Honey for Wound Healing — Topical Use, Burns, and Chronic Ulcers
Honey is one of the oldest wound dressings on the planet — the Smith Papyrus (circa 1600 BCE Egypt) describes its use, as do early Greek, Roman, and Arabic medical texts. Modern medicine abandoned honey in the 1940s with the arrival of antibiotics, then rediscovered it in the 1990s and 2000s as antibiotic resistance accelerated and chronic wound rates climbed with diabetes prevalence. Today, FDA-cleared 510(k) medical-grade Manuka honey dressings (Medihoney, Activon) are standard in hospital wound-care formularies in the US, UK, Australia, and across the EU. The Cochrane Collaboration's 2015 systematic review of 26 randomized trials (3,011 participants) found honey superior to standard treatments for partial-thickness burns and competitive with conventional dressings for chronic wounds. Four mechanisms work together — osmotic dehydration, hydrogen peroxide release, low pH, and (in Manuka) direct methylglyoxal bactericidal kill — and the combination has documented efficacy against MRSA, Pseudomonas aeruginosa, and other multidrug-resistant pathogens that increasingly defeat conventional antibiotic therapy.
Table of Contents
- History: From Smith Papyrus to FDA 510(k)
- The Four Wound-Healing Mechanisms
- FDA-Cleared Medical-Grade Manuka Dressings
- Burns — Partial-Thickness
- Chronic Ulcers (Diabetic Foot, Venous Leg, Pressure)
- MRSA, Pseudomonas, and Antibiotic-Resistant Pathogens
- Why Honey Disrupts Biofilms (and Why That Matters)
- Practical Application: Home Use vs Hospital Use
- Where Honey Should Not Be Used
- Cautions
- Key Research Papers
- Connections
- Featured Videos
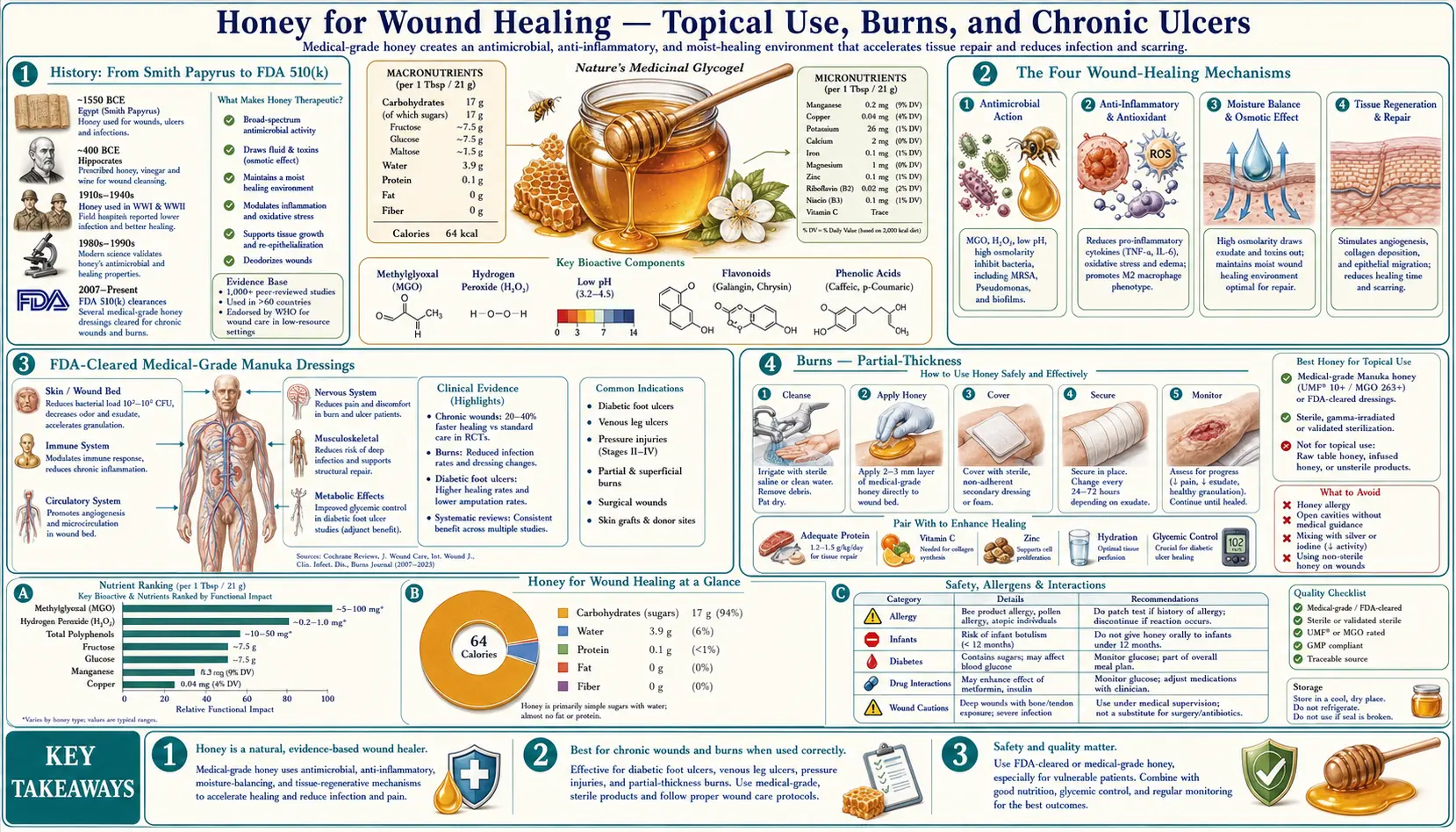
History: From Smith Papyrus to FDA 510(k)
The Edwin Smith Papyrus, an Egyptian surgical text dated to approximately 1600 BCE and itself a copy of an older work, describes 48 cases of traumatic injury and includes detailed instructions for the application of honey to wounds. Honey, lint, and grease are the recurring topical agents. Hippocrates, Aristotle, Galen, and Dioscorides all wrote on the wound-healing properties of honey. Through the medieval period and into the early 20th century, honey-based dressings (often combined with cod liver oil or wax) were standard surgical practice across European, Arabic, Indian, and Chinese medical traditions.
The arrival of penicillin in the 1940s and the broader antibiotic revolution that followed displaced honey almost entirely. By the 1960s, mainstream Western medicine viewed honey-on-wounds as a discredited folk remedy. The exception was Russian and Eastern European surgical practice, where honey continued to see use, and parts of the developing world where antibiotic access was limited.
The modern rediscovery began in New Zealand in the 1980s and 1990s. Peter Molan at the University of Waikato published a long series of papers characterizing the antibacterial activity of New Zealand honeys, leading to the identification of methylglyoxal as the dominant non-peroxide active in Manuka (Mavric et al. 2008) and the development of the UMF rating system. See the Manuka rating page for the chemistry.
The first medical-grade Manuka product to gain regulatory clearance was Medihoney, developed in Australia and FDA-cleared as a 510(k) medical device in the United States in 2007 for the management of moderately to heavily exuding wounds including diabetic foot ulcers, leg ulcers, pressure ulcers, and partial-thickness burns. Other products followed: Activon (Advancis Medical, UK), MelMax (BioMed, Netherlands), various country-specific formulations. By the late 2010s, Manuka honey dressings were a standard tool in chronic wound clinics across the developed world.
The Four Wound-Healing Mechanisms
The therapeutic effect of honey on wounds emerges from four overlapping mechanisms that act simultaneously. Understanding all four explains why different honeys produce different effects, why pasteurized honey is partly inactive, and why the medical-grade products work even after gamma irradiation.
- Osmotic dehydration of bacteria — honey has water activity (aw) below 0.6, well under the 0.85 threshold most bacteria require for growth. When honey is applied to a wound, the steep osmotic gradient draws water out of bacterial cells and out of the wound bed, simultaneously dehydrating contaminating bacteria and producing the moist (but not wet) environment that supports keratinocyte migration and tissue healing. This mechanism is present in any unadulterated honey, raw or pasteurized.
- Hydrogen peroxide generation — bee-derived glucose oxidase (GOx), suspended inactive in concentrated honey, becomes active when honey is diluted by wound exudate. GOx oxidizes glucose to gluconic acid and hydrogen peroxide. The peroxide is generated slowly, at low concentration (around 1 mmol/L), and continuously — achieving sustained bactericidal activity without the tissue toxicity of pharmacy-grade 3% (~880 mmol/L) hydrogen peroxide. This mechanism is destroyed by pasteurization: GOx is heat-labile. It is also the reason Manuka medical-grade products do not rely on this mechanism — gamma irradiation used to sterilize hospital product also reduces GOx activity, but Manuka's heat- and irradiation-stable MGO carries the load.
- Low pH — honey is acidic (pH 3.2-4.5). Applied to a wound, it acidifies the wound bed. This inhibits bacterial protease activity, releases oxygen from hemoglobin (improving local tissue oxygenation), and shifts the wound milieu toward conditions favorable to fibroblast and keratinocyte function. The pH effect is heat-stable and present in pasteurized honey.
- Methylglyoxal (MGO) direct kill — Manuka only — the methylglyoxal that distinguishes Manuka from other honeys produces a fourth mechanism: direct alkylation of bacterial proteins and DNA. At Manuka concentrations of 100+ mg/kg MGO and above, this mechanism is bactericidal against essentially all clinically important wound pathogens, including those resistant to most antibiotics. MGO is heat-stable and gamma-irradiation-stable, which is what enables manufacture of sterile medical-grade Manuka dressings.
Beyond the four direct antimicrobial mechanisms, honey also produces secondary wound-healing effects that are increasingly well-documented: stimulation of keratinocyte and fibroblast proliferation, autolytic debridement (the osmotic gradient pulls necrotic tissue away from the wound bed), reduction of wound odor (by reducing the bacterial production of ammonia and short-chain fatty acids), and reduction of edema and inflammation.
FDA-Cleared Medical-Grade Manuka Dressings
Medical-grade Manuka honey differs from food-grade Manuka in three important ways:
- Gamma irradiation — food-grade honey can contain Clostridium botulinum spores (the infant-botulism risk). Medical-grade Manuka for wound application is gamma-irradiated (typically 25 kGy) to eliminate spores. This is critical for application to deep wounds or wounds in patients with compromised gut motility.
- Standardized MGO concentration — medical-grade product is tested and labeled to a specific MGO level, typically equivalent to UMF 18+ or MGO 700+ for premium hospital products.
- Pharmaceutical packaging — sterile single-use packets, impregnated dressings (gauze, alginate, hydrogel matrix), gels in sterile tubes. The presentation matches existing wound-care workflow.
The major commercially available product lines:
- Medihoney (Derma Sciences / Integra LifeSciences, US) — the original FDA-cleared product. Available as paste, gel, alginate dressing, calcium alginate, hydrocolloid, and impregnated foam. The dressings are the workhorses of US hospital chronic-wound clinics.
- Activon (Advancis Medical, UK) — 100% sterile Manuka honey in a tube and as an impregnated tulle dressing. Used heavily in UK NHS wound care.
- MelMax (BioMed) — the European competitor, distributed across the EU.
- Various national-formulary products — Australia, New Zealand, and several other countries have domestic Manuka medical-device products.
All of these products are intended for use under standard wound-care protocols, typically by a wound-care nurse or wound-care physician, applied at dressing changes every 1-3 days depending on exudate volume.
Burns — Partial-Thickness
Burns are the application with the most consistent clinical evidence for honey. The 2015 Cochrane review (Jull et al.) pooled 26 trials with 3,011 participants and found that honey was significantly better than standard wound dressings (paraffin gauze, polyurethane film, hydrogels) for partial-thickness burns, reducing time to healing by an average of 4-5 days. The classic Indian RCT by Subrahmanyam (1991) randomized 104 patients with partial-thickness burns to honey-impregnated gauze vs silver sulfadiazine cream and found honey-treated patients healed faster (average 10.8 vs 15.3 days), had fewer infections, and had less scarring.
The mechanism explanation is straightforward: partial-thickness burns expose a large surface area, are heavily exudative, and are at high risk of bacterial colonization that delays healing or progresses to deep infection. Honey's broad-spectrum antimicrobial activity prevents the colonization, the osmotic effect absorbs exudate without sticking to the wound bed, and the moist environment supports keratinocyte migration from the wound edges and from preserved epidermal islands in the burn bed.
Practical considerations for partial-thickness burns:
- First-degree burns (sunburn, erythema only) do not need honey or any other dressing
- Superficial partial-thickness burns (blistering, painful, blanching) are where honey shines — medical-grade Manuka with a non-adherent dressing, changed every 2-3 days
- Deep partial-thickness and full-thickness burns require surgical evaluation and are typically managed with skin grafts; honey may be used as an adjunct but not as monotherapy
- Any burn larger than the patient's palm, on the face/hands/genitals, or with signs of infection should be evaluated by a clinician
For more on burns generally, see the Burns page.
Chronic Ulcers (Diabetic Foot, Venous Leg, Pressure)
Chronic ulcers are the largest market for medical-grade Manuka. They share three problematic features: they are colonized or infected with biofilm-forming bacteria, they fail to progress through normal wound-healing phases, and they often co-occur in patients with diabetes, peripheral vascular disease, or immobility. Conventional treatments (silver dressings, antimicrobial alginates, negative-pressure wound therapy) are effective but expensive and do not always work.
Manuka honey dressings have established efficacy in:
- Diabetic foot ulcers — multiple RCTs and the HALT trial subgroup demonstrate that Manuka dressings produce faster reduction in wound size and lower rates of infection compared to conventional dressings. The infection-prevention effect is particularly valuable because diabetic foot infections are the leading cause of non-traumatic lower-extremity amputation. See the Diabetes page for context.
- Venous leg ulcers — the HALT (Honey as Adjuvant Leg Ulcer Therapy) trial in New Zealand was the largest RCT (n=368) of Manuka for venous leg ulcers. Results were mixed — complete healing rates at 12 weeks were similar between Manuka and standard care, but the Manuka group had significantly lower MRSA colonization rates and faster eradication of existing infection. Manuka is now part of NHS guidelines as an option for venous leg ulcers, particularly those colonized with MRSA.
- Pressure ulcers (bedsores) — smaller trials suggest faster healing with Manuka than with hydrocolloid or saline-soaked gauze. The osmotic debridement effect is particularly valuable for stage 2-3 pressure ulcers with necrotic slough.
- Post-surgical wound dehiscence — case series support Manuka for surgical wounds that have re-opened, particularly when contaminated.
The typical regimen: Manuka dressing applied at every standard dressing change (1-3 days), continued until the wound has filled with granulation tissue and shrunk to closure. Cost per dressing is several US dollars — expensive compared to saline gauze but cheaper than long courses of systemic antibiotics or hospital admission for infection.
MRSA, Pseudomonas, and Antibiotic-Resistant Pathogens
One of the strongest arguments for honey in modern wound care is its activity against pathogens that defeat most conventional antibiotics:
- MRSA (methicillin-resistant Staphylococcus aureus) — Manuka honey produces complete kill of MRSA at in-vitro concentrations of 5-10% (v/v). The Cooper et al. 2002 paper and many subsequent papers have demonstrated that all clinical MRSA isolates tested remain susceptible to Manuka honey. See the MRSA page.
- Pseudomonas aeruginosa — one of the most problematic gram-negative wound pathogens, especially in burns and chronic ulcers. The Cooper 1999 paper demonstrated Manuka activity against burn-derived Pseudomonas isolates. The Roberts 2015 paper showed Manuka reduces Pseudomonas motility, an important virulence factor. See the Pseudomonas page.
- VRE (vancomycin-resistant enterococci) — in-vitro activity demonstrated.
- ESBL-producing Escherichia coli — in-vitro activity demonstrated, including against carbapenem-resistant strains.
- Acinetobacter baumannii — an emerging burn/ICU pathogen with frequent multidrug resistance. Manuka shows in-vitro activity, with limited clinical data so far.
- Mycobacteria — in-vitro activity against M. tuberculosis, M. abscessus, and atypical mycobacteria has been demonstrated, but clinical use is exploratory.
The key feature is that extensive in-vitro work has failed to produce stable Manuka-resistant mutants of clinically important pathogens. The proposed reason: MGO acts through multiple non-specific protein and DNA targets simultaneously, leaving no single target for resistance mutations to address. This is unlike most antibiotics, which target a single enzyme or pathway and accumulate resistance with use.
Why Honey Disrupts Biofilms (and Why That Matters)
Biofilms are bacterial communities encased in a self-produced extracellular polymeric matrix. Within a biofilm, bacterial metabolic activity is reduced, antibiotic penetration is poor, and the community as a whole is up to 1,000-fold less susceptible to antibiotics than the same bacteria in planktonic (free-swimming) form. Biofilms are the primary reason chronic wounds become and stay chronic — ordinary antibiotic courses do not penetrate the matrix to kill the embedded bacteria, and as soon as the antibiotic is withdrawn, the biofilm regrows.
Honey, and especially Manuka honey, has documented biofilm-disrupting activity. The Maeda 2008 paper demonstrated that Manuka honey eradicates established Staphylococcus aureus biofilms in vitro. The Maddocks 2012 paper showed similar effect on Streptococcus pyogenes biofilms. The proposed mechanisms include osmotic disruption of the matrix, direct MGO penetration through the matrix, and methylglyoxal-induced downregulation of biofilm-formation gene expression.
The clinical implication: a chronic wound that has been managed for months with systemic antibiotics with no resolution can sometimes be turned around by sustained Manuka honey topical application, which addresses the biofilm component that the systemic antibiotics could not reach.
Practical Application: Home Use vs Hospital Use
For minor wounds, abrasions, small superficial burns, and skin irritations that an individual might manage at home:
- Clean the wound with saline or clean water
- Apply a thin layer of MGO 400+ (UMF 17+) Manuka honey to the wound surface
- Cover with a non-adherent dressing (Telfa, hydrocolloid, or similar)
- Change the dressing every 24-48 hours, reapplying honey as needed
- Continue until the wound is closed and healed
- Discontinue and seek clinician evaluation if the wound shows signs of infection (expanding redness, warmth, increasing pain, fever, purulent discharge) or fails to progress within 1-2 weeks
For wounds that require professional management (chronic ulcers, deep wounds, burns larger than a palm, infected wounds, wounds in patients with diabetes or compromised immunity):
- Seek wound-care clinic evaluation
- Medical-grade Manuka products (Medihoney, Activon) are standard in formularies and are gamma-irradiated to eliminate C. botulinum spore risk
- Application is by a wound-care nurse following an individualized care plan
- Insurance coverage is generally available for medical-grade honey dressings under wound-care benefits
For minor wounds, food-grade Manuka is acceptable. For wounds in immunocompromised patients, for deep wounds, or for any wound that breaches the skin into deeper tissue, only medical-grade (gamma-irradiated, sterile) honey should be used. See the Wound Care page for general wound management.
Where Honey Should Not Be Used
- Deep penetrating wounds — honey should not be packed into deep cavity wounds that communicate with body cavities (e.g. abdominal, thoracic) without surgical evaluation
- Internal application — honey is for topical and oral use only; it should never be injected, instilled into the bladder or peritoneum, or used as eye drops without specific medical-device clearance for that application
- Patients with documented honey allergy or bee-venom anaphylaxis
- Infants and toddlers under 12 months — do not apply honey to skin abrasions in this age group; food-grade honey can release spores into the environment, and infants can ingest topical honey through hand-mouth contact
- Wounds with active heavy bleeding — honey is not a hemostatic agent; standard hemostasis must be achieved first
- Necrotic eschar — honey can soften and debride eschar over time, but it is not a substitute for sharp surgical debridement when that is indicated
Cautions
- Infant botulism — topical application — food-grade honey applied to the skin of an infant under 12 months poses risk because the infant can ingest honey through hand-mouth contact or mouthing of the dressing. Use only medical-grade gamma-irradiated Manuka in this age group, and only under clinician direction.
- Transient burning or stinging — some patients report a brief stinging sensation at application, lasting 5-30 minutes. This is attributed to the osmotic effect on exposed nerve endings and the low pH. It resolves with continued use and is not a sign of harm.
- Increased exudate volume initially — the osmotic effect can transiently increase wound exudate as fluid is drawn from the wound bed. Dressing absorbency should be matched to this; check and change dressings more frequently in the first 24-48 hours of honey therapy.
- Honey allergy — rare. Contact dermatitis from topical honey has been reported, including in patients with no oral honey allergy. Stop use and consult a clinician if a rash develops at the dressing site.
- Glycemic effect from absorption — topically applied honey on small wounds does not produce systemic glycemic effects. Large-area application (e.g. extensive burns) in diabetic patients may produce measurable glucose absorption; this should be monitored.
- Drug interactions — no documented topical honey drug interactions. Concurrent systemic antibiotic therapy is not contraindicated and may be synergistic.
- Cost — medical-grade Manuka dressings are expensive. They are most cost-effective for chronic wounds where the alternative is months of failed conventional therapy or progression to amputation.
Key Research Papers
- Jull AB, Cullum N, Dumville JC, Westby MJ, Deshpande S, Walker N (2015). Honey as a topical treatment for wounds. Cochrane Database of Systematic Reviews. — Search PubMed
- Subrahmanyam M (1991). Topical application of honey in treatment of burns. British Journal of Surgery. — Search PubMed
- Molan PC, Rhodes T (2015). Honey: A Biologic Wound Dressing. Wounds. — PubMed: PMID 26061489
- Cooper RA, Halas E, Molan PC (2002). The efficacy of honey in inhibiting strains of Pseudomonas aeruginosa from infected burns. Journal of Burn Care & Rehabilitation. PubMed: Cooper 2002
- Cooper RA, Molan PC, Harding KG (2002). The sensitivity to honey of Gram-positive cocci of clinical significance isolated from wounds. Journal of Applied Microbiology. — Search PubMed
- Maeda Y, Loughrey A, Earle JA et al. (2008). Antibacterial activity of honey against community-associated methicillin-resistant Staphylococcus aureus. Complementary Therapies in Clinical Practice. PubMed: Maeda MRSA
- Maddocks SE, Lopez MS, Rowlands RS, Cooper RA (2012). Manuka honey inhibits the development of Streptococcus pyogenes biofilms and causes reduced expression of two fibronectin binding proteins. Microbiology. — Search PubMed
- Carter DA, Blair SE, Cokcetin NN et al. (2016). Therapeutic Manuka Honey: No Longer So Alternative. Frontiers in Microbiology. — Search PubMed
- Roberts AEL, Maddocks SE, Cooper RA (2015). Manuka honey reduces the motility of Pseudomonas aeruginosa by suppression of flagella-associated genes. Journal of Antimicrobial Chemotherapy. PubMed: Roberts manuka motility
- Jull A, Walker N, Parag V, Molan P, Rodgers A (2008). Randomized clinical trial of honey-impregnated dressings for venous leg ulcers (HALT trial). British Journal of Surgery. — PubMed: PMID 18161896
- Molan P (2009). The evidence and the rationale for the use of honey as wound dressing. Wound Practice and Research. PubMed: Molan rationale
- Yaghoobi R, Kazerouni A, Kazerouni O (2013). Evidence for clinical use of honey in wound healing as an anti-bacterial, anti-inflammatory anti-oxidant and anti-viral agent: A review. Jundishapur Journal of Natural Pharmaceutical Products. — PubMed: PMID 24624197
PubMed Topic Searches
- PubMed: Honey wound healing clinical
- PubMed: Manuka and MRSA chronic wound
- PubMed: Manuka diabetic foot ulcer
- PubMed: Honey partial-thickness burns
- PubMed: Manuka biofilm
Connections
- Honey Main Page
- Honey Benefits Hub
- Manuka and MGO Rating
- Raw vs Pasteurized
- Cough Suppressant Evidence
- Wound Care
- Burns
- MRSA
- Pseudomonas aeruginosa
- Diabetes Foot Ulcer
- Eczema
- Remedies
- Immune Boosting
- All Food