Almonds for Magnesium and Bone Health
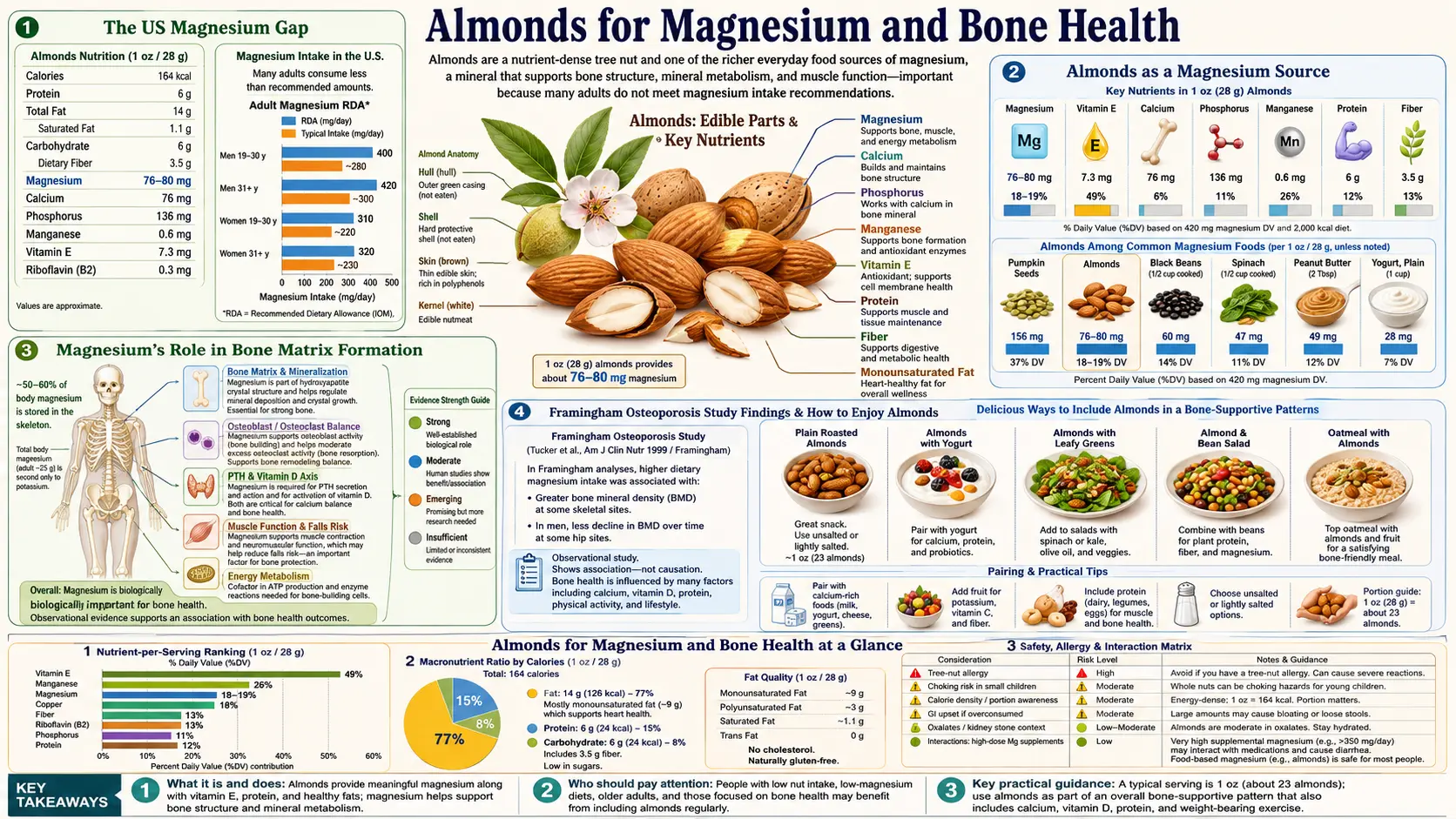
A single ounce of almonds delivers 76 mg of magnesium — 18% of the adult Daily Value and one of the highest snack-format magnesium densities in the food supply. Magnesium is the fourth-most-abundant cation in the body and is required for over 300 enzymatic reactions, including ATP hydrolysis, DNA and RNA synthesis, vitamin D activation, parathyroid hormone signaling, and the crystallization of hydroxyapatite into the mineral matrix of bone. The NHANES survey data show that most US adults consume 200-300 mg of magnesium per day against an RDA of 320 mg (women) to 420 mg (men) — the so-called "magnesium gap." Adding a daily ounce of almonds closes a meaningful fraction of that gap from a single whole-food source, with measurable downstream effects on bone mineral density (Framingham Osteoporosis Study), insulin sensitivity (PREDIMED, multiple observational cohorts), blood pressure (DASH diet trials and the Kass meta-analysis), and migraine frequency. This page walks through the magnesium-bone mechanism, the Framingham and related cohort data, the synergy with calcium and vitamin D, and the practical implications for adults at risk for osteoporosis or chronic magnesium insufficiency.
Table of Contents
- The US Magnesium Gap
- Almonds as a Magnesium Source
- Magnesium's Role in Bone Matrix Formation
- Framingham Osteoporosis Study Findings
- Vitamin D, PTH, and Magnesium Synergy
- Insulin Sensitivity and Type 2 Diabetes Risk
- Blood Pressure and the DASH Pattern
- Muscle Cramps, Migraine, and Other Magnesium-Responsive Conditions
- Bioavailability of Almond Magnesium
- Practical Protocol
- Key Research Papers
- Connections
- Featured Videos
The US Magnesium Gap
The Institute of Medicine RDA for magnesium is 420 mg/day for adult men and 320 mg/day for adult women. NHANES survey data, which serially measures dietary intake in a representative US sample, consistently show median magnesium intake of approximately 240-270 mg/day in adults over 19 years of age. Approximately 50-60% of adults in the US consume less than the Estimated Average Requirement (EAR, which is set at the level meeting the needs of half the population). The gap is most pronounced in adults over 70 (lowest intake), in non-Hispanic Black adults, and in those with the lowest household income.
The mechanism behind the gap is straightforward: the foods richest in magnesium — whole grains, dark leafy greens (spinach, chard, kale), legumes (beans, lentils), nuts and seeds, dark chocolate — are systematically displaced in the modern Western diet by refined-grain products, processed snacks, and animal-protein-heavy meals. Magnesium is concentrated in the bran and germ fractions of grains, which are removed in milling to produce refined flour, white rice, and most breakfast cereals. A serving of white bread provides 6-10 mg of magnesium; a comparable serving of whole-wheat bread provides 25-35 mg.
Clinical magnesium deficiency in the formal sense (serum magnesium < 1.7 mg/dL) is rare in the absence of underlying disease or medication effect. Subclinical magnesium insufficiency, however, is widespread — the serum compartment is tightly regulated and remains normal even when bone and muscle magnesium stores are depleted. The downstream consequences of chronic subclinical insufficiency are difficult to measure individually but accumulate over decades.
Almonds as a Magnesium Source
One ounce of raw almonds (approximately 23 nuts) contains 76 mg of magnesium per USDA FoodData Central. Per-ounce comparison with other tree nuts:
- Brazil nuts: 107 mg (highest among tree nuts; selenium toxicity limits intake)
- Cashews: 83 mg
- Almonds: 76 mg
- Pine nuts: 71 mg
- Pecans: 34 mg
- Walnuts: 45 mg
- Pistachios: 34 mg
- Macadamia: 37 mg
Almonds occupy a sweet spot: high enough magnesium density to meaningfully address the gap, without the selenium-toxicity concerns of Brazil nuts (which can deliver 700-1000 mcg of selenium per ounce against a tolerable upper intake of 400 mcg/day). A two-ounce daily almond intake provides 152 mg of magnesium — approximately 36-48% of the RDA from a single snack-format whole food.
Compared with non-nut sources: 1 cup cooked spinach provides 157 mg, 1 cup boiled black beans provides 120 mg, 1 oz pumpkin seeds provides 156 mg, 1 oz dark chocolate (70-85% cocoa) provides 65 mg. Almonds compete well in the snack-format category specifically — you can carry an ounce in a pocket, none of the cooking, preparation, or refrigeration constraints of the other top sources.
Magnesium's Role in Bone Matrix Formation
Bone is roughly 50-60% mineral (predominantly hydroxyapatite, a calcium-phosphate-hydroxyl crystal) and 40-50% organic matrix (predominantly type I collagen, with smaller amounts of non-collagenous proteins). Approximately 60% of total body magnesium — roughly 14-16 grams in a 70 kg adult — is stored in bone, in two distinct compartments.
The first compartment is a stoichiometric magnesium content within the hydroxyapatite crystal itself, substituting for calcium in approximately 0.5-1% of crystal positions. This magnesium content is metabolically inert — it is not exchangeable with serum magnesium and serves a purely structural role. The second compartment is a surface-bound magnesium pool on the crystal surface and within the organic matrix, which is exchangeable with serum and provides the buffering reserve that maintains tight serum magnesium homeostasis.
The functional consequence is that magnesium deficiency impairs bone in three ways. First, the structural magnesium within hydroxyapatite affects crystal size and morphology; magnesium-poor crystals are larger, more brittle, and have less surface area for remodeling. Second, magnesium is a cofactor for alkaline phosphatase activity (the enzyme that hydrolyzes pyrophosphate to allow mineralization to proceed) and for osteoblast proliferation and differentiation. Third, magnesium is required for activation of vitamin D (see next section), and severe magnesium deficiency produces clinical vitamin D resistance that is unresponsive to supplementation.
Animal studies of induced magnesium deficiency consistently show reduced bone mineral density, reduced bone strength, and impaired fracture healing. Human supplementation trials, while smaller and more heterogeneous, show modest improvement in bone density and bone turnover markers in magnesium-deficient subjects.
Framingham Osteoporosis Study Findings
The Framingham Osteoporosis Study (Tucker et al. 1999, AJCN) examined the relationship between dietary magnesium intake and bone mineral density in 907 elderly participants of the Framingham Heart Study cohort. Magnesium intake was assessed by a 126-item food frequency questionnaire; bone mineral density was measured by DXA at the hip and spine.
Key findings: dietary magnesium intake was positively associated with bone mineral density at the hip in both men and women, after adjustment for age, body mass index, caffeine intake, calcium intake, vitamin D intake, smoking status, alcohol intake, physical activity, and hormone replacement therapy use. The magnitude of the effect was approximately 1% higher hip BMD per quintile increase in magnesium intake. Across the full range from lowest to highest quintile of intake, this corresponded to approximately 4% difference in hip BMD — clinically meaningful given that each 1 SD reduction in hip BMD is associated with approximately 2.6-fold increased fracture risk.
Subsequent analyses of other large cohorts (Women's Health Initiative, Korean Health Examinees Study, Norwegian HUNT Study) have largely replicated the magnesium-BMD association, with effect sizes in the same range. The Korean cohort additionally showed that magnesium intake was inversely associated with subsequent hip fracture incidence over 10 years of follow-up.
Interventional data are sparser. A small trial in postmenopausal women with osteoporosis (Stendig-Lindberg et al. 1993) administered 250-750 mg/day of magnesium oxide for 2 years and found approximately 1-3% improvement in trabecular bone density. The Aydin et al. 2010 trial in young adolescents found magnesium supplementation increased hip bone mineral content.
The cumulative interpretation: magnesium adequacy is necessary but not sufficient for optimal bone density. Calcium and vitamin D remain the primary nutritional levers, but a daily ounce of almonds (or equivalent magnesium source) is a reasonable contribution to a comprehensive bone-health dietary pattern for adults at risk for osteoporosis.
Vitamin D, PTH, and Magnesium Synergy
Magnesium is an obligate cofactor at three steps in the vitamin D activation pathway. First, the hepatic 25-hydroxylase enzyme (CYP2R1 and CYP27A1) that converts vitamin D3 to 25-hydroxyvitamin D requires magnesium as a cofactor. Second, the renal 1-alpha-hydroxylase enzyme (CYP27B1) that converts 25-hydroxyvitamin D to the active 1,25-dihydroxyvitamin D requires magnesium. Third, the vitamin D binding protein (DBP) that transports both forms in serum requires magnesium-dependent binding kinetics.
The clinical consequence is that severe magnesium deficiency produces clinical vitamin D resistance. The Uwitonze and Razzaque 2018 review (JAOA) describes the phenotype: low 25-hydroxyvitamin D that fails to rise with oral vitamin D supplementation, accompanied by low 1,25-dihydroxyvitamin D, and persistent hypocalcemia. Restoration of magnesium status, even without additional vitamin D, restores responsiveness to supplementation and normalizes calcium homeostasis.
Parathyroid hormone (PTH) signaling also depends on magnesium. The PTH receptor in target tissues uses magnesium-dependent G-protein signaling. Severely magnesium-deficient patients can paradoxically have low PTH (functional hypoparathyroidism) despite hypocalcemia, because the parathyroid gland cannot mount a normal secretory response without adequate intracellular magnesium.
The practical translation: for patients pursuing vitamin D repletion (the standard recommendation for the majority of adults in northern latitudes with low sun exposure), magnesium adequacy is a prerequisite for the vitamin D to translate into clinical benefit. A daily ounce of almonds, providing 76 mg of magnesium alongside other vitamin D / bone-supporting nutrients, supports this synergy. For the related Vitamin D3 story see the linked page.
Insulin Sensitivity and Type 2 Diabetes Risk
Magnesium plays a direct role in insulin signaling. The insulin receptor is a tyrosine kinase that requires magnesium as a cofactor for its phosphorylation activity, both for autophosphorylation upon insulin binding and for downstream substrate phosphorylation. Magnesium deficiency reduces insulin receptor sensitivity at the cellular level.
Multiple large prospective cohort studies have demonstrated an inverse relationship between dietary magnesium intake and incident type 2 diabetes. The pooled meta-analysis by Larsson and Wolk (2007, J Intern Med), incorporating 7 cohorts and 286,000 participants, found a 15% lower risk of type 2 diabetes per 100 mg/day increment in magnesium intake. The PREDIMED Mediterranean diet trial specifically showed reduced incidence of type 2 diabetes in the nut-supplemented arm, with magnesium intake as one of the mediating mechanisms.
Randomized trials of magnesium supplementation in adults with type 2 diabetes have produced modest improvements in fasting glucose, HOMA-IR, and HbA1c, with the largest effects in subjects with documented baseline magnesium deficiency. The 2011 meta-analysis by Song et al. (Diabetic Medicine) found a pooled HbA1c reduction of 0.4% with magnesium supplementation versus placebo in type 2 diabetic patients.
For adults with type 2 diabetes or insulin resistance, daily almond consumption (alongside the broader Mediterranean dietary pattern) is one of the recommended dietary modifications — combining magnesium adequacy with the low glycemic index and the postprandial-glucose-flattening effect of mixed nuts.
Blood Pressure and the DASH Pattern
The DASH (Dietary Approaches to Stop Hypertension) trial framework demonstrated that a dietary pattern rich in fruits, vegetables, low-fat dairy, whole grains, and nuts/seeds reduces blood pressure comparably to first-line single-drug antihypertensive therapy — roughly 11/6 mmHg reduction at the highest level of adherence. Magnesium intake is one of the major mediating nutrients alongside potassium, calcium, and the dietary fiber load.
The Kass et al. 2012 meta-analysis (European Journal of Clinical Nutrition), pooling 22 randomized trials of magnesium supplementation, found a pooled blood pressure reduction of 2-3 mmHg systolic and 1-2 mmHg diastolic with magnesium supplementation alone, with the largest effects in patients with documented hypertension and chronic disease. Doses in the trial range of 240-960 mg/day were used; the effect appears dose-responsive up to approximately 600 mg/day total intake.
Magnesium reduces blood pressure through multiple mechanisms: vasodilation via calcium-channel-blocking action at vascular smooth muscle, increased nitric oxide production by endothelium, reduced systemic vascular resistance, and indirect effects through reduced sympathetic nervous system activity. The blood pressure effect of a single ounce of almonds alone is small (the 76 mg of magnesium is a modest fraction of the dose typically used in supplementation trials), but added to the broader DASH dietary pattern, it contributes to the overall effect.
Muscle Cramps, Migraine, and Other Magnesium-Responsive Conditions
- Nocturnal leg cramps: Marginal trial evidence (Cochrane review found inconsistent results). A daily ounce of almonds combined with adequate hydration is a reasonable first step before progressing to magnesium supplementation. Patients reporting clear benefit are likely those with subclinical magnesium insufficiency at baseline.
- Migraine prophylaxis: Better trial evidence supports magnesium supplementation (400-600 mg/day) for migraine frequency reduction. The American Headache Society includes magnesium as a Level B recommendation for migraine prophylaxis. Almonds alone do not deliver the trial-tested dose, but contribute to overall magnesium status.
- Premenstrual syndrome (PMS): Some evidence for magnesium supplementation (200 mg/day) reducing PMS-related fluid retention and mood symptoms.
- Constipation: Magnesium oxide and magnesium citrate are osmotic laxatives. Dietary magnesium from food sources does not produce the laxative effect (food-source magnesium is absorbed efficiently in the small intestine; the laxative effect requires the unabsorbed magnesium reaching the colon).
- Restless legs syndrome: Mixed evidence. Some patients report symptomatic improvement with magnesium supplementation; others do not.
- Insulin resistance and metabolic syndrome: Documented benefit in supplementation trials, as discussed above.
- Tinnitus and sensorineural hearing protection: Limited but suggestive evidence for magnesium in noise-induced hearing loss prevention.
Bioavailability of Almond Magnesium
Magnesium in almonds is bound to phytic acid (see the Soaking and Phytic Acid deep-dive page for details), which moderately reduces absorption efficiency compared with magnesium in a simple aqueous salt solution. Estimated bioavailability of magnesium from whole almonds is approximately 30-40%, comparable to magnesium from whole grains and legumes, lower than magnesium from dark leafy greens (60-70%) and from inorganic supplements (35-50% for magnesium oxide, 65-80% for magnesium citrate and glycinate).
Practical implication: of the 76 mg of magnesium in an ounce of almonds, approximately 22-30 mg is actually absorbed and contributes to systemic magnesium status. This is meaningful but modest. Patients with documented magnesium deficiency or with conditions warranting therapeutic magnesium dosing (severe migraine, refractory hypertension, type 2 diabetes with poor glycemic control) should not rely on dietary almonds alone; a supplementation strategy using bioavailable forms (magnesium glycinate, magnesium citrate, magnesium L-threonate) at 200-400 mg/day is appropriate.
Soaking or sprouting almonds (which reduces phytate by 10-30% and 50-70% respectively) modestly improves magnesium bioavailability but at the cost of significant kitchen labor. For most adults pursuing general magnesium adequacy, simply eating a daily ounce of whole almonds (with skin) without additional preparation is sufficient.
Practical Protocol
- Daily dose: 28-56 g (1-2 oz) of whole almonds provides 76-152 mg of magnesium, ~30-50% of which is absorbed (22-76 mg net contribution to status).
- Combine with other magnesium sources: Almonds alone will not close the gap from 240 mg baseline intake to the 320-420 mg/day RDA. Pair with leafy greens, beans, whole grains, pumpkin seeds, or dark chocolate.
- Calcium-magnesium balance: The optimal Ca:Mg ratio in the total diet is approximately 2:1 to 3:1. Modern US diets often have ratios >4:1 (excess calcium from fortified foods, inadequate magnesium). Almonds plus dairy or fortified plant milks helps balance the ratio.
- Bone-health stack: Almonds (magnesium) + dairy or leafy greens (calcium) + sun exposure or D3 supplementation (vitamin D) + adequate protein + resistance exercise. No single intervention is sufficient; the stack is.
- Patients on PPI therapy: Proton pump inhibitors (omeprazole, esomeprazole, etc.) reduce magnesium absorption with chronic use. Long-term PPI patients should specifically prioritize magnesium-dense foods including almonds.
- Patients on diuretics: Loop diuretics (furosemide) and thiazide diuretics increase urinary magnesium losses. Compensatory dietary magnesium increase is warranted.
- Renal disease caution: Advanced chronic kidney disease (eGFR <30) impairs magnesium excretion. Patients in this category should not aggressively load magnesium and should not take magnesium supplements without nephrology guidance.
- Lab assessment: Serum magnesium is a poor marker of body magnesium status (tightly homeostatically regulated). RBC magnesium or 24-hour urinary magnesium are more sensitive indicators if clinical concern warrants assessment.
Key Research Papers
- Tucker KL et al. (1999). Potassium, magnesium, and fruit and vegetable intakes are associated with greater bone mineral density in elderly men and women. American Journal of Clinical Nutrition. — PubMed
- Rude RK, Singer FR, Gruber HE (2009). Skeletal and hormonal effects of magnesium deficiency. Journal of the American College of Nutrition. — PubMed
- Uwitonze AM, Razzaque MS (2018). Role of magnesium in vitamin D activation and function. Journal of the American Osteopathic Association. — PubMed
- Larsson SC, Wolk A (2007). Magnesium intake and risk of type 2 diabetes: a meta-analysis. Journal of Internal Medicine. — PubMed
- Kass L, Weekes J, Carpenter L (2012). Effect of magnesium supplementation on blood pressure: a meta-analysis. European Journal of Clinical Nutrition. — PubMed
- Song Y et al. (2011). Magnesium supplementation in type 2 diabetes meta-analysis. Diabetic Medicine. — PubMed
- Stendig-Lindberg G, Tepper R, Leichter I (1993). Trabecular bone density in a two year controlled trial of peroral magnesium in osteoporosis. Magnesium Research. — PubMed
- Veronese N et al. (2017). Magnesium intake and incident type 2 diabetes meta-analysis. European Journal of Nutrition. — PubMed
- Dimai HP et al. (1998). Daily oral magnesium supplementation suppresses bone turnover in young adult males. Journal of Clinical Endocrinology and Metabolism. — PubMed
- Rodriguez-Moran M, Guerrero-Romero F (2003). Oral magnesium supplementation improves insulin sensitivity and metabolic control in type 2 diabetic subjects: a randomized double-blind controlled trial. Diabetes Care. — PubMed
- Welch AA et al. (2017). Dietary magnesium is positively associated with skeletal muscle power and indices of muscle mass and may attenuate the association between circulating C-reactive protein and muscle mass in women. Journal of Bone and Mineral Research. — PubMed
- Volpe SL (2013). Magnesium in disease prevention and overall health. Advances in Nutrition. — PubMed
PubMed Topic Searches
- PubMed: Magnesium and bone mineral density
- PubMed: Magnesium and type 2 diabetes cohorts
- PubMed: Magnesium and blood pressure
- PubMed: Magnesium and vitamin D activation
- PubMed: Magnesium and migraine prophylaxis
Connections
- Almonds Overview
- Almonds Benefits Hub
- Almonds for Heart Health & LDL
- Almonds for Vitamin E & Skin
- Soaking & Phytic Acid
- Magnesium (Main Page)
- Calcium
- Vitamin D3 (Activation Cofactor)
- Vitamin K2
- Osteoporosis
- Type 2 Diabetes
- Hypertension
- Migraine
- Spinach (Magnesium)
- All Food