Honey — Benefits Deep Dive
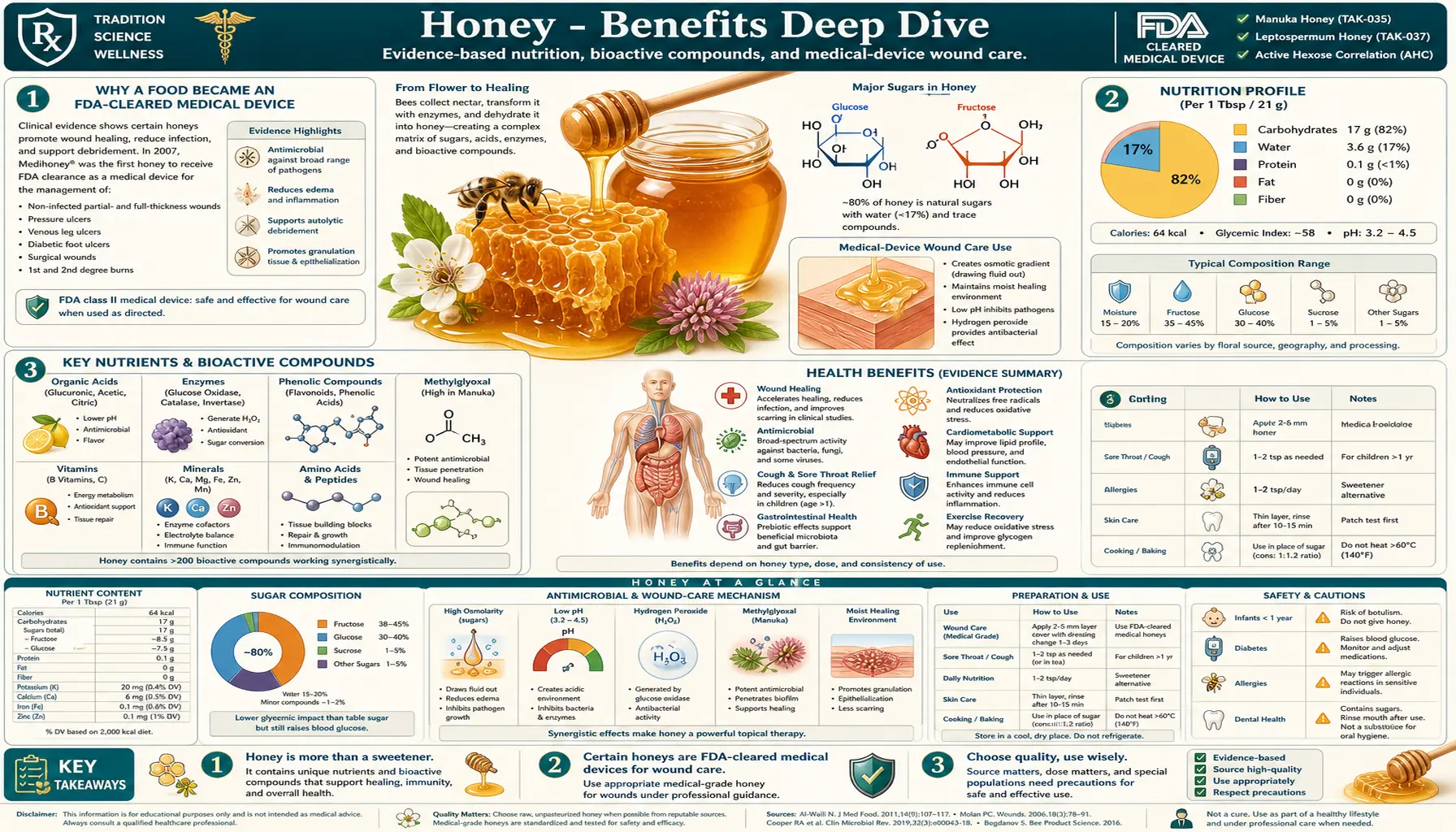
Honey is one of the few foods that has crossed the boundary from kitchen pantry to FDA-cleared medical device. Medical-grade Manuka honey dressings (Medihoney, Activon) are approved for the treatment of chronic wounds, burns, and ulcers in hospitals across the United States, the United Kingdom, Australia, and the European Union. The Cochrane Collaboration has published systematic reviews concluding that honey is superior to standard treatment for partial-thickness burns, and the World Health Organization recommends honey as a first-line cough remedy for children over 12 months. The four deep-dive pages below explore the four areas where honey's clinical evidence base is strongest: the chemistry of Manuka and MGO rating systems, the difference between raw and pasteurized honey, topical use for wound healing, and the use of honey as a cough suppressant.
Deep-Dive Articles
Manuka and MGO Rating
The chemistry of methylglyoxal (MGO) as the dominant non-peroxide antibacterial compound in Manuka honey, how dihydroxyacetone (DHA) in the nectar of Leptospermum scoparium converts to MGO during maturation, the UMF (Unique Manuka Factor) vs MGO vs NPA rating systems, the New Zealand MPI scientific test for authentic Manuka, the relationship between MGO concentration (50 mg/kg to 1,200+ mg/kg) and antibacterial potency, and how to read a Manuka label without being defrauded.
Raw vs Pasteurized
What is destroyed when honey is heated above 40°C / 104°F (glucose oxidase enzyme, hydrogen peroxide generation capacity, heat-labile phenolics, beneficial yeasts and bacteria) and what survives (sugar profile, basic acidity, MGO in Manuka). The commercial reasoning behind pasteurization (slows crystallization, sterilizes for shelf appearance), the infant botulism rule (no honey under 12 months regardless of processing), the difference between raw, unfiltered, strained, ultra-filtered, and pasteurized honey on a US label, and why "raw" is not a regulated term.
Wound Healing Topical
The four-mechanism wound-healing story: low water activity (aw < 0.6 dehydrates bacteria osmotically), hydrogen peroxide release from glucose oxidase, low pH (3.2-4.5 inhibits bacterial protease activity), and (in Manuka) direct methylglyoxal kill. FDA clearance of Medihoney and Activon dressings, Cochrane review evidence for partial-thickness burns, diabetic foot ulcer protocols, MRSA and Pseudomonas aeruginosa coverage, why honey does not promote antibiotic resistance, and the practical limits (deep wounds, internal infection, allergy).
Cough Suppressant Evidence
The Paul et al. 2007 NEJM trial that established honey as superior to dextromethorphan and to no treatment for nocturnal cough and sleep quality in children over 12 months, the WHO and AAP first-line recommendation, the Cochrane review of six pediatric trials, the proposed mechanisms (demulcent coating effect, sweet taste-mediated saliva and mucus production, mild antimicrobial effect), the buckwheat honey advantage, the strict infant contraindication for Clostridium botulinum spores, and the adult evidence (less robust but supportive).
Table of Contents
- Deep-Dive Articles
- Why a Food Became an FDA-Cleared Medical Device
- Research Papers: Manuka and MGO Chemistry
- Research Papers: Raw vs Pasteurized
- Research Papers: Wound Healing
- Research Papers: Cough Suppressant
- Research Papers: Cross-Cutting (Composition, Safety)
- External Authoritative Resources
- Connections
- Featured Videos
Why a Food Became an FDA-Cleared Medical Device
Honey is unusual in modern medicine because it has moved backward through the regulatory pipeline. Most therapeutic agents start as folk remedies, get studied scientifically, and either fail and are abandoned or succeed and become standardized pharmaceuticals. Honey was abandoned as a wound dressing in the 1940s when antibiotics arrived, then re-emerged in the 1990s and 2000s as antibiotic resistance accelerated, and is now back in the hospital formulary — not as a folk remedy but as an FDA-cleared 510(k) medical device with documented efficacy against MRSA, Pseudomonas aeruginosa, and other multidrug-resistant pathogens.
Four mechanisms together account for the therapeutic effect, and understanding all four is necessary to understand why one type of honey works for one application and not another:
- Osmotic dehydration of bacteria — all honey has water activity (aw) below 0.6, well under the 0.85 threshold most bacteria require for growth. Honey applied to a wound surface draws water osmotically out of bacterial cells. This mechanism works for any unadulterated honey.
- Hydrogen peroxide generation — bee-derived glucose oxidase, suspended inactive in the concentrated honey, becomes active when honey is diluted (for example, by wound exudate). The enzyme converts glucose to gluconic acid and hydrogen peroxide. The slow, sustained, low-concentration peroxide release is bactericidal without the tissue toxicity of pharmacy-grade 3% hydrogen peroxide. This mechanism is destroyed by pasteurization — glucose oxidase is heat-labile.
- Low pH — honey is acidic (pH 3.2-4.5). On a wound surface this creates an environment unfavorable to bacterial protease activity and shifts the wound milieu toward conditions that support keratinocyte migration and tissue healing.
- Methylglyoxal (MGO) — Manuka only — Manuka honey, made from the nectar of New Zealand and Australian Leptospermum scoparium (the manuka or tea tree), contains 50 to over 1,200 mg/kg of methylglyoxal, a small alpha-oxoaldehyde with direct bactericidal action through protein and DNA alkylation. The MGO/UMF rating systems quantify this. Non-Manuka honey contains 1-10 mg/kg of MGO — effectively zero by comparison.
The clinical translation falls into two clearly delineated buckets — topical applications, where the FDA-cleared Manuka dressings have transformed chronic wound and burn care, and oral applications, where the WHO recommends honey as first-line treatment for nocturnal cough in children over 12 months. The first three deep-dive pages cover the topical and chemistry side; the fourth covers the oral cough evidence. The categorical infant warning — no honey under 12 months, ever, due to risk of infant botulism from Clostridium botulinum spores — cuts across all applications and is repeated on every page.
Research Papers: Manuka and MGO Chemistry
- Mavric E et al. (2008). Identification and quantification of methylglyoxal as the dominant antibacterial constituent of Manuka honey Search PubMed
- Adams CJ et al. (2008). Isolation by HPLC and characterisation of the bioactive fraction of New Zealand manuka honey Search PubMed
- Adams CJ et al. (2009). The origin of methylglyoxal in New Zealand manuka honey (DHA-to-MGO conversion) — Search PubMed
- Atrott J, Henle T (2009). Methylglyoxal in Manuka honey: correlation with antibacterial properties PubMed: Atrott and Henle
- Allen KL, Molan PC, Reid GM (1991). A survey of the antibacterial activity of some New Zealand honeys PubMed: Allen-Molan 1991
- Molan PC (1992). The antibacterial activity of honey: the nature of the antibacterial activity (review) PubMed: Molan 1992
- UMF (Unique Manuka Factor) industry rating system origin PubMed: UMF rating
- New Zealand MPI scientific definition of monofloral Manuka honey PubMed: NZ MPI Manuka definition
- Leptosperin as Manuka authenticity marker PubMed: Leptosperin marker
- Stephens JM et al. (2010). Phenolic compounds and methylglyoxal in some New Zealand manuka and kanuka honeys PubMed: Stephens 2010
Research Papers: Raw vs Pasteurized
- Bogdanov S et al. (2008). Honey for nutrition and health: a review PubMed: Bogdanov review
- White JW Jr (1979). Composition of honey (USDA classic survey) PubMed: White USDA composition
- Effect of heat on honey diastase, invertase, and glucose oxidase activity PubMed: Heat effect on enzymes
- Hydroxymethylfurfural (HMF) accumulation as honey heat-damage marker PubMed: HMF marker
- Infant botulism and honey — CDC recommendation against honey under 12 months PubMed: Infant botulism and honey
- Raw vs heated honey phenolic content comparison PubMed: Raw vs heated phenolics
- Beneficial Lactobacillus and Bifidobacterium content of raw honey PubMed: Honey-borne probiotic species
- Adulteration of honey with corn syrup and rice syrup — detection methods PubMed: Adulteration detection
- Pollen content as raw-honey authenticity marker PubMed: Pollen melissopalynology
- Crystallization kinetics of honey (glucose vs fructose ratio) PubMed: Crystallization kinetics
Research Papers: Wound Healing
- Jull AB et al. (2015). Honey as a topical treatment for wounds (Cochrane systematic review, 26 trials, 3,011 participants) — PubMed: PMID 25742878
- Subrahmanyam M (1991). Topical application of honey in treatment of burns (Indian RCT, n=104) PubMed: Subrahmanyam burns RCT
- Molan PC, Rhodes T (2015). Honey: a biologic wound dressing (review) — PubMed: PMID 26061489
- Cooper RA et al. (2002). The sensitivity to honey of Gram-positive cocci of clinical significance isolated from wounds PubMed: Cooper Gram-positive sensitivity
- Cooper RA et al. (1999). The efficacy of honey in inhibiting strains of Pseudomonas aeruginosa from infected burns PubMed: Cooper Pseudomonas
- Maeda Y et al. (2008). Manuka honey eradicates biofilms in vitro PubMed: Manuka and biofilms
- Maddocks SE et al. (2012). Honey, biofilms, and Streptococcus pyogenes PubMed: Maddocks Streptococcus
- Medihoney FDA 510(k) clearance and clinical evidence for diabetic foot ulcers PubMed: Medihoney diabetic foot ulcer
- Honey vs silver sulfadiazine for partial-thickness burns RCT PubMed: Honey vs silver sulfadiazine
- Topical honey for venous leg ulcers (HALT trial) PubMed: HALT venous leg ulcer
Research Papers: Cough Suppressant
- Paul IM et al. (2007). Effect of honey, dextromethorphan, and no treatment on nocturnal cough and sleep quality for coughing children and their parents — PubMed: PMID 18056558
- Oduwole O et al. (2018). Honey for acute cough in children (Cochrane review of 6 trials) — PubMed: PMID 29633783
- Cohen HA et al. (2012). Effect of honey on nocturnal cough and sleep quality: a double-blind, randomized, placebo-controlled study — PubMed: PMID 22869830
- Shadkam MN et al. (2010). A comparison of the effect of honey, dextromethorphan, and diphenhydramine on nightly cough and sleep quality — PubMed: PMID 20618098
- Abuelgasim H et al. (2021). Effectiveness of honey for symptomatic relief in upper respiratory tract infections: systematic review — PubMed: PMID 32817011
- WHO recommendation on cough and cold remedies in children PubMed: WHO cough remedy recommendation
- American Academy of Pediatrics position on honey for cough PubMed: AAP honey cough
- Buckwheat honey vs other floral source honey for cough PubMed: Buckwheat honey for cough
- Sweet taste demulcent effect and cough reflex modulation PubMed: Sweet demulcent cough mechanism
- FDA black-box warning on dextromethorphan for children under 6 (the comparison context for honey research) PubMed: FDA OTC cough cold warning
Research Papers: Cross-Cutting (Composition, Safety)
- Honey allergy and pollen cross-reactivity PubMed: Honey allergy
- Glycemic index of honey vs sucrose vs glucose PubMed: Honey glycemic index
- Honey and lipid profile in human trials PubMed: Honey and lipid profile
- Honey, fructose content, and metabolic effects PubMed: Honey and fructose
- Pyrrolizidine alkaloid contamination of honey PubMed: Pyrrolizidine alkaloids in honey
- Mad honey (Rhododendron-derived grayanotoxin) poisoning PubMed: Mad honey grayanotoxin
- Honey and oral health: dental caries risk PubMed: Honey and dental caries
- Honey and allergic rhinitis (local honey allergy desensitization claim) PubMed: Honey and allergic rhinitis
- Honey antioxidant activity by floral source PubMed: Honey antioxidant by floral source
- Codex Alimentarius standard for honey PubMed: Codex honey standard
External Authoritative Resources
- World Health Organization — cough and cold guideline for children (honey recommended as first-line for nocturnal cough in children over 12 months)
- CDC — Infant Botulism Prevention (no honey under 12 months)
- FDA 510(k) clearance database for Medihoney, Activon, and other Manuka wound dressings
- New Zealand Ministry for Primary Industries — scientific definition of monofloral Manuka honey (the four chemical markers and one DNA marker)
- PubMed — All research on honey therapeutic use (over 8,000 papers)
Connections
- Honey (Main Page)
- Manuka and MGO Rating
- Raw vs Pasteurized
- Wound Healing (Topical)
- Cough Suppressant Evidence
- All Food
- Remedies
- Wound Care
- Cough
- Bronchitis
- Burns
- Diabetes (Foot Ulcer)
- Immune Boosting
- Sweet Potatoes
- Ginger