Manuka Honey and the MGO / UMF Rating System
Manuka honey is the only honey in commercial production whose antibacterial potency is high enough and chemically distinct enough to support an FDA-cleared medical device and a multi-billion-dollar global premium market. The dominant active compound is methylglyoxal (MGO), a small alpha-oxoaldehyde present at 50 to over 1,200 mg/kg in authentic Manuka and at only 1-10 mg/kg in ordinary honey — a 100-fold to 1,000-fold concentration difference. Three competing label systems (MGO mg/kg, UMF Unique Manuka Factor, and NPA Non-Peroxide Activity) all measure essentially the same thing, but the proliferation of unrelated marketing claims (KFactor, Bio Active, TA, Plus, etc.) has made the Manuka shelf one of the most confusing in the food and supplement category. This page walks through the chemistry, the rating systems, the New Zealand MPI scientific definition that distinguishes real Manuka from fraud, and the practical question of which jar to buy for which application.
Table of Contents
- Where Manuka Comes From: Leptospermum scoparium
- The DHA-to-MGO Conversion in the Honey Jar
- Mechanism: How MGO Kills Bacteria
- The Three Rating Systems (MGO, UMF, NPA)
- The New Zealand MPI Scientific Definition
- Choosing the Right MGO Strength for Each Application
- Avoiding Fraud and Watered-Down Manuka
- Australian vs New Zealand Manuka
- Cautions
- Key Research Papers
- Connections
- Featured Videos
Where Manuka Comes From: Leptospermum scoparium
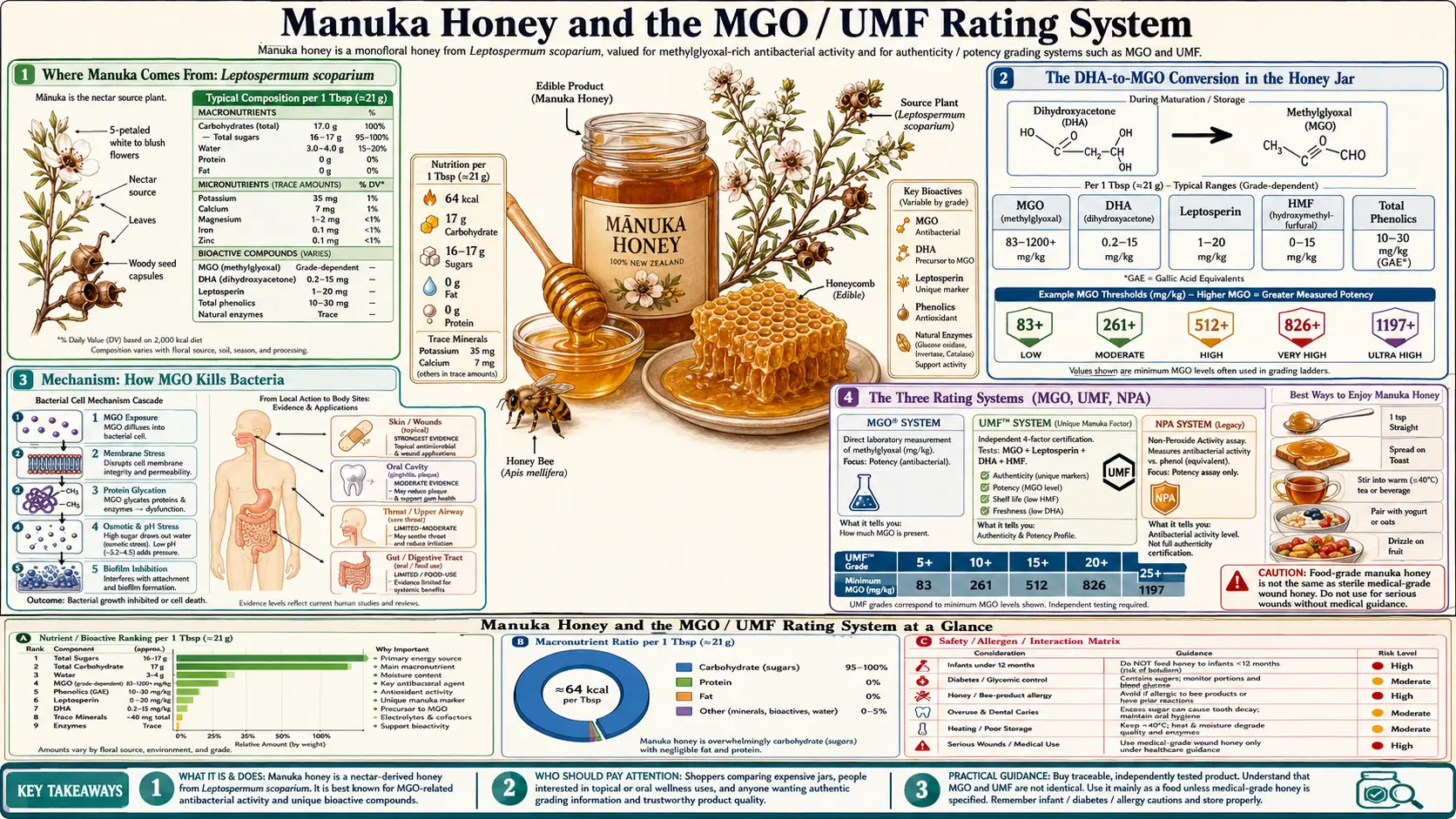
Manuka honey is the product of European honey bees (Apis mellifera) foraging on the nectar of Leptospermum scoparium, a small flowering shrub in the Myrtaceae family native to New Zealand and southeastern Australia. The plant is known as manuka or tea tree (not to be confused with Melaleuca alternifolia, the Australian tea tree from which tea tree oil is extracted). It grows abundantly on hillsides, in regenerating clearcut forest, and in scrub margins across both islands of New Zealand and parts of Tasmania, Victoria, and New South Wales.
The flowering window is narrow — typically 2 to 6 weeks in mid to late summer (December-February in the Southern Hemisphere). Beekeepers truck their hives into manuka stands for the duration of the bloom and pull them out as soon as the manuka is finished, before the bees can backfill the same combs with nectar from other plants. The intensity of manuka flowering in any given year is weather-dependent and unpredictable, which is the primary supply constraint that keeps prices high.
The nectar itself is not what is bactericidal. The active antibacterial precursor in nectar is dihydroxyacetone (DHA), a simple three-carbon ketose. DHA concentration in fresh manuka nectar varies dramatically by individual plant genetics, year, and location — this is why two jars of honest, authentic Manuka can have vastly different MGO ratings.
The DHA-to-MGO Conversion in the Honey Jar
The Adams 2009 paper (Carbohydrate Research) established the precise chemical pathway that distinguishes Manuka from all other honeys. The bees collect manuka nectar, transport it to the hive, and process it normally — reducing water content, adding enzymes, sealing the comb. Fresh-harvested Manuka honey contains high DHA but only modest MGO. Over the next 6 to 12 months in the jar at ambient temperature, DHA undergoes spontaneous non-enzymatic dehydration to methylglyoxal:
Dihydroxyacetone (DHA) → Methylglyoxal (MGO) + H2O
This is a slow chemical process — not a fermentation, not enzymatic, simply a temperature-dependent dehydration reaction in a highly concentrated acidic sugar matrix. The conversion accelerates at warmer storage temperatures (37°C produces near-complete conversion in weeks; 4°C nearly halts it). Commercial Manuka producers typically warm-store fresh honey at controlled elevated temperatures (around 27-37°C) for several months to drive the conversion before bottling. The final MGO level is essentially fixed by the starting DHA concentration in the nectar — you cannot make a 100+ MGO honey into a 500+ by storing it longer.
This explains several otherwise puzzling features of the Manuka market:
- Two-tier label — many premium brands print both "MGO" and "DHA" content. The DHA number represents the residual conversion potential. A honey with high DHA and modest MGO will increase in MGO with time; a honey with all DHA already converted is at its peak.
- Honest "best-before" dates — unlike most foods where "use-by" is downside protection against spoilage, Manuka actually peaks in MGO mid-shelf-life.
- Fraud opportunity — an unscrupulous producer can spike DHA-poor honey with synthetic DHA and produce a high-MGO product that lacks the other authenticity markers of real Manuka. The MPI definition (below) was developed specifically to detect this.
Mechanism: How MGO Kills Bacteria
Methylglyoxal is a reactive electrophile — one of the most reactive small molecules in human biology. It is also produced endogenously as a side-reaction of glycolysis (which is why every aerobic organism has a glyoxalase detoxification system to scavenge it). At the concentrations present in even modestly-rated Manuka (100+ mg/kg = 100+ ppm), MGO produces sustained, broad-spectrum bactericidal activity through several overlapping mechanisms:
- Protein alkylation — MGO reacts with arginine, lysine, and cysteine side chains, forming advanced glycation end-products (AGEs) on bacterial cell-surface and structural proteins. The protein modifications inactivate enzymes essential to bacterial replication and disrupt membrane proteins.
- DNA modification — MGO reacts with guanine bases to form 3-(2-deoxy-beta-D-erythro-pentofuranosyl)-pyrimido[1,2-a]purin-10(3H)-one (the MG-dG adduct), an unrepairable lesion that blocks DNA replication.
- Biofilm disruption — the Maeda 2008 and Maddocks 2012 papers demonstrated that Manuka honey eradicates established Staphylococcus aureus and Streptococcus pyogenes biofilms on wound surfaces, a critical capability since biofilms are the primary reason chronic wounds resist standard antibiotic therapy.
- Synergy with the other three honey mechanisms — MGO works on top of the osmotic, peroxide, and acidic-pH effects of all honey. Manuka does not replace those mechanisms; it adds a fourth, potent direct-kill mechanism that ordinary honey lacks.
An important note on resistance: extensive in vitro work has failed to produce stable MGO-resistant mutants of clinically important bacteria. The proposed reason is that MGO acts through multiple non-specific protein and DNA targets simultaneously, leaving no single target for resistance mutations to address. This is in contrast to most antibiotics that target a single enzyme or pathway. The practical implication: Manuka and MRSA, Manuka and Pseudomonas aeruginosa, Manuka and Enterococcus, Manuka and ESBL-producing E. coli all show consistent in-vitro and in-vivo kill curves even when the same organisms are resistant to most pharmacy antibiotics. See the Wound Healing page for the topical applications this enables.
The Three Rating Systems (MGO, UMF, NPA)
Three rating systems coexist on the Manuka shelf. They measure essentially the same property in different ways:
- MGO (mg/kg) — the most direct measurement. Reports the actual measured methylglyoxal concentration in mg per kg of honey (equivalent to parts per million). Typical commercial range: MGO 30 (basic), MGO 100+ (entry premium), MGO 250+ (mid-premium), MGO 400+ (therapeutic-grade), MGO 550+ (high therapeutic), MGO 800+ and MGO 1,000+ (very-high-end therapeutic). The MGO trademark is held by the German producer Manuka Health New Zealand Ltd.
- UMF (Unique Manuka Factor) — the original rating system, developed by Peter Molan's lab at the University of Waikato in the 1990s. UMF compares the antibacterial activity of Manuka against a phenol standard in a zone-of-inhibition assay against Staphylococcus aureus. UMF 10+ is the minimum threshold for the trademarked UMF designation; UMF 15+ is therapeutic-grade; UMF 20+ and UMF 24+ are premium therapeutic. UMF licensing is administered by the Unique Manuka Factor Honey Association (UMFHA) in New Zealand. Modern UMF certification also requires testing for leptosperin and DHA content.
- NPA (Non-Peroxide Activity) — a generic descriptor for the antibacterial activity that remains after the hydrogen-peroxide-generating glucose oxidase is destroyed (typically by adding catalase or by heat-treating). NPA effectively isolates the MGO contribution. NPA values track UMF values closely (NPA 10 ≈ UMF 10).
The approximate conversion table that authoritative producers publish:
- MGO 83 ≈ UMF 5+ ≈ NPA 5+
- MGO 263 ≈ UMF 10+ ≈ NPA 10+
- MGO 514 ≈ UMF 15+ ≈ NPA 15+
- MGO 829 ≈ UMF 20+ ≈ NPA 20+
- MGO 1,200 ≈ UMF 24+ ≈ NPA 24+
Several other marketing labels exist (KFactor, Bio Active, TA, Plus rating) but are not standardized scientific measurements and should be treated with suspicion. If a jar does not show one of the three real ratings (MGO, UMF, or NPA), there is no way to compare its potency against anything else.
The New Zealand MPI Scientific Definition
Authentic monofloral Manuka honey was for years defined only by pollen content (melissopalynology), which was easy to fake and easy to dispute. In 2018, the New Zealand Ministry for Primary Industries (MPI) introduced a science-based regulatory definition that all honey exported from New Zealand and labeled "Manuka" must meet. The MPI definition requires five tests:
- 3-phenyllactic acid ≥ 400 mg/kg (monofloral) or ≥ 20 mg/kg (multifloral)
- 2'-methoxyacetophenone ≥ 5 mg/kg
- 2-methoxybenzoic acid ≥ 1 mg/kg
- 4-hydroxyphenyllactic acid ≥ 1 mg/kg
- DNA from Leptospermum scoparium — less than Cq 36 in a qPCR assay
All five tests must pass for "monofloral Manuka" certification. The thresholds were calibrated against known authentic Manuka samples and are difficult to fake by spiking with synthetic DHA, syrup adulteration, or pollen contamination. The MPI label on a jar (typically as an export certificate number or a "Made in New Zealand" mark backed by MPI testing) is the strongest single signal of authenticity available to consumers.
Australian Manuka honey (from Tasmanian and Victorian Leptospermum scoparium as well as several closely related Australian Leptospermum species) is not covered by the MPI definition. The Australian Manuka Honey Association (AMHA) maintains a parallel standard, but the New Zealand industry contests the use of the word "Manuka" by Australian producers in international markets. From a chemical and clinical-efficacy standpoint, both sources produce high-MGO honey.
Choosing the Right MGO Strength for Each Application
The simplest rule: lower MGO for oral use, higher MGO for topical wound use. Specifically:
- Cough, sore throat, daily oral health — MGO 100+ to MGO 250+ (UMF 10+ to UMF 15+) is more than sufficient. Higher MGO is wasted in this application because oral mucosa is well-perfused, the contact time is short, and the cost premium is large.
- Gastrointestinal use (e.g. occasional support for the gut) — MGO 250+ to MGO 400+ (UMF 15+ to UMF 17+). Higher is acceptable but not necessary; the honey is diluted in the GI tract regardless.
- Topical use on minor wounds, abrasions, eczema — MGO 400+ (UMF 17+) and up. This is the threshold at which topical antibacterial activity is reliably superior to ordinary honey.
- Chronic wounds, burns, ulcers — in clinical settings, use the FDA-cleared Manuka dressings (Medihoney, Activon) rather than a food jar. Hospital-grade Manuka medical-device products are gamma-irradiated to eliminate Clostridium spores, packaged sterile, and standardized to high MGO concentrations equivalent to MGO 550+ to 800+.
- MGO 800+ and above — these are luxury-tier products. The clinical evidence for any incremental benefit over MGO 400+ in real use is thin. Most of the price difference reflects scarcity, not therapeutic advantage.
Avoiding Fraud and Watered-Down Manuka
The Manuka market has historically been plagued by fraud. Global sales of products labeled "Manuka" routinely exceed the entire New Zealand annual harvest by 3-to-1 or more — meaning the majority of jars on global shelves at any given time are partly or wholly counterfeit. Defenses against fraud:
- Buy from New Zealand or Australia, labeled with country of origin clearly visible
- Require one of the three real ratings (MGO, UMF, or NPA) on the label, with a specific number
- Prefer UMF-certified products, as the UMF Honey Association independently audits the chemistry of every batch
- For New Zealand product, look for the MPI export certificate or an explicit statement that the honey meets the MPI five-test definition for monofloral Manuka
- Be suspicious of "Manuka blend" or "Manuka with other floral sources" labels — these often contain very small fractions of real Manuka mixed with ordinary clover or rapeseed honey
- Be suspicious of unusually low prices — authentic UMF 15+ Manuka retails for approximately $40-60 USD per 250g jar in 2026
- Be aware that "Active 12+" or "Total Activity 16+" can include the hydrogen-peroxide activity present in all honey, not just the non-peroxide Manuka activity — these inflated numbers are misleading
For a deeper discussion of raw vs pasteurized labeling and other honey label terms, see the separate page in this Benefits hub.
Australian vs New Zealand Manuka
Australian Leptospermum honey is chemically equivalent to New Zealand Manuka in terms of MGO content and antibacterial activity. The dispute is about the word "Manuka" itself, which has Maori linguistic and cultural roots in New Zealand and which the New Zealand industry has sought to protect as a geographical indication (analogous to "Champagne" or "Roquefort" in Europe).
From a clinical/therapeutic standpoint, an MGO-400 honey from Tasmania or Victoria is interchangeable with an MGO-400 honey from the Coromandel Peninsula. From a fraud-defense standpoint, the New Zealand product currently has the more developed regulatory framework (MPI five-test definition + UMF certification), and the Australian framework (AMHA) is catching up. Either is fine; both are vastly preferable to honey labeled "Manuka" sourced from third countries with no Leptospermum trees.
Cautions
- Infant botulism — absolute contraindication under 12 months — this applies to Manuka exactly as it applies to all honey. Food-grade Manuka honey is not gamma-irradiated and can contain Clostridium botulinum spores. Never give any honey, including Manuka, to a child under 12 months old. The only exception is hospital medical-grade Manuka dressings, which are gamma-irradiated and labeled sterile — these are not for oral use.
- Diabetes management — Manuka honey is approximately 80% sugar (mostly fructose and glucose). The glycemic load is real and must be counted. For oral use in cough or sore throat, the small spoonful dose is rarely a problem; for daily multi-tablespoon supplementation, it should be calculated into total carbohydrate intake. See the Diabetes page for context.
- Cost — high-MGO Manuka is one of the most expensive foods sold by weight. For applications where ordinary honey is sufficient (oral coughs, sweetener replacement), there is no reason to use Manuka.
- Allergy — honey allergy is rare but can include anaphylaxis, especially in individuals sensitized to bee venom proteins or specific pollens. People with documented honey allergy should avoid Manuka as well as ordinary honey.
- Dental caries — despite some marketing claims, Manuka honey is a fermentable sugar in the oral cavity and supports cariogenic bacterial growth on tooth surfaces. Brush after consumption; do not let a child fall asleep with honey on a pacifier.
- Drug interactions — Manuka has not been documented to interact with prescription medications at oral doses. Topical application to wounds in patients on systemic antibiotics is not contraindicated and may be synergistic.
Key Research Papers
- Mavric E, Wittmann S, Barth G, Henle T (2008). Identification and quantification of methylglyoxal as the dominant antibacterial constituent of Manuka honey from New Zealand. Molecular Nutrition & Food Research. — Search PubMed
- Adams CJ, Manley-Harris M, Molan PC (2009). The origin of methylglyoxal in New Zealand manuka (Leptospermum scoparium) honey. Carbohydrate Research. — Search PubMed
- Adams CJ et al. (2008). Isolation by HPLC and characterisation of the bioactive fraction of New Zealand manuka honey. Carbohydrate Research. — Search PubMed
- Allen KL, Molan PC, Reid GM (1991). A survey of the antibacterial activity of some New Zealand honeys. Journal of Pharmacy and Pharmacology. PubMed: Allen-Molan 1991
- Molan PC (1992). The antibacterial activity of honey: the nature of the antibacterial activity. Bee World. PubMed: Molan 1992
- Atrott J, Henle T (2009). Methylglyoxal in Manuka honey — correlation with antibacterial properties. Czech Journal of Food Sciences. PubMed: Atrott-Henle 2009
- Stephens JM et al. (2010). Phenolic compounds and methylglyoxal in some New Zealand manuka and kanuka honeys. Food Chemistry. PubMed: Stephens 2010
- Maeda Y et al. (2008). Manuka honey eradicates established biofilms of Staphylococcus aureus. PubMed: Maeda biofilms
- Maddocks SE et al. (2012). Manuka honey inhibits the development of Streptococcus pyogenes biofilms. Journal of Medical Microbiology. PubMed: Maddocks Streptococcus
- Carter DA et al. (2016). Therapeutic Manuka Honey: No Longer So Alternative (review). Frontiers in Microbiology. — Search PubMed
- Roberts AEL, Maddocks SE, Cooper RA (2015). Manuka honey reduces the motility of Pseudomonas aeruginosa. PubMed: Roberts manuka and Pseudomonas
- Cokcetin NN et al. (2016). The antibacterial activity of Australian Leptospermum honey correlates with methylglyoxal levels. PLOS ONE. — Search PubMed
PubMed Topic Searches
- PubMed: MGO and Manuka antibacterial
- PubMed: Manuka and MRSA wound
- PubMed: Manuka and biofilms
- PubMed: Leptospermum nectar DHA
- PubMed: UMF rating
Connections
- Honey Main Page
- Honey Benefits Hub
- Raw vs Pasteurized
- Wound Healing Topical
- Cough Suppressant Evidence
- Wound Care
- Burns
- MRSA
- Pseudomonas aeruginosa
- Diabetes (Foot Ulcer)
- Immune Boosting
- Remedies
- All Food
- Tea Tree (Melaleuca)