40-50 µg per 100 g
- Soft cheese (Camembert, Brie) — ~50-60 µg per 100 g
- Egg yolk (chicken) — ~32 µg per 100 g
- Chicken liver — ~9 µg per 100 g (mostly MK-4, modest MK-7)
- Butter — ~15 µg per 100 g (predominantly MK-4)
- Whole milk — trace amounts
The 100× concentration of natto over the next-highest food source is the practical reason that Japanese populations — particularly the eastern Kanto, Tohoku, and Hokkaido regions where natto consumption is highest — achieve serum MK-7 levels 4-6 times higher than Westerners, even those eating cheese-heavy diets. The Kaneki 2001 study (covered on the Bone Density deep dive) used this regional gradient to demonstrate the inverse correlation between MK-7 intake and hip fracture incidence across Japanese prefectures.
The practical takeaway: 30-50 grams of natto per day (one to two store-bought packets, or one tablespoon to two tablespoons of the homemade ferment) supplies more than enough MK-7 to saturate gamma-carboxylation of extra-hepatic Vitamin K-dependent proteins.
Osteocalcin Gamma-Carboxylation (Bone Mineralization)
Osteocalcin is a small protein secreted by osteoblasts (bone-building cells). It contains three glutamic acid residues that must be gamma-carboxylated to function properly. In its carboxylated form (cOC), osteocalcin binds calcium ions and orients them on the hydroxyapatite crystal lattice of newly forming bone, supporting orderly mineralization. In its undercarboxylated form (ucOC), osteocalcin cannot bind calcium and the calcium that would have been incorporated into bone instead remains in circulation, where it can be deposited inappropriately in soft tissues including arterial walls.
The ratio of ucOC to cOC (or, equivalently, serum ucOC level) is a sensitive marker of Vitamin K2 status. Postmenopausal women with the highest tertile of ucOC (indicating poor carboxylation) have approximately twice the hip fracture risk of women in the lowest tertile in longitudinal studies. MK-7 supplementation rapidly normalizes the ucOC ratio — the Inaba 2015 trial demonstrated that as little as 50 µg/day MK-7 produced a significant reduction in ucOC within 4 weeks, and 100-200 µg/day produced near-maximal activation.
The clinical relevance: serum ucOC (or undercarboxylated-to-total osteocalcin ratio) is a clinically available marker that can be ordered to assess Vitamin K2 status in patients with osteoporosis or osteopenia. An elevated ratio implies inadequate K2 and predicts a favorable response to MK-7 repletion (either via natto or supplemental MK-7).
See the Bone Density deep dive for the Knapen 3-year postmenopausal MK-7 trial and the regional Japanese hip fracture data.
Matrix Gla Protein (Arterial Calcification Prevention)
Matrix Gla protein (MGP) is the body's primary defense against vascular calcification. It is synthesized by vascular smooth muscle cells, secreted into the arterial wall extracellular matrix, and (when properly gamma-carboxylated) binds calcium ions before they can crystallize onto elastin fibers. The carboxylated form of MGP (cMGP) actively dissolves nascent calcium deposits in the arterial wall; the undercarboxylated form (ucMGP) is biologically inactive and permits calcification to proceed.
The clinical implication is dramatic. MGP-knockout mice develop massive arterial calcification within weeks of birth and die of aortic rupture before sexual maturity. Humans with severe MGP deficiency (Keutel syndrome) develop diffuse soft-tissue and cartilage calcification. Subclinical MGP undercarboxylation in the general population, driven by Vitamin K2 insufficiency, contributes to the progressive coronary and aortic calcification observed with aging.
The Beulens 2009 cross-sectional analysis (and the prospective Knapen 2015 trial) demonstrated that high MK-7 intake associates with reduced coronary artery calcification and that supplemental MK-7 actually improves arterial elasticity over 3 years. The mechanism is precisely the activation of MGP. The high-MK-7 group in the Beulens analysis had approximately 50% lower coronary calcification scores than the low-intake group, after adjustment for age, sex, smoking, blood pressure, lipid profile, and other cardiovascular risk factors.
This is the mechanistic basis for the combined "K2 plus D3 plus calcium" strategy advocated by integrative cardiologists: Vitamin D3 increases calcium absorption from the gut, Vitamin K2 (as MK-7) ensures that absorbed calcium is preferentially deposited in bone rather than artery. Without adequate K2, supplemental calcium and Vitamin D may increase the risk of arterial calcification — the concern raised by the WHI calcium supplementation analyses. With adequate K2 (whether from natto or from MK-7 supplements), this risk is largely eliminated.
See our pages on Atherosclerosis and Vitamin K2 for additional context.
Rotterdam Study and Coronary Heart Disease
The Rotterdam Study is a prospective Dutch cohort of approximately 4,800 individuals followed from 1990 onward for cardiovascular and other chronic disease outcomes. Geleijnse et al. analyzed dietary menaquinone intake (estimated from food-frequency questionnaires) against coronary heart disease incidence and mortality. After 7-10 years of follow-up, individuals in the highest tertile of menaquinone intake (median ~32 µg/day) had:
- Approximately 57% reduction in CHD-related mortality compared to the lowest tertile
- Approximately 26% reduction in all-cause mortality
- Approximately 52% reduction in severe aortic calcification on imaging
The effect was specific to menaquinone (K2) — phylloquinone (K1) intake showed no association with CHD outcomes in the same cohort. This was one of the first large prospective studies to demonstrate that the K1/K2 distinction has clinically meaningful consequences beyond simple coagulation.
The Gast 2009 follow-up analysis in a separate Dutch cohort (the Prospect-EPIC cohort, ~16,000 women) reinforced the finding: each 10 µg/day increase in menaquinone intake was associated with approximately 9% reduction in CHD incidence. The 2020 Haugsgjerd analysis in a Norwegian cohort and the 2021 Eriksen analysis in a Danish cohort both confirmed the inverse association in independent populations.
It is worth noting that the menaquinone intake levels in these European cohorts (15-45 µg/day) are an order of magnitude lower than what a regular natto consumer achieves (~500 µg/serving). If the dose-response relationship is roughly linear — and the bone density data suggest it may even be steeper at higher doses — the cardiovascular benefit of regular natto consumption is plausibly larger than what the European epidemiology demonstrates.
Dosing — Food vs Supplement Equivalence
For an adult seeking adequate Vitamin K2 (MK-7) intake for bone, arterial, and general extra-hepatic gamma-carboxylation:
- Food route: 30-50 g natto per day (one standard store-bought packet) supplies ~300-500 µg MK-7 — more than enough to saturate gamma-carboxylation. Eating natto every other day (50-100 g per serving every 48 hours) also maintains adequate steady-state due to the 72-hour half-life.
- Supplement route: 100-200 µg/day MK-7 (as menaquinone-7, often labeled MenaQ7 in commercial preparations) reproduces the activation observed in the Knapen, Inaba, and Theuwissen trials. Bioequivalence to dietary MK-7 from natto is approximately 1:1 in head-to-head bioavailability studies (Schurgers 2007).
- MK-4 route (Japanese pharmaceutical): 45 mg/day menatetrenone, divided into 3 doses, is the registered dose for osteoporosis in Japan. The dose is much larger because of the 1-2 hour MK-4 half-life; the activation produced is similar to 200 µg/day MK-7.
For combination supplementation with Vitamin D3 (typical for bone/cardiovascular use), a common regimen is 2,000-5,000 IU vitamin D3 plus 100-200 µg MK-7 per day, often combined into a single soft-gel capsule. Both are fat-soluble and should be taken with a meal containing fat.
For patients on warfarin, dosing requires explicit coordination with the prescribing physician — see the next section.
For comparison and broader context on Vitamin K2 supplementation, see our Vitamin K2 page.
Warfarin Interaction (Critical Caution)
Warfarin works by inhibiting the Vitamin K epoxide reductase complex (VKORC1), depleting the reduced Vitamin K available for the gamma-carboxylase enzyme. This reduces gamma-carboxylation of clotting factors II, VII, IX, and X, producing therapeutic anticoagulation. The same mechanism reduces gamma-carboxylation of osteocalcin and matrix Gla protein, which is why long-term warfarin therapy is associated with accelerated osteoporosis and accelerated arterial calcification.
Increased intake of Vitamin K (either K1 or K2) directly antagonizes warfarin's effect by providing more substrate for the partial residual gamma-carboxylase activity. The INR (international normalized ratio, the warfarin monitoring lab) drops when K intake rises and rises when K intake falls.
The specific implications for natto:
- Patients on warfarin should not start eating natto without explicit physician coordination. A 50 g serving of natto delivers 500 µg of MK-7, which is approximately 5 times the intake of a typical Western diet. Adding natto to a stable warfarin regimen can drop the INR substantially and require dose increase.
- Consistent intake is the key principle. If natto is part of the regular diet, INR can be stabilized at the appropriate warfarin dose; the problem is variability. Sporadic natto consumption (5 packets one week, none the next) is incompatible with stable warfarin management.
- The newer oral anticoagulants (apixaban, rivaroxaban, dabigatran) do not interact with Vitamin K and are increasingly preferred when long-term anticoagulation is required, in part to avoid this and other dietary interactions. Patients who can switch from warfarin to a direct oral anticoagulant gain dietary freedom around K-containing foods.
- The K2 supplementation case in patients on warfarin is sometimes made on the grounds that warfarin's harms to bone and artery are mediated by extra-hepatic Vitamin K deficiency that could be selectively repleted without affecting the hepatic clotting-factor effect. This is plausible mechanistically but requires careful dosing and INR monitoring; it is not a self-administered intervention.
For non-anticoagulated patients with active thromboembolic disease, see the separate Nattokinase deep dive, which addresses the fibrinolytic enzyme in natto rather than the K2.
Key Research Papers
- Schurgers LJ, Vermeer C (2000). Determination of phylloquinone and menaquinones in food. Haemostasis. — PubMed
- Schurgers LJ et al. (2007). Vitamin K-containing dietary supplements: comparison of synthetic K1 and natto-derived MK-7. Blood. — PubMed
- Sato T et al. (2012). Comparison of menaquinone-4 and menaquinone-7 bioavailability in healthy women. Nutrition Journal. — PubMed
- Geleijnse JM et al. (2004). Dietary intake of menaquinone is associated with a reduced risk of coronary heart disease (Rotterdam Study). J Nutr. — PubMed
- Gast GC et al. (2009). High menaquinone intake reduces incidence of coronary heart disease. Nutr Metab Cardiovasc Dis. — PubMed
- Beulens JW et al. (2009). High dietary menaquinone intake is associated with reduced coronary calcification. Atherosclerosis. — PubMed
- Knapen MH et al. (2013). Three-year low-dose MK-7 supplementation helps decrease bone loss in healthy postmenopausal women. Osteoporosis Int. — PubMed
- Knapen MH et al. (2015). MK-7 supplementation improves arterial stiffness in healthy postmenopausal women. Thromb Haemost. — PubMed
- Theuwissen E et al. (2013). Low-dose MK-7 supplementation improved extra-hepatic Vitamin K status. Br J Nutr. — PubMed
- Inaba N et al. (2015). Low-dose daily intake of MK-7 improves osteocalcin gamma-carboxylation. J Nutr Sci Vitaminol. — PubMed
- Schurgers LJ et al. (2008). Vitamin K-dependent carboxylation of matrix Gla protein. Thromb Haemost. — PubMed
- Halder M et al. (2019). Vitamin K: double bonds beyond coagulation. Int J Mol Sci. — PubMed
PubMed Topic Searches
- PubMed: MK-7 bioavailability
- PubMed: MGP arterial calcification
- PubMed: Undercarboxylated osteocalcin
- PubMed: Warfarin K2 interaction
- PubMed: K2 coronary heart disease
Connections
- Natto (Main Page)
- Natto Benefits Hub
- Nattokinase & Fibrinolysis
- Bone Density
- Acquired Taste Tips
- Vitamin K2
- Vitamin D3
- Vitamin A (RXR Partner)
- Calcium
- Magnesium
- Atherosclerosis
- Osteoporosis
- All Food
- Yogurt
- Probiotics