Avocado Potassium and Blood Pressure — The Sodium-Potassium Axis
A medium Hass avocado contains approximately 975 mg of potassium — roughly 2.3× what a medium banana provides (~422 mg), and one of the highest single-fruit potassium loads available in the supermarket. The relevance: dietary potassium has direct blood-pressure-lowering effects through the kidney's sodium-potassium exchange system, and the current understanding is that the sodium-to-potassium ratio of the diet is a stronger predictor of cardiovascular outcomes than sodium alone. The PURE study of 100,000+ adults across 17 countries found that low potassium intake was as predictive of cardiovascular death as high sodium intake. The WHO recommends 3,510 mg/day of potassium; the US adequate intake is 3,400 mg for men and 2,600 mg for women. Most Americans consume roughly half the recommended amount, while consuming 1.5-2× the recommended sodium. This page covers the mineral chemistry, the renal mechanism, the DASH and PREDIMED trial evidence, the specific calculation of avocado's contribution to a potassium-adequate diet, and the important kidney-disease caution where high-potassium foods become hazardous.
Table of Contents
- Why Avocado Is Potassium-Dense
- The Renal Sodium-Potassium Exchange Mechanism
- The DASH Trial and Dietary Pattern Evidence
- Sodium-to-Potassium Ratio — The Better Marker
- The Filippini Dose-Response Meta-Analysis
- Mechanisms Beyond the Kidney
- How Avocado Fits Daily Potassium Targets
- Comparison to Other Potassium-Rich Foods
- Critical Caution: Chronic Kidney Disease
- Other Cautions and Edge Cases
- Key Research Papers
- Connections
- Featured Videos
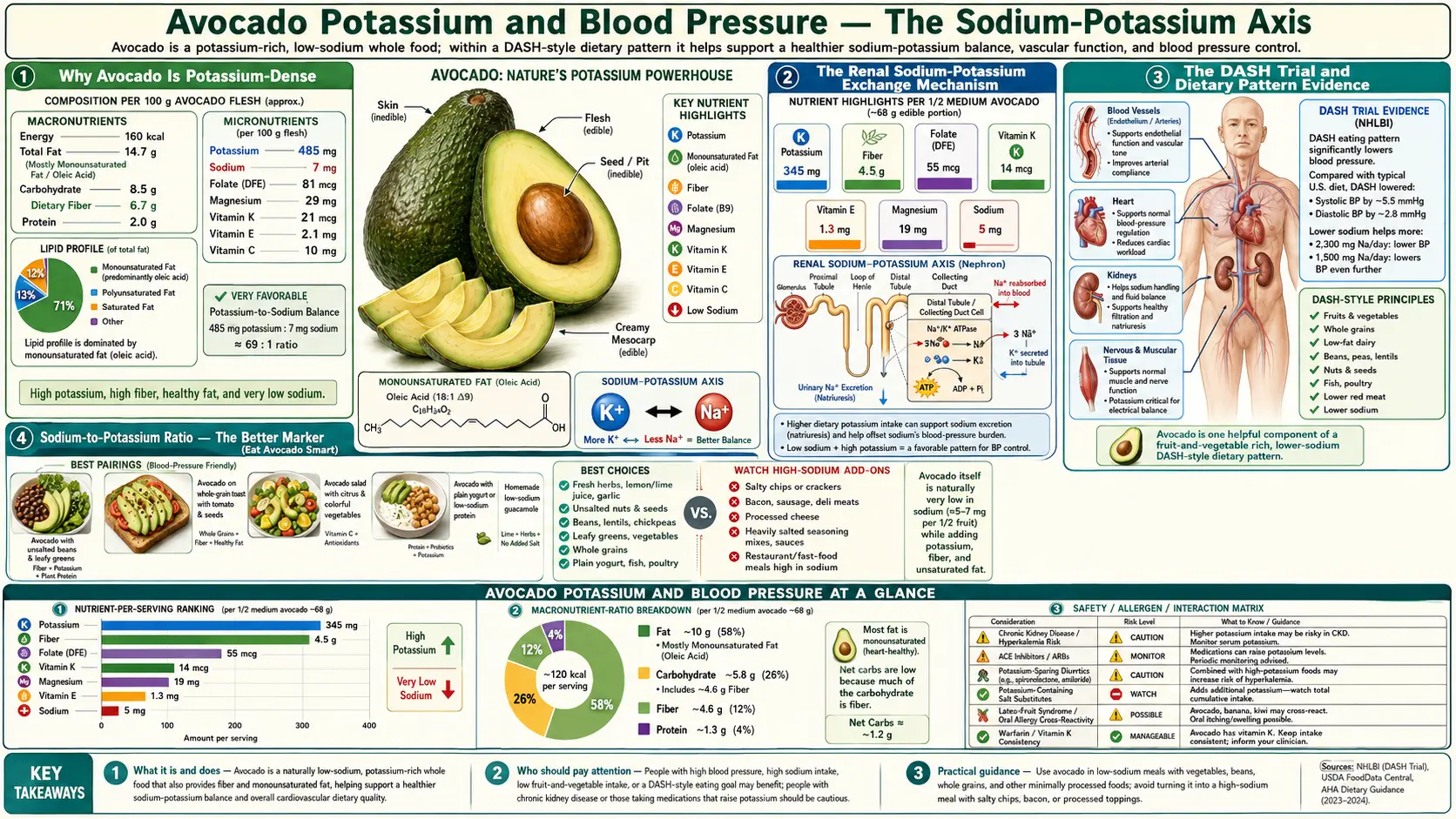
Why Avocado Is Potassium-Dense
The potassium-density of avocado is genuinely unusual in the fruit category. Most fruits are dominated by water and simple sugars, with mineral content typically modest. Avocado's low water content (~73% vs ~85% for most fruits) and very low sugar content (~0.5 g per fruit vs ~12-25 g for most fruits) leave room for higher mineral density per gram of food.
Per medium Hass avocado (~200 g edible flesh):
- Potassium: 975 mg — approximately 28% of the WHO 3,510 mg/day target
- Sodium: ~14 mg — trivially low (the desirable direction)
- Magnesium: ~58 mg — approximately 14% of RDA
- Phosphorus: ~104 mg
- Copper: ~0.4 mg — approximately 44% of RDA, a meaningful copper source
- Manganese: ~0.3 mg
- Calcium: ~24 mg — modest
- Iron: ~1.1 mg — modest, non-heme form
- Zinc: ~1.3 mg
The 975 mg potassium / 14 mg sodium ratio of 70:1 is dramatically favorable. By comparison, the typical American diet has a potassium-to-sodium ratio closer to 1:1, when the evolutionary-baseline ratio for hunter-gatherer diets is estimated at 10:1 or higher. Avocado consistently pushes the diet toward the ancestral ratio.
The Renal Sodium-Potassium Exchange Mechanism
The blood-pressure-lowering effect of dietary potassium is mediated primarily through the kidney's distal nephron. The principal cells of the distal convoluted tubule and collecting duct have two key transporters in the basolateral membrane: the Na+/K+-ATPase pump (which extrudes sodium into the interstitium and pumps potassium into the cell), and on the apical side, the epithelial sodium channel (ENaC) and the renal outer medullary potassium channel (ROMK).
The mechanism works as follows: when serum potassium rises in response to dietary potassium intake, aldosterone secretion from the adrenal gland is suppressed and intracellular signaling shifts to favor potassium secretion (via ROMK) and reduce sodium reabsorption (via ENaC downregulation). The result is increased urinary sodium excretion (natriuresis), which lowers extracellular fluid volume, which in turn lowers blood pressure.
This mechanism is mechanistically the same as the action of the potassium-sparing diuretic drugs (spironolactone, eplerenone, amiloride, triamterene) but achieved through dietary mineral intake. The effect size is smaller per dose but applied chronically across the population, dietary potassium produces meaningful blood pressure reductions documented in multiple meta-analyses.
A secondary mechanism: potassium induces direct vasodilation of small arterioles through hyperpolarization of vascular smooth muscle cells, mediated by potassium-channel activation. This local vasodilation contributes to the blood-pressure-lowering effect independently of the renal mechanism.
The DASH Trial and Dietary Pattern Evidence
The DASH (Dietary Approaches to Stop Hypertension) trial (Appel et al., NEJM 1997) is the seminal dietary intervention trial for blood pressure. 459 adults with systolic BP <160 mmHg and diastolic BP 80-95 mmHg were randomized to one of three controlled diets for 8 weeks:
- Control diet — typical US intake, ~3,500 mg sodium, ~1,700 mg potassium
- Fruit/vegetable diet — same sodium, ~4,700 mg potassium (achieved through 8-10 servings of fruits and vegetables daily)
- DASH combination diet — same sodium, ~4,700 mg potassium plus reduced saturated fat, increased low-fat dairy
Results in hypertensive participants:
- The DASH combination diet lowered systolic BP by 11.4 mmHg and diastolic BP by 5.5 mmHg compared to control
- The fruit/vegetable diet alone lowered systolic BP by 7.2 mmHg and diastolic by 2.8 mmHg — demonstrating that potassium-rich produce alone accounted for most of the effect
- Effects appeared within 2 weeks and stabilized by week 8
The DASH-Sodium follow-on trial (Sacks et al., NEJM 2001) added a sodium-restriction arm and confirmed that DASH + low sodium was additive — the lowest-sodium DASH arm achieved BP reductions comparable to single-drug antihypertensive therapy in hypertensive participants. This established the modern guideline recommendation of a DASH-style high-potassium, low-sodium diet as first-line non-pharmacologic therapy for hypertension.
Sodium-to-Potassium Ratio — The Better Marker
For decades the sodium content of the diet was the focus of hypertension prevention. More recent research has refined this view: the ratio of sodium to potassium appears to be a stronger predictor of cardiovascular outcomes than either mineral in isolation.
The Yang 2011 NHANES analysis (Archives of Internal Medicine) followed 12,267 US adults for a median of 14.8 years. Findings:
- Higher sodium-to-potassium ratio was associated with a 46% higher risk of cardiovascular mortality compared to lowest ratio quartile
- The association was stronger for the ratio than for either sodium or potassium considered alone
- The relationship held after adjustment for age, sex, race, BMI, diabetes, smoking, alcohol, education, and dietary energy intake
The interpretation: the cardiovascular system responds to the relative balance of these two minerals, not to the absolute amount of either. Reducing sodium intake is helpful; raising potassium intake is also helpful; doing both is best. A 4,000 mg sodium / 4,000 mg potassium diet may produce lower cardiovascular risk than a 2,000 mg sodium / 1,500 mg potassium diet, even though the sodium load is double, because the ratio is more favorable.
The clinical relevance for avocado: a single medium avocado adds 975 mg of potassium and only 14 mg of sodium — the ratio of added potassium-to-sodium is 70:1. Few common foods can shift the daily ratio as dramatically per serving.
The Filippini Dose-Response Meta-Analysis
Filippini et al. published in JAHA (2020) the most comprehensive dose-response meta-analysis of potassium supplementation trials. 32 randomized controlled trials with 2,609 participants were pooled. The dose-response relationship found:
- At low baseline potassium intakes (around 1,500-2,000 mg/day), each additional 1,000 mg/day reduced systolic BP by approximately 3.5 mmHg in hypertensive participants and 1.5 mmHg in normotensive participants
- The dose-response curve flattened above approximately 3,500 mg/day total intake — additional potassium beyond this had diminishing returns on blood pressure
- Effects were stronger in salt-sensitive populations (African ancestry, older adults, kidney-disease patients on appropriate monitoring)
- The blood-pressure-lowering effect was independent of sodium intake reduction
This dose-response curve is one of the bases for the WHO 3,510 mg/day target. The implication is that incrementally adding potassium-rich foods like avocado to a diet that is currently potassium-deficient (which describes most Western diets) produces a clinically meaningful blood pressure reduction.
Mechanisms Beyond the Kidney
Beyond the renal natriuretic effect, dietary potassium affects blood pressure through several additional pathways:
- Vascular smooth muscle relaxation — elevated extracellular potassium hyperpolarizes vascular smooth muscle cells via activation of inwardly-rectifying potassium channels (Kir) and the Na+/K+-ATPase. Hyperpolarized cells are less responsive to vasoconstrictor stimuli, producing relative vasodilation in resistance arterioles.
- Endothelial nitric oxide production — potassium-replete diets increase endothelial nitric oxide synthase (eNOS) activity, raising vascular NO availability and improving endothelium-dependent vasodilation. Endothelial dysfunction is one of the earliest measurable changes in hypertension and atherosclerosis.
- Reduced platelet aggregation — potassium-rich diets reduce platelet hyperaggregability seen in hypertensive patients, contributing to reduced thrombotic risk.
- Suppressed renin-angiotensin-aldosterone system (RAAS) — high potassium intake suppresses renin secretion from the juxtaglomerular apparatus, reducing the chronic vasoconstrictor and sodium-retentive drive of the RAAS axis.
- Reduced sympathetic nervous system tone — small reductions in sympathetic outflow to peripheral arterioles are documented with potassium repletion.
The multiple mechanisms acting in parallel explain why the cardiovascular benefit of dietary potassium extends beyond the modest absolute blood-pressure reduction — epidemiologic data shows reduced stroke, coronary events, and cardiovascular mortality at potassium-intake levels not fully accounted for by BP change alone.
How Avocado Fits Daily Potassium Targets
The WHO target of 3,510 mg/day potassium and the US adequate intake of 3,400 mg (men) / 2,600 mg (women) are reachable on a normal diet, but require deliberate effort. NHANES 2015-2018 data show median US adult potassium intake of approximately 2,500-2,800 mg/day, well below targets.
A practical "potassium-adequate" day might look like:
- Breakfast: 1/2 avocado on toast with two eggs — ~500 mg potassium
- Snack: medium banana — ~420 mg potassium
- Lunch: large mixed-green salad with 1/2 cup beans, 1/2 cup roasted sweet potato, and 1/2 avocado — ~1,400 mg potassium
- Snack: 1 cup plain Greek yogurt with 1/4 cup dried apricots — ~600 mg potassium
- Dinner: 4 oz salmon with roasted potato (medium, with skin) and 1 cup spinach — ~1,500 mg potassium
Total: ~4,400 mg potassium — comfortably above the WHO target. The avocado contributions in this example provide 975 mg, or roughly 28% of the WHO target, from one whole fruit divided across two meals.
For a person who does not eat potatoes, dairy, or beans, hitting 3,500 mg/day without avocado becomes meaningfully harder. Avocado is one of the few "calorie-efficient" potassium sources (per calorie, it delivers about 4 mg potassium, similar to leafy greens and beans, much better than starchy vegetables on a per-calorie basis).
Comparison to Other Potassium-Rich Foods
Per standard serving, ranked by potassium content:
- Baked potato with skin (1 medium, ~173 g): 941 mg
- Sweet potato (1 medium, ~150 g): 542 mg
- Acorn squash (1 cup cubed): 900 mg
- Avocado (1 medium Hass, 200 g flesh): 975 mg
- White beans (1 cup cooked): 1,189 mg
- Lima beans (1 cup cooked): 955 mg
- Cooked spinach (1 cup): 839 mg
- Cooked beet greens (1 cup): 1,309 mg
- Salmon, wild Atlantic (4 oz): 534 mg
- Plain yogurt (1 cup): 573 mg
- Banana (1 medium): 422 mg
- Orange (1 medium): 237 mg
- Tomato (1 medium): 292 mg
The often-cited "banana = potassium" association substantially underrates the actual ranking. Beans, leafy greens, potatoes, sweet potatoes, and avocados are all considerably better. Bananas are convenient and ubiquitous but not exceptional in this category.
For more on dietary potassium and the foods that deliver it, see our Potassium page and Mediterranean Diet page.
Critical Caution: Chronic Kidney Disease
The most important caveat on this entire page: the blood-pressure benefit of high-potassium foods assumes normal renal function. Patients with chronic kidney disease (CKD), particularly stages 3b-5, have impaired ability to excrete potassium and can develop life-threatening hyperkalemia from foods that healthy adults consume without issue.
- CKD stage 3b (eGFR 30-44): consult a renal dietitian for individualized potassium-intake limits. Avocado is often partially restricted.
- CKD stage 4 (eGFR 15-29): moderate-to-strict potassium restriction is typical, often capping intake at 2,000-3,000 mg/day. A whole avocado per day is generally not recommended.
- CKD stage 5 / dialysis: strict potassium restriction (~2,000-2,500 mg/day or per renal team). High-potassium foods including whole avocado, raw banana, potato, beans, and tomato paste are typically minimized.
Medications that elevate the risk: ACE inhibitors, ARBs, aldosterone receptor antagonists (spironolactone, eplerenone), potassium-sparing diuretics (amiloride, triamterene), NSAIDs (chronic use), trimethoprim/sulfamethoxazole, heparin, tacrolimus, cyclosporine, beta-blockers (modest effect). The combination of CKD + any of these drugs requires individualized potassium-intake guidance.
Hyperkalemia symptoms (weakness, palpitations, paresthesias, ECG changes) can be silent until severe; serum potassium monitoring is the only reliable safety check in at-risk patients. For more on chronic kidney disease management, see our CKD page.
Other Cautions and Edge Cases
- Adrenal insufficiency (Addison's disease) — without adequate aldosterone production, potassium excretion is impaired. High-potassium foods need cautious dosing with endocrinologist involvement.
- Type 4 renal tubular acidosis — aldosterone-resistant or pseudohypoaldosteronism conditions impair potassium excretion. Individualized management is required.
- Potassium supplements + avocado — patients prescribed potassium chloride supplements (e.g. K-Dur, Klor-Con) should account for dietary potassium when adjusting supplement dose. Often the goal of supplementation is to compensate for thiazide- or loop-diuretic-induced potassium loss; high dietary potassium intake can sometimes reduce the supplement requirement, but this should be done with the prescribing physician.
- Severe rhabdomyolysis or tumor lysis syndrome — acute massive cell death releases intracellular potassium and can cause life-threatening hyperkalemia. Dietary potassium adds to the load.
- Pre-eclampsia and pregnancy hypertension — DASH-style high-potassium dietary patterns are generally favorable in pregnancy and avocado consumption is reasonable for most pregnant women.
Key Research Papers
- Appel LJ et al. (1997). A clinical trial of the effects of dietary patterns on blood pressure (DASH). NEJM. — PubMed
- Sacks FM et al. (2001). Effects on blood pressure of reduced dietary sodium and the DASH-Sodium trial. NEJM. — PubMed
- Yang Q et al. (2011). Sodium and potassium intake and mortality among US adults: prospective data from NHANES III. Archives of Internal Medicine. — PubMed
- O'Donnell M et al. (2014). Urinary sodium and potassium excretion, mortality, and cardiovascular events (PURE Study). NEJM. — PubMed
- Aburto NJ et al. (2013). Effect of increased potassium intake on cardiovascular risk factors and disease: systematic review and meta-analyses. BMJ. — PubMed
- Filippini T et al. (2020). Potassium intake and blood pressure: a dose-response meta-analysis of randomized controlled trials. JAHA. — PubMed
- WHO (2012). Guideline: Potassium intake for adults and children. — PubMed
- Whelton PK et al. (2017). 2017 ACC/AHA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults. Hypertension. — PubMed
- Stone MS et al. (2016). Potassium intake, bioavailability, hypertension, and glucose control. Nutrients. — PubMed
- Cogswell ME et al. (2012). Sodium and potassium intakes among US adults: NHANES 2003-2008. AJCN. — PubMed
- Dreher ML, Davenport AJ (2013). Hass avocado composition and potential health effects. Critical Reviews in Food Science and Nutrition. — PubMed
- Kovesdy CP et al. (2017). Potassium homeostasis in health and disease: a scientific workshop. American Journal of Kidney Diseases. — PubMed
PubMed Topic Searches
- PubMed: Dietary potassium BP meta-analyses
- PubMed: Na:K ratio cardiovascular
- PubMed: DASH diet hypertension
- PubMed: Hyperkalemia CKD dietary management
- PubMed: Potassium stroke prevention
Connections
- Avocado Overview
- Avocado Benefits Hub
- Avocado Monounsaturated Fats
- Avocado Fiber & Satiety
- Avocado Skin & Carotenoids
- Potassium
- Magnesium
- Sodium
- Hypertension
- Stroke
- Chronic Kidney Disease
- Mediterranean Diet
- Sweet Potatoes
- Spinach
- Basic Metabolic Panel (Serum K+)
- All Food