Lactose Intolerance — Lactase Persistence Genetics, Threshold Dose, and Workarounds
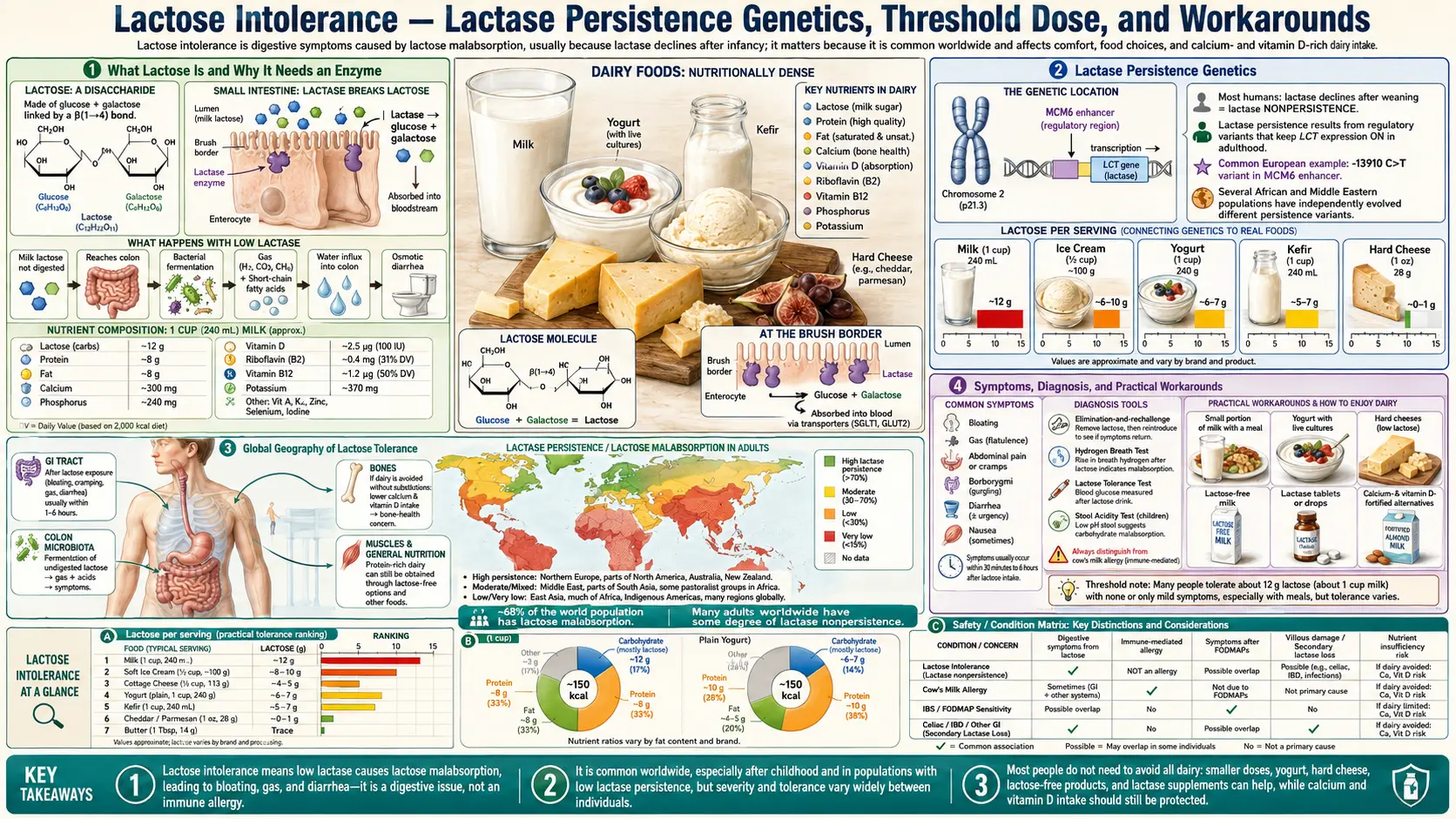
Lactose intolerance is one of the clearest examples of recent human evolution. The ancestral mammalian condition is that intestinal lactase — the enzyme that splits the milk sugar lactose into glucose and galactose — declines sharply after weaning, leaving most adult mammals unable to digest milk. In the past 10,000 years, at least four independent mutations in the regulatory region upstream of the LCT (lactase) gene have arisen in human populations with a tradition of dairying. The European −13910*T variant is now present in 95% of Scandinavians, 75% of British, 25% of West Africans, and 5% of East Asians. Adults without any lactase-persistence variant lose intestinal lactase expression after weaning and experience osmotic diarrhea, bloating, and flatulence above a threshold of approximately 12 grams of lactose per sitting. Most can tolerate yogurt, kefir, hard cheese, and small amounts of milk without issue.
Table of Contents
- What Lactose Is and Why It Needs an Enzyme
- Lactase Persistence Genetics
- Global Geography of Lactose Tolerance
- Symptoms and Diagnosis
- The Threshold Dose
- Why Fermented Dairy Works
- Lactose-Free Milk, Enzyme Pills, and Adaptation
- Primary vs Secondary Lactase Deficiency
- Lactose Intolerance Is Not Milk Allergy
- Research Papers
- External Resources
- Connections
- Featured Videos
1. What Lactose Is and Why It Needs an Enzyme
Lactose is a disaccharide of glucose and galactose joined by a beta-1,4-glycosidic bond. It is the dominant carbohydrate in mammalian milk — cow's milk contains roughly 4.7% lactose by weight, human milk roughly 7.0%, goat milk roughly 4.1%, sheep milk roughly 4.8%. A typical 240 mL (1 cup) serving of cow's milk delivers approximately 12 grams of lactose.
Like all disaccharides, lactose cannot be absorbed intact across the intestinal epithelium — the brush-border transporters that move sugars into enterocytes are specific to monosaccharides. To be useful as a nutrient, lactose must first be hydrolyzed into its constituent glucose and galactose by the enzyme lactase (also called lactase-phlorizin hydrolase, LPH, or beta-galactosidase). This enzyme is anchored to the brush border of the small intestinal enterocyte, with its active site facing the lumen. Glucose and galactose released by lactase hydrolysis are then absorbed by the SGLT1 (sodium-glucose cotransporter 1) transporter on the enterocyte apical membrane.
If lactase is absent or insufficient, unhydrolyzed lactose passes into the colon. There it is osmotically active (drawing water into the bowel and producing watery diarrhea) and it is fermented by colonic bacteria into short-chain fatty acids and gas (hydrogen, methane, and carbon dioxide), producing the bloating, abdominal pain, and flatulence characteristic of lactose intolerance.
2. Lactase Persistence Genetics
In all mammals, including humans, the LCT gene encoding lactase is highly expressed in the small intestinal enterocyte during infancy and then is normally downregulated around the time of weaning. In ancestral humans — and in roughly 65% of the present-day adult global population — this downregulation persists into adulthood, resulting in low or absent intestinal lactase by age 5-15.
The downregulation is mediated by the MCM6 regulatory region located roughly 14 kilobases upstream of the LCT gene on chromosome 2. The MCM6 region contains transcription factor binding sites that normally suppress LCT expression after weaning.
Several mutations in this regulatory region disrupt the suppression mechanism, leaving LCT expression high into adulthood and producing the "lactase persistence" trait. The most common in Europe is the −13910*T variant (a C-to-T substitution 13,910 bases upstream of LCT), identified by Enattah et al. in 2002 (PMID 11788828). Independent lactase-persistence mutations have arisen in:
- Northern Europe (−13910*T): approximately 95% of Scandinavians, 75% of British, 70% of Germans, 50% of Spanish/Italian, 5-10% of Greek
- East Africa (−13907*G, −14010*C, −13915*G): three independent variants, prevalent in pastoralist Maasai, Beja, Tutsi, and Fulani populations at 50-90% frequency
- Middle East (−13915*G overlapping with East African): common in Saudi and Bedouin populations
- South Asia (−13910*T introduced by Indo-European migration): moderate frequency in northern India and Pakistan
The Tishkoff et al. 2007 paper (PMID 17159977) demonstrated through population genetics that the East African variants arose independently of the European variant within the past 3,000-7,000 years — one of the cleanest examples of convergent evolution under recent selection in the human lineage. The selective advantage in dairying populations was substantial, with selection coefficients estimated at 0.04-0.10, among the highest documented in the human genome.
3. Global Geography of Lactose Tolerance
The Storhaug et al. 2017 meta-analysis in Lancet Gastroenterology & Hepatology (PMID 28690131) provides the most comprehensive country-by-country estimates. Approximate adult lactose malabsorption prevalence (the proportion of adults without a lactase-persistence variant):
- Denmark, Sweden, Netherlands, Ireland, UK: 5-15%
- Germany, France, Northern Italy: 15-30%
- Southern Italy, Greece, Spain: 40-60%
- India (Northern, including Punjabi): 20-30%
- India (Southern, including Tamil): 50-70%
- West Africa (Yoruba, Igbo): 70-90%
- East Africa pastoralist (Maasai, Tutsi): 10-30%
- East Africa non-pastoralist (Bantu): 70-95%
- Native American: 80-100%
- East Asia (Chinese, Japanese, Korean): 85-100%
- Southeast Asia: 90-100%
- Australia (indigenous): 85-95%
- Australia, Canada, USA (European-descent): 5-25%
Globally, approximately 65-70% of adults have some degree of lactose malabsorption, making lactase persistence (not lactose intolerance) the unusual condition from a global perspective.
4. Symptoms and Diagnosis
Symptoms of lactose intolerance typically appear 30 minutes to 2 hours after lactose ingestion and include: abdominal bloating, abdominal pain or cramping, increased flatulence, loose stools or watery diarrhea, and audible bowel sounds. The severity is dose-dependent and varies among individuals with similar genotypes due to differences in colonic microbiota, gut transit time, and the presence of other carbohydrates that may modulate fermentation.
Three diagnostic tests are available:
- Hydrogen breath test: the standard clinical test. The patient consumes a 25-50 g lactose dose; expired breath hydrogen is measured every 15-30 minutes for 3 hours. An increase of 20 ppm or more above baseline is positive. Sensitivity ~80%, specificity ~85%.
- Lactose tolerance test (blood glucose): the older test. Patient consumes 50 g lactose; serum glucose measured at 0, 60, 120 minutes. Rise of less than 1.4 mmol/L (25 mg/dL) is positive. Less specific than the breath test.
- Genetic testing for the −13910*T (and related) variants: useful in patients of European, Indian, or East African ancestry but does not detect all causes of low lactase, and does not detect secondary lactase deficiency (see below).
The simplest practical test is the dietary elimination/rechallenge: eliminate all dairy for 7 days, then reintroduce a moderate dose (1 cup milk) and watch for symptoms within 4 hours. Symptoms on rechallenge but absent on elimination is diagnostic for practical purposes, though it does not distinguish lactose intolerance from milk-protein issues (alpha-s1 casein allergy or A1 beta-casein BCM-7 sensitivity).
5. The Threshold Dose
The Hertzler & Savaiano 1996 study (PMID 8780346) and the NIH consensus statement (Suchy et al. 2010, PMID 20404261) are the key references for the dose-response relationship. Findings:
- 12 g lactose (1 cup milk) consumed alone: tolerated without symptoms by most lactose-intolerant adults
- 12 g lactose consumed with other food: tolerated by virtually all lactose-intolerant adults (food slows gastric emptying and dilutes the lactose load)
- 24 g lactose (2 cups milk) consumed alone: symptomatic in about 50% of lactose-intolerant adults
- 50 g lactose (4 cups milk) consumed alone: symptomatic in essentially all lactose-intolerant adults
The implication is that the practical management of lactose intolerance is largely a question of dose and pacing, not complete elimination. A lactose-intolerant adult who limits dairy to no more than one cup of milk at a time, taken with food, and who distributes consumption across the day, can typically get most of the nutritional benefit of dairy (calcium, protein, B12) without symptoms.
The Hertzler & Savaiano paper also documented that some lactose-intolerant adults experience colonic adaptation with regular dairy consumption — over 10-14 days of daily lactose intake, colonic bacteria upregulate beta-galactosidase activity, reducing symptomatic fermentation of the same lactose load. This is the basis for the "build up tolerance gradually" advice given to patients.
6. Why Fermented Dairy Works
Yogurt, kefir, buttermilk, and aged cheese are typically well-tolerated by lactose-intolerant adults despite being made from lactose-containing milk. Three mechanisms operate:
- Fermentation reduces residual lactose: in yogurt, the starter cultures (Streptococcus thermophilus and Lactobacillus bulgaricus) consume approximately 30-50% of the lactose during fermentation, converting it to lactic acid. Plain unsweetened yogurt typically contains 4-5 g lactose per cup, vs 12 g in milk.
- Live cultures deliver their own beta-galactosidase enzyme: the Savaiano 2014 review (PMID 24695891) emphasizes that the bacterial cells in live-culture yogurt and kefir carry their own beta-galactosidase enzyme, which is released during transit through the gut and continues to hydrolyze residual lactose in vivo. This is the dominant mechanism, and it explains why heat-treated (pasteurized-after-fermentation) yogurt does not work as well as live-culture yogurt for the lactose-intolerant.
- Aged cheese has essentially no lactose: hard cheeses (cheddar, parmesan, Swiss, gouda) ripened for 60+ days contain less than 0.1 g lactose per 30 g serving — effectively zero. The lactose is consumed by ripening cultures or drained off in the whey during cheesemaking. Aged hard cheese can be consumed by virtually all lactose-intolerant adults without symptoms.
Kefir typically contains less residual lactose than yogurt (often 30-50% lower) and a more diverse range of beta-galactosidase-producing organisms, making it among the best-tolerated forms of fluid dairy for the lactose-intolerant.
7. Lactose-Free Milk, Enzyme Pills, and Adaptation
Three practical approaches to enjoying dairy with lactose intolerance:
- Lactose-free milk: commercial product (e.g., Lactaid in the US, Zymil in Europe) made by adding microbial beta-galactosidase to ordinary milk during processing, which hydrolyzes essentially all the lactose to glucose and galactose before packaging. The product tastes slightly sweeter than ordinary milk (because glucose and galactose are sweeter than lactose) but is otherwise indistinguishable nutritionally. This is the most reliable workaround.
- Lactase enzyme pills: commercial supplements (Lactaid caplets, Dairy Ease) deliver microbial beta-galactosidase enzyme in a pill that the consumer takes with the first bite of dairy. Each tablet typically delivers 3,000-9,000 FCC units of enzyme activity. The pills work reasonably well for moderate dairy meals; they are less reliable for large dairy loads or for individuals with the most severe lactose intolerance, because of variable enzyme delivery and acid inactivation in the stomach.
- Gradual reintroduction / colonic adaptation: starting with very small daily doses (1/4 cup milk per day) and gradually increasing over 2-4 weeks allows colonic flora to adapt with upregulated bacterial beta-galactosidase activity. This works for some patients and not for others; it does not change the small-intestinal lactase deficiency, only the colonic fermentation profile.
Plant-based milk substitutes (soy, almond, oat, coconut milk) are by default lactose-free and are reasonable substitutes for fluid milk in cooking and beverages. Their protein content is typically much lower than cow's milk (oat and almond milks contain 1-2 g protein per cup vs 8 g in cow's milk; soy milk contains 7-8 g and is the only plant milk with a comparable amino acid profile). Calcium content varies; fortified plant milks typically deliver 30-45% of the daily value per cup, comparable to cow's milk.
8. Primary vs Secondary Lactase Deficiency
Primary lactase deficiency is the genetic condition described above — the post-weaning decline of lactase expression in individuals without a lactase-persistence variant. It is the cause of essentially all lactose intolerance in healthy adults.
Secondary lactase deficiency is an acquired condition in which the intestinal lactase enzyme is reduced because of damage to the small intestinal brush border. Causes include:
- Acute gastroenteritis (typically resolves within 2-6 weeks of recovery)
- Celiac disease (resolves with gluten-free diet)
- Crohn's disease (may resolve with disease remission)
- Small intestinal bacterial overgrowth (resolves with SIBO treatment)
- Giardiasis and other parasitic infections (resolves with treatment)
- Radiation enteritis
- Severe malnutrition
An adult with previously normal dairy tolerance who develops sudden-onset lactose intolerance should be evaluated for these conditions before assuming the development of late-onset primary lactose intolerance (which does occur but is uncommon in adults of European ancestry).
Congenital lactase deficiency is a rare autosomal recessive disorder in which a child is born with no functional lactase enzyme. It presents in the neonatal period with severe watery diarrhea on the first feeds of breast milk or formula and is incompatible with survival without a lactose-free formula.
9. Lactose Intolerance Is Not Milk Allergy
An important and frequently confused distinction: lactose intolerance is a digestive enzyme deficiency causing osmotic and fermentative GI symptoms; cow's milk protein allergy (CMPA) is an immune-mediated reaction to milk proteins (typically alpha-s1 casein or whey).
- Lactose intolerance: symptoms are confined to the GI tract (bloating, gas, diarrhea), occur within hours of ingestion, are dose-dependent, are not life-threatening, and typically permit small doses of dairy without symptoms.
- Cow's milk protein allergy: symptoms can include urticaria (hives), angioedema, vomiting, eczema flare, wheezing, and in severe cases anaphylaxis. Symptoms occur within minutes to a few hours of even small amounts. CMPA in infants is common (2-3% prevalence) but most resolve by age 3-5. Adult-onset CMPA is rare.
- Non-IgE-mediated milk protein intolerance (eosinophilic esophagitis, FPIES): a separate category producing chronic GI symptoms and eosinophilic inflammation, requiring complete dairy exclusion and pediatric specialist management.
- A1 beta-casein BCM-7 sensitivity: a third category overlapping with lactose intolerance presentation; see the A1 vs A2 page.
A patient who experiences GI symptoms after dairy should consider all four possibilities. The simplest sequential workup is: try lactose-free milk for 7 days (rules in/out lactose intolerance); if symptoms persist, try A2 milk for 7 days (rules in/out BCM-7 sensitivity); if symptoms persist, eliminate all dairy and consult a clinician about possible milk-protein allergy or intolerance.
10. Research Papers
- Enattah NS et al., Identification of a variant associated with adult-type hypolactasia (Nat Genet 2002;30:233-237) — PubMed PMID 11788828
- Tishkoff SA et al., Convergent adaptation of human lactase persistence in Africa and Europe (Nat Genet 2007;39:31-40) — PubMed PMID 17159977
- Suchy FJ et al., NIH consensus development conference statement: lactose intolerance and health (Ann Intern Med 2010;152:792-796) — PubMed PMID 20404261
- Savaiano DA, Lactose digestion from yogurt: mechanism and relevance (Am J Clin Nutr 2014;99:1251S-1255S) — Search PubMed
- Misselwitz B et al., Update on lactose malabsorption and intolerance: pathogenesis, diagnosis and clinical management (Gut 2019;68:2080-2091) — Search PubMed
- Storhaug CL, Fosse SK, Fadnes LT, Country, regional, and global estimates for lactose malabsorption in adults: a systematic review and meta-analysis (Lancet Gastroenterol Hepatol 2017;2:738-746) — PubMed PMID 28690131
- Hertzler SR, Savaiano DA, Colonic adaptation to daily lactose feeding in lactose maldigesters reduces lactose intolerance (Am J Clin Nutr 1996;64:232-236) — Search PubMed
- Hertzler SR, Clancy SM, Kefir improves lactose digestion and tolerance in adults with lactose maldigestion (J Am Diet Assoc 2003;103:582-587) — PubMed PMID 12728216
- Lukito W, Malik SG, Surono IS, Wahlqvist ML, From 'lactose intolerance' to 'lactose nutrition' (Asia Pac J Clin Nutr 2015) — PubMed PMID 26715080
- Itan Y et al., A worldwide correlation of lactase persistence phenotype and genotypes (BMC Evol Biol 2010;10:36) — PubMed PMID 20144208
- Heyman MB, Lactose intolerance in infants, children, and adolescents (Pediatrics 2006;118:1279-1286) — PubMed PMID 16951027
- Lactase enzyme supplement efficacy in randomized trials PubMed: Lactase supplement RCTs
11. External Resources
- NIH NIDDK — Lactose Intolerance
- MedlinePlus — Lactose Intolerance
- NIH NIDDK — Eating, Diet, and Nutrition for Lactose Intolerance
- MedlinePlus Genetics — Lactose Intolerance Genetics
- PubMed — All lactose intolerance / lactase persistence research
12. Connections
- Milk Benefits Hub
- A1 vs A2 Casein
- Raw vs Pasteurized
- Grass-Fed and CLA
- Milk (Main Page)
- Yogurt
- Gastroenterology
- Irritable Bowel Syndrome
- SIBO
- Calcium
- Vitamin D3
- Vitamin B12
- All Foods
- Lactose Intolerance — the full clinical page on diagnosis and management.