Honey as a Cough Suppressant — The Pediatric and Adult Evidence
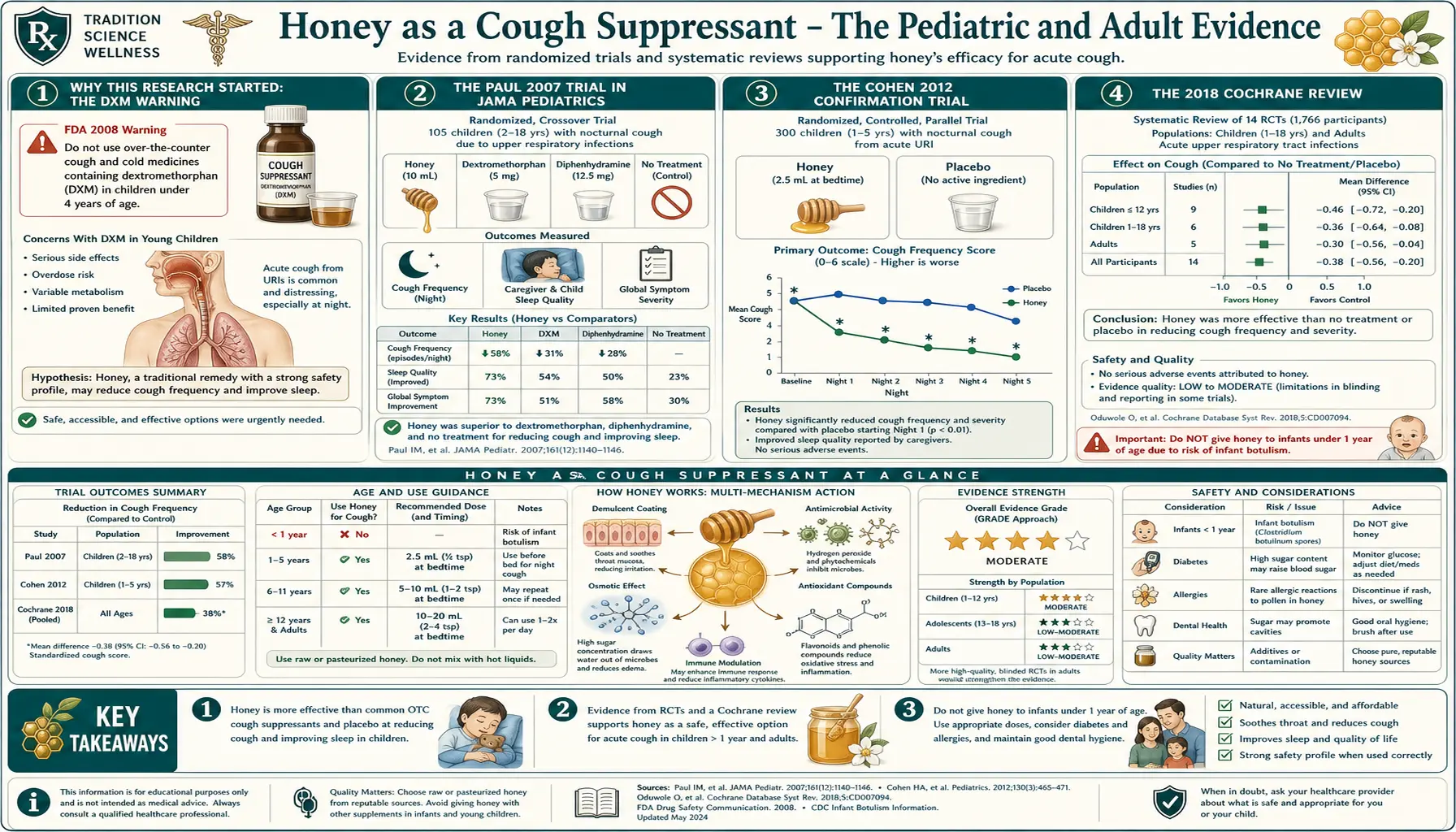
In 2007, Ian Paul and colleagues at Penn State College of Medicine published an unusual trial in JAMA Pediatrics. They randomized 105 children aged 2-18 with upper respiratory infection and nocturnal cough to one of three treatments: a single bedtime dose of buckwheat honey, an age-appropriate dose of dextromethorphan (the active ingredient in most over-the-counter cough syrups), or no treatment. Honey beat dextromethorphan and beat no treatment for both cough frequency and parent-rated sleep quality. The paper, published two months after the FDA had warned against over-the-counter cough and cold medicine for children under six, prompted the American Academy of Pediatrics and World Health Organization to formally endorse honey as first-line therapy for nocturnal cough in children over 12 months. A 2018 Cochrane review of six pediatric trials confirmed the effect. The evidence in adults is less robust but generally supportive. This page walks through the trial evidence, the proposed mechanisms (demulcent coating, sweet-taste mediated mucus production, mild antimicrobial effect), the buckwheat-honey angle, practical dosing, and the categorical infant contraindication that applies regardless of cough severity.
Table of Contents
- Why This Research Started: The DXM Warning
- The Paul 2007 Trial in JAMA Pediatrics
- The Cohen 2012 Confirmation Trial
- The 2018 Cochrane Review
- Proposed Mechanisms
- Why Buckwheat Honey Specifically
- Practical Dosing
- Adult Cough Evidence
- The Infant Contraindication
- Cautions
- Key Research Papers
- Connections
- Featured Videos
Why This Research Started: The DXM Warning
To understand why a JAMA Pediatrics paper on honey for cough became influential, it helps to know what was happening in pediatric cough-and-cold medicine in the years leading up to it.
For decades, over-the-counter cough and cold medicines for children — combining antitussives (dextromethorphan or DXM), antihistamines (diphenhydramine, brompheniramine), decongestants (pseudoephedrine, phenylephrine), and expectorants (guaifenesin) — were standard pediatric pharmacy products, frequently used by parents and recommended by pediatricians. The accumulated trial evidence for efficacy in children was thin, however, and safety concerns mounted through the 1990s and early 2000s as case reports accumulated of dose-related toxicity (sedation, respiratory depression, cardiac events, and rare fatal overdoses) particularly in infants and toddlers.
In October 2007, the FDA convened a Nonprescription Drugs Advisory Committee that recommended against the use of over-the-counter cough and cold medicines in children under six years of age. The agency followed with a Public Health Advisory that month. Manufacturers voluntarily relabeled products to "Do not use in children under 4." The American Academy of Pediatrics went further, recommending against use under 6 years.
This created a clinical vacuum. Parents and pediatricians faced sick children with miserable nighttime cough and no recommended pharmacy intervention. Into this gap, the Paul 2007 trial — published just two months after the FDA advisory — offered a credible, evidence-based, low-cost alternative. The timing was a major factor in its rapid adoption.
The Paul 2007 Trial in JAMA Pediatrics
The Paul trial (Archives of Pediatrics and Adolescent Medicine, 2007; the journal was later renamed JAMA Pediatrics) was a three-arm randomized controlled trial. Participants were 105 children aged 2-18 with upper respiratory infection, cough symptoms for less than 7 days, and no underlying chronic respiratory disease. They were randomized at the bedtime appointment to one of:
- Buckwheat honey — weight-based dose (half-teaspoon for ages 2-5, one teaspoon for ages 6-11, two teaspoons for ages 12+), given 30 minutes before bedtime
- Dextromethorphan — honey-flavored dextromethorphan in age-appropriate dose
- No treatment — control arm received no intervention
The next morning, parents completed a 5-question survey scoring (on 0-6 Likert scales) the previous night's cough frequency, cough severity, bothersome cough impact on the child, impact on parent sleep, and impact on child sleep. Results:
- Honey scored significantly better than no treatment on all five outcome measures
- Honey scored significantly better than dextromethorphan on cough frequency, cough severity, and combined cough symptom score
- Dextromethorphan vs no treatment showed no statistically significant difference, consistent with the broader literature questioning OTC cough syrup efficacy in children
- Honey was well tolerated; mild hyperactivity was reported in 5 honey-treated children (likely sugar-related), no other adverse effects
The trial was funded in part by the National Honey Board, an industry trade group — an important caveat that the authors disclosed. However, the methodology (single-night three-arm randomized comparison) was sound, and the result has been independently replicated.
The Cohen 2012 Confirmation Trial
The most important methodological criticism of the Paul 2007 trial was the lack of placebo. The no-treatment group could not be blinded; parents who got honey for their child knew they were getting active treatment. The Cohen 2012 trial in Pediatrics addressed this by using a syrup-textured placebo (silan date extract) that matched honey for sweetness and viscosity.
Cohen et al. randomized 300 Israeli children aged 1-5 with upper respiratory infection and nocturnal cough to one of four arms:
- Eucalyptus honey
- Citrus honey
- Labiatae (lip-family) honey
- Placebo (silan date extract, matched for sweetness and viscosity)
All four arms received a 10 g (about 2 teaspoon) dose 30 minutes before bedtime. The cough scoring system was the same Likert-scale parent-completed survey from the Paul protocol.
Results: All three honey varieties produced significantly larger improvements than placebo for cough frequency, cough severity, bothersome impact, and child sleep. The three honey varieties did not differ significantly from each other. The improvement vs placebo was approximately equivalent in magnitude to that seen in the Paul honey-vs-DXM comparison.
Together, the Paul 2007 and Cohen 2012 trials established that:
- Honey is superior to placebo for nocturnal cough in children — ruling out the "sweetness alone" or "viscosity alone" explanation
- Honey is superior to dextromethorphan for the same outcome — though DXM is also barely better than no treatment
- The effect generalizes across multiple honey types (buckwheat, eucalyptus, citrus, labiatae)
The 2018 Cochrane Review
The Oduwole 2018 Cochrane review (PMID 29633783) pooled six trials with 899 children with acute cough due to upper respiratory infection. The pooled effect:
- Honey vs no treatment for cough frequency: standardized mean difference -1.05 (large effect favoring honey)
- Honey vs no treatment for cough severity: standardized mean difference -1.01 (large effect favoring honey)
- Honey vs diphenhydramine (Benadryl): not significantly different (both reduced cough)
- Honey vs dextromethorphan: similar effect, with honey marginally favored
- Honey vs salbutamol or bromelain: similar effect
- Honey vs placebo: significantly favoring honey
The Cochrane review concluded that honey probably reduces cough symptoms more than no treatment, diphenhydramine, and placebo, with a similar effect to dextromethorphan. The quality of evidence was rated as moderate for the honey-vs-placebo and honey-vs-DXM comparisons, and lower for the other comparisons.
Based on this evidence, the World Health Organization, the American Academy of Pediatrics, the UK National Institute for Health and Care Excellence (NICE), and equivalent agencies in most developed countries now recommend honey as a first-line treatment for symptomatic relief of acute cough in children over 12 months old.
Proposed Mechanisms
No single mechanism fully explains honey's antitussive effect. The proposed contributing mechanisms include:
- Demulcent coating effect — honey is viscous and adheres to the pharyngeal mucosa, providing a physical coating that may reduce irritation of cough-trigger receptors in the upper airway. This is the same proposed mechanism for the older "honey-and-lemon" home remedy.
- Sweet-taste reflex — the strong sweet taste of honey triggers salivation and increased mucus production in the upper airway. The increased airway secretions may dilute irritants and reduce cough sensitivity. There is also some evidence that sweet taste produces a centrally-mediated cough-reflex modulation via the medullary cough center, though this is less well established.
- Mild antimicrobial activity — the four mechanisms of honey antibacterial activity (osmotic, peroxide, low pH, and MGO in Manuka) discussed in the Wound Healing page may reduce bacterial colonization on the pharyngeal mucosa, though most upper-respiratory cough is viral rather than bacterial.
- Anti-inflammatory and antioxidant phenolics — honey's polyphenols, particularly in dark honeys like buckwheat, may produce local mucosal anti-inflammatory effects. Raw honey retains more of these than pasteurized.
- Sleep-quality effect — both Paul and Cohen reported parent-rated sleep improvement, which may be partly independent of objective cough frequency. A demulcent that interrupts even a few coughs in the early sleep period may produce disproportionate benefit for sleep continuity.
Importantly, the mechanism is local and short-lasting. Honey does not provide a systemic antitussive effect like dextromethorphan or codeine. The benefit window is approximately the first 30-60 minutes after dosing — which is why the trials specifically dosed 30 minutes before bedtime to align peak effect with the period of greatest sleep-onset disruption.
Why Buckwheat Honey Specifically
Paul 2007 specifically used buckwheat honey, and it has become the default recommendation in many US pediatric circles. The reasons:
- High phenolic content — buckwheat honey is one of the darkest commercially available honeys (along with manuka, heather, and chestnut). Color in honey roughly tracks total phenolic content; darker honeys have more antioxidant and anti-inflammatory polyphenols. Buckwheat honey's ORAC (oxygen radical absorbance capacity) is typically 5-10 times that of clover honey.
- Strong characteristic taste — buckwheat honey has a robust, molasses-like flavor that produces a strong sweet-taste reflex. Children sometimes don't love the flavor, but it triggers the salivation and mucus-production response well.
- Availability — buckwheat honey is widely available from US producers in Pennsylvania, New York, and the upper Midwest. Cohen 2012 confirmed that other dark honey varieties (eucalyptus, citrus, labiatae) work comparably.
For practical purposes, any dark, unprocessed, raw or minimally-processed honey appears equivalent. Manuka honey works for cough but is overkill and unnecessarily expensive for this application — the MGO content that distinguishes Manuka is mostly irrelevant to the cough mechanism. For cough use, save the money and use a domestic dark varietal.
Practical Dosing
The trial-validated dose schedule:
- Children 1-5 years — half teaspoon (2.5 mL, approximately 3.5 g) 30 minutes before bedtime
- Children 6-11 years — one teaspoon (5 mL, approximately 7 g) 30 minutes before bedtime
- Children 12+ years and adults — two teaspoons (10 mL, approximately 14 g) 30 minutes before bedtime
The dose can be given straight from a spoon, mixed into a small amount of warm (not hot) water or chamomile tea, or used to coat the throat directly. Avoid mixing into very hot tea, which dilutes the demulcent coating effect.
The dose can be repeated during the night if needed (e.g. if cough recurs and disrupts sleep at 2 AM), though most trials studied only single bedtime dosing.
Duration of use: continue for the duration of the cough symptoms, typically 3-7 days for a typical upper respiratory infection. A cough that persists more than 2 weeks warrants medical evaluation; honey is not a treatment for chronic cough, post-viral bronchial hyperreactivity, asthma, or any non-self-limiting cough syndrome. See the Cough page for a broader discussion of cough etiologies.
Adult Cough Evidence
The evidence base in adults is much smaller than in children, primarily because the major trials have focused on the pediatric population (where DXM is not recommended and the clinical need for an alternative is greatest). The Abuelgasim 2021 systematic review (PMID 32817011) pooled adult and adolescent trials and found:
- Honey was associated with greater improvement in cough symptoms than usual care in upper respiratory tract infections
- The effect size was smaller than seen in pediatric trials
- Heterogeneity between trials was substantial, limiting confidence in the pooled estimate
The mechanistic plausibility of benefit in adults is the same as in children (demulcent, sweet-taste, mild antimicrobial). The practical recommendation is that honey is a reasonable, low-cost, low-risk first-line option for adult acute cough due to upper respiratory infection. It is not a substitute for clinician evaluation if cough is severe, persistent beyond 2 weeks, productive of purulent or bloody sputum, accompanied by fever, or in a patient with underlying lung disease. For these scenarios see the Bronchitis page and the Pneumonia page.
The Infant Contraindication
The single most important caveat for honey-for-cough: do not give honey to infants under 12 months old, no matter how severe the cough. The risk of infant botulism (discussed in detail on the Raw vs Pasteurized page) outweighs any potential benefit. This contraindication applies to:
- All honey varieties — clover, buckwheat, wildflower, orange blossom, Manuka, any other
- Both raw and pasteurized honey (pasteurization does not eliminate Clostridium botulinum spores)
- Honey in any preparation — on a spoon, in tea, in cereal, on a pacifier, in baby food
- Comb honey, honey-containing products, and granola, breads, or baked goods sweetened with honey if the infant might mouth a portion
An infant under 12 months with a cough that interferes with feeding or sleep should be evaluated by a pediatrician. Treatment options include saline nasal drops, humidified air, fever management with acetaminophen (per pediatrician), and the patience to wait out the typical 7-10 day course of a viral upper respiratory infection. Honey is contraindicated as is most OTC cough/cold medicine.
Cautions
- Under 12 months — absolute contraindication — see above
- Diabetes — honey contains approximately 80% sugar. The single-dose (1-2 teaspoon = 7-14 g) load is small and unlikely to cause significant glycemic issues in well-controlled diabetes, but should be counted as carbohydrate. Diabetic patients on insulin or sulfonylureas should be aware.
- Tooth decay — honey is cariogenic. The bedtime dosing pattern places sugar on tooth surfaces during the sleeping hours, when salivary clearance is minimal. After dosing, the child should rinse the mouth with water; brushing 20-30 minutes later (to allow tooth enamel to re-mineralize after the acid exposure) is ideal.
- Honey allergy — rare but possible. Anaphylaxis to honey has been reported, particularly in individuals with severe bee-venom allergy or with allergy to specific pollens (composite-family pollens in particular). Discontinue at any sign of allergic reaction.
- Pollen-allergic individuals — raw honey contains pollen and may transiently worsen seasonal allergy symptoms in highly sensitized individuals. Pasteurized or ultra-filtered honey has lower pollen content. The "local honey desensitizes you to local allergens" claim is not well supported; honey contains primarily entomophilous (insect-pollinated) pollens, while seasonal allergic rhinitis is caused primarily by anemophilous (wind-pollinated) pollens that bees do not collect.
- Cough that lasts more than 2 weeks — not within the scope of self-treatment. Evaluate for post-infectious cough, pertussis, asthma, GERD, ACE-inhibitor cough, post-nasal drip syndrome, or other causes.
- Productive cough with discolored sputum, fever, or shortness of breath — suggests bacterial bronchitis or pneumonia. Evaluate with a clinician; honey is not a substitute for antibiotic therapy when indicated.
- Mad honey poisoning — honey from Rhododendron-rich regions of Turkey, Nepal, and certain other areas can contain grayanotoxin. Rare in commercial honey but a real consideration for tourist purchases.
- Drug interactions — no documented oral-honey drug interactions at the small doses used for cough.
Key Research Papers
- Paul IM, Beiler J, McMonagle A, Shaffer ML, Duda L, Berlin CM Jr (2007). Effect of honey, dextromethorphan, and no treatment on nocturnal cough and sleep quality for coughing children and their parents. Archives of Pediatrics & Adolescent Medicine. — PubMed: PMID 18056558
- Cohen HA, Rozen J, Kristal H, Laks Y, Berkovitch M, Uziel Y, Kozer E, Pomeranz A, Efrat H (2012). Effect of honey on nocturnal cough and sleep quality: a double-blind, randomized, placebo-controlled study. Pediatrics. — PubMed: PMID 22869830
- Oduwole O, Udoh EE, Oyo-Ita A, Meremikwu MM (2018). Honey for acute cough in children. Cochrane Database of Systematic Reviews. — Search PubMed
- Shadkam MN, Mozaffari-Khosravi H, Mozayan MR (2010). A comparison of the effect of honey, dextromethorphan, and diphenhydramine on nightly cough and sleep quality in children and their parents. Journal of Alternative and Complementary Medicine. — PubMed: PMID 20618098
- Abuelgasim H, Albury C, Lee J (2021). Effectiveness of honey for symptomatic relief in upper respiratory tract infections: a systematic review and meta-analysis. BMJ Evidence-Based Medicine. — PubMed: PMID 32817011
- Paul IM (2012). Therapeutic options for acute cough due to upper respiratory infections in children. Lung. PubMed: Paul therapeutic options
- Goldman RD (2014). Honey for treatment of cough in children. Canadian Family Physician. — PubMed: PMID 25551129
- Eccles R (2006). Mechanisms of the placebo effect of sweet cough syrups. Respiratory Physiology & Neurobiology. — Search PubMed
- Smith SM, Schroeder K, Fahey T (2014). Over-the-counter (OTC) medications for acute cough in children and adults in community settings. Cochrane Database. — PubMed: PMID 25420096
- WHO (2001). Cough and cold remedies for the treatment of acute respiratory infections in young children. PubMed: WHO cough and cold
- Schroeder K, Fahey T (2002). Systematic review of randomised controlled trials of over the counter cough medicines for acute cough in adults. BMJ. — Search PubMed
- Ayazi P, Mahyar A, Yousef-Zanjani M, Allami A, Esmailzadehha N, Beyhaghi T (2017). Comparison of the effect of two kinds of Iranian honey and diphenhydramine on nocturnal cough and the sleep quality in coughing children and their parents. PLOS ONE. — Search PubMed
PubMed Topic Searches
- PubMed: Honey nocturnal cough RCT
- PubMed: Honey vs DXM pediatric
- PubMed: Buckwheat honey for cough
- PubMed: Sweet demulcent mechanism
- PubMed: FDA OTC cough/cold under 6
Connections
- Honey Main Page
- Honey Benefits Hub
- Manuka and MGO Rating
- Raw vs Pasteurized
- Wound Healing Topical
- Cough
- Bronchitis
- Pneumonia
- Asthma
- Sore Throat
- Immune Boosting
- Remedies
- Ginger
- Thyme
- All Food