Autism Spectrum Disorder (ASD)
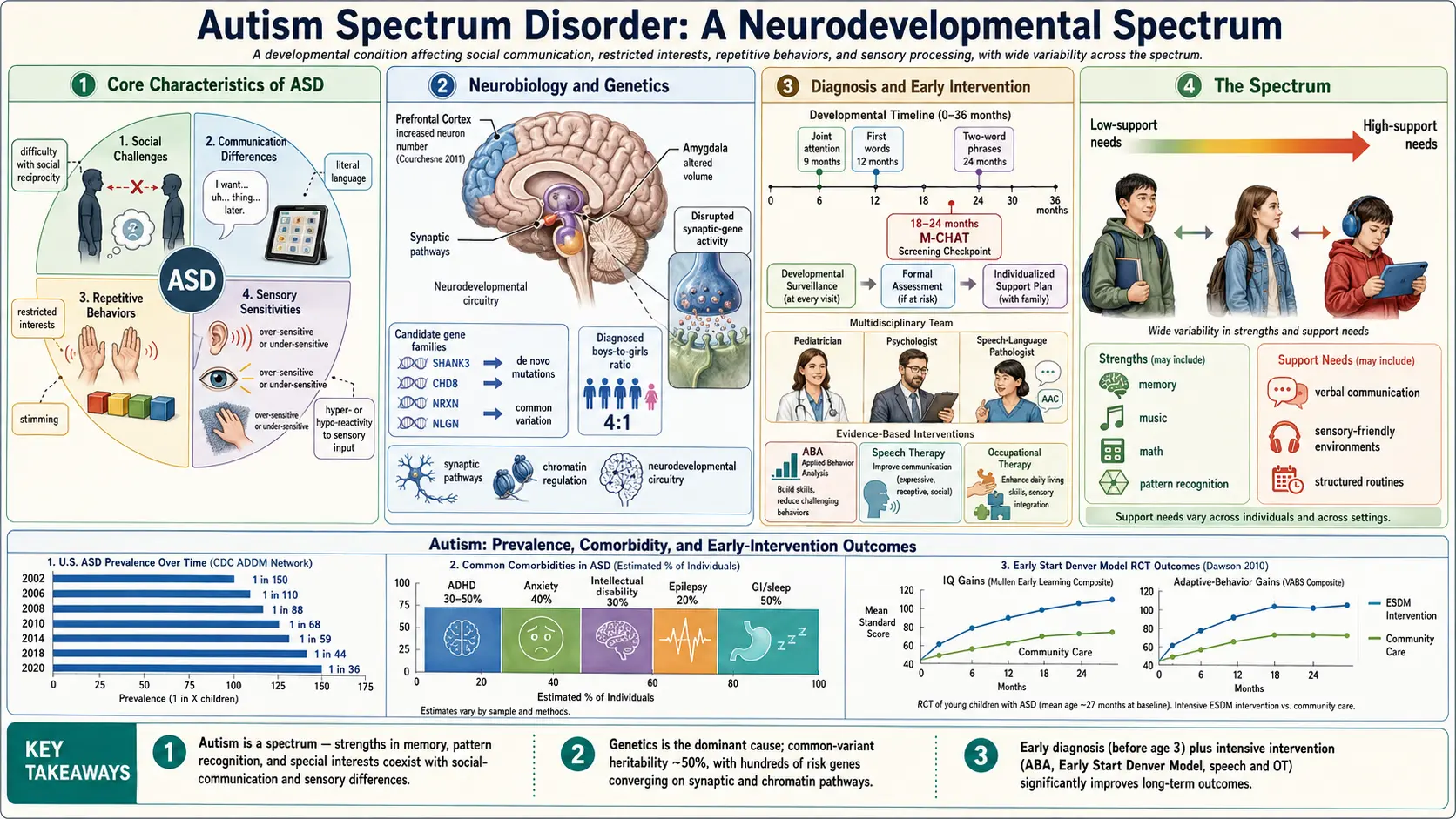
Table of Contents
- Overview
- Epidemiology
- Pathophysiology (Neurobiology)
- Etiology and Risk Factors
- DSM-5 Diagnostic Criteria and Levels
- Clinical Presentation
- Diagnosis and Screening
- Treatment and Interventions
- Comorbidities
- Complications and Quality of Life
- Prognosis and Adult Outcomes
- Research Papers and References
- Featured Videos
1. Overview
Autism Spectrum Disorder (ASD) is a neurodevelopmental condition characterized by persistent differences in social communication and interaction, combined with restricted, repetitive patterns of behavior, interests, or activities. The DSM-5 (2013) collapsed what were previously separate diagnoses — Autistic Disorder, Asperger Syndrome, and Pervasive Developmental Disorder Not Otherwise Specified (PDD-NOS) — into a single unified spectrum, reflecting the continuous and heterogeneous nature of these presentations.
ASD is not a disease to be cured but a neurodevelopmental condition representing a different profile of cognitive and social processing. The CDC's 2023 estimate places prevalence at 1 in 36 children in the United States — up from 1 in 150 in 2000 — a change that primarily reflects expanded diagnostic criteria, greater awareness, and improved access to evaluation rather than a true epidemic. Males are diagnosed approximately 4 times more often than females, though the true ratio is closer to 3:1; females tend to present differently and engage in "camouflaging" or "masking," leading to delayed or missed diagnoses.
ASD is defined by two core domains in the DSM-5:
- Persistent deficits in social communication and social interaction across multiple contexts
- Restricted, repetitive patterns of behavior, interests, or activities
The heterogeneity of ASD is profound. As the saying in the autism community goes: "If you've met one person with autism, you've met one person with autism." Presentations range from individuals requiring round-the-clock support who are nonspeaking, to highly articulate adults who hold advanced degrees and careers but struggle with social reciprocity and sensory processing. Understanding this spectrum is essential to providing appropriate, individualized support.
2. Epidemiology
The CDC's Autism and Developmental Disabilities Monitoring (ADDM) Network reported a prevalence of 1 in 36 children aged 8 years in the United States in 2020, published in 2023 (PMID: 36897920). Global estimates generally range from 1–2% of the population, with variation reflecting differences in diagnostic criteria, case ascertainment methods, and healthcare access rather than true geographic differences in underlying biology.
Prevalence has risen dramatically over recent decades — from approximately 1 in 150 in 2000 to 1 in 36 in 2023. This increase is primarily explained by:
- Expanded diagnostic criteria — particularly the broadening associated with DSM-IV (1994) to include Asperger Syndrome and PDD-NOS
- Diagnostic substitution — intellectual disability (ID) diagnoses have declined as ASD diagnoses rose; many individuals previously labeled ID now receive ASD diagnoses
- Increased awareness among clinicians, parents, teachers, and the public
- Reduction of stigma encouraging more families to seek evaluation
Important demographic patterns:
- Sex ratio: Males are diagnosed 4 times more often than females (diagnosed ratio), but the true biological ratio is closer to 3:1. Females show stronger social motivation, better mimicry of social norms, and more socially acceptable special interests — a phenomenon called camouflaging or masking — which delays recognition and diagnosis by an average of 2-3 years compared to white males.
- Race and ethnicity: Black and Hispanic children are historically underdiagnosed due to access barriers, clinician bias, and language barriers in standardized assessments. Recent ADDM data show narrowing but persistent disparities.
- Adult prevalence: Estimated 1–2% of adults, with a large proportion of individuals over age 40 undiagnosed — many received diagnoses of intellectual disability, schizophrenia, or personality disorders before ASD was well recognized in adults.
- Former Asperger Syndrome (now ASD Level 1) had a diagnosed male-to-female ratio as high as 9:1 in some studies, but female underdiagnosis is particularly pronounced in this group.
3. Pathophysiology (Neurobiology)
Synaptic Development and Pruning
One of the most replicated neurobiological findings in ASD is altered synaptic pruning — the normal developmental process by which excess synaptic connections are eliminated during childhood and adolescence to improve neural efficiency. In autism, this pruning is reduced, leading to an excess of synaptic connections (synaptic density) particularly in the cortex. Postmortem studies have confirmed increased synapse density in the prefrontal cortex of autistic individuals compared to neurotypical controls.
Excitatory/Inhibitory (E/I) Imbalance
The E/I imbalance theory, developed by Rubenstein and Merzenich (2003), proposes that ASD results from an elevated ratio of excitatory (glutamatergic) to inhibitory (GABAergic) signaling in key neural systems. Evidence includes elevated glutamate and reduced GABA concentrations in specific brain regions detected by magnetic resonance spectroscopy, and convergent genetic findings implicating genes that regulate E/I balance (SHANK3, NRXN1, CNTN4). This imbalance may contribute to sensory hypersensitivity, repetitive behaviors, and epilepsy comorbidity.
Brain Connectivity and Default Mode Network
Functional MRI studies consistently demonstrate altered long-range connectivity in ASD. The default mode network (DMN) — a system active during social cognition, self-referential thought, and mentalizing — shows hypoconnectivity in autism, particularly between medial prefrontal cortex and posterior cingulate cortex. Short-range local connectivity may be increased while long-range connectivity is decreased — a pattern sometimes called "under-connectivity theory." The mirror neuron system has also been implicated in social-cognitive differences, though this remains debated.
Amygdala and Social Processing
The amygdala, critical for processing emotional salience and social stimuli, shows both structural and functional differences in ASD. Amygdala hyperreactivity to social stimuli (particularly faces and eyes) may drive gaze avoidance as a self-regulating strategy rather than a social deficit per se. Early brain overgrowth — including enlarged amygdala — is observed in toddlers with ASD, followed by normalization or even reduction in later childhood.
Early Brain Overgrowth
Prospective MRI studies of high-risk infant siblings of autistic children demonstrate accelerated brain volume growth during the first 2 years of life in children who later receive ASD diagnoses. This early overgrowth, particularly of cortical surface area, precedes behavioral symptom emergence and is detectable before 12 months. Increased head circumference (macrocephaly) in toddlers is a clinical correlate observed in a subset of autistic individuals.
Cerebellar and Immune Mechanisms
The cerebellum — long considered purely a motor structure — is increasingly recognized for roles in social cognition, language, and sensory prediction. Cerebellar abnormalities are among the most consistent neuropathological findings in postmortem ASD brain studies. Additionally, immune dysregulation is observed in a substantial subset: elevated maternal antibodies against fetal brain proteins, altered microglial activation, and differences in the gut-brain axis microbiome are active areas of investigation, though no single immune mechanism accounts for ASD broadly.
4. Etiology and Risk Factors
Genetic Factors
ASD is among the most heritable of neurodevelopmental conditions. Monozygotic twin concordance rates range from 64–91% in different studies, and heritability is estimated at 64–91% (Tick et al., 2016 meta-analysis). The genetic architecture is highly complex:
- Hundreds of risk genes have been implicated, including CHD8, SHANK3, PTEN, FMR1, NRXN1, and CNTN4 — but no single gene accounts for more than 1–2% of cases
- De novo mutations (spontaneous, not inherited from parents) account for approximately 30% of ASD cases
- Common variants of small effect contribute to polygenic risk — genome-wide association studies (GWAS) have identified dozens of loci
- Rare copy number variants (CNVs) — chromosomal deletions or duplications — are found in 5–10% of ASD cases
Monogenic and Chromosomal Syndromes
- Fragile X syndrome (FMR1 gene mutation) — the most common single-gene cause of ASD; 20–50% of males with Fragile X also meet ASD criteria
- Rett syndrome (MECP2 mutation) — predominantly affects females; characterized by regression after 6–18 months of apparently normal development
- Tuberous sclerosis complex (TSC1/TSC2) — 25–50% have ASD
- 22q11.2 deletion syndrome (velocardiofacial syndrome) — 15–20% have ASD
- CHARGE syndrome, Angelman syndrome, Phelan-McDermid syndrome (22q13.3) — all associated with high ASD rates
- PTEN hamartoma tumor syndrome — macrocephaly plus ASD presentation
Prenatal and Perinatal Risk Factors
- Advanced parental age — particularly paternal age; de novo mutation rate increases with paternal age. Risk increases ~5% per additional 5 years of paternal age
- Maternal infection during pregnancy — rubella (causing congenital rubella syndrome), cytomegalovirus, and maternal immune activation (animal models strongly support this pathway)
- Valproate in pregnancy — anticonvulsant valproic acid carries a 3-fold increased risk of ASD; now carries FDA black box warning regarding neural tube defects and neurodevelopmental risks
- Thalidomide exposure in pregnancy (historical) — provided early evidence of prenatal vulnerability window
- Extreme prematurity (<28 weeks gestation) — 7–8% rate of ASD diagnosis
- Maternal diabetes and obesity — modest association in epidemiological studies
What Does NOT Cause Autism
Vaccines do not cause autism. The 1998 Wakefield paper in The Lancet that claimed a link between the MMR (measles-mumps-rubella) vaccine and autism was found to be fraudulent — data were fabricated, ethical violations were committed, and the paper was fully retracted in 2010. Wakefield's medical license was revoked by the UK General Medical Council. Subsequent large-scale studies have definitively refuted any connection — most notably the Danish cohort study of 650,000 children (Madsen et al., 2002) and a 2019 Danish study of 650,000 children born 1999–2010 finding no increased risk. The autism-vaccine claim has caused measurable harm through declining vaccination rates and resurgent preventable disease outbreaks.
Autism is also not caused by "refrigerator mothers" (Bettelheim's discredited 1967 theory of cold, rejecting parenting), gut bacteria alone, screen time exposure, or single environmental toxins in isolation.
5. DSM-5 Diagnostic Criteria and Levels
Domain A — Social Communication and Interaction
Persistent deficits in social communication and social interaction across multiple contexts, as manifested by all three of the following:
- A1: Deficits in social-emotional reciprocity — abnormal social approach, failure of normal back-and-forth conversation, reduced sharing of interests or emotions, failure to initiate or respond to social interactions
- A2: Deficits in nonverbal communicative behaviors used for social interaction — poorly integrated verbal and nonverbal communication, abnormalities in eye contact and body language, deficits in understanding and use of gestures, absent facial expressions and nonverbal communication
- A3: Deficits in developing, maintaining, and understanding relationships — difficulties adjusting behavior to suit different social contexts, difficulties in sharing imaginative play or in making friends, absence of interest in peers
Domain B — Restricted, Repetitive Behaviors
Restricted, repetitive patterns of behavior, interests, or activities, as manifested by at least two of the following four:
- B1: Stereotyped or repetitive motor movements, use of objects, or speech (simple motor stereotypies, lining up toys, echolalia, idiosyncratic phrases)
- B2: Insistence on sameness, inflexible adherence to routines, or ritualized patterns of verbal or nonverbal behavior (extreme distress at small changes, difficulties with transitions, rigid thinking patterns, greeting rituals, same route or food daily)
- B3: Highly restricted, fixated interests that are abnormal in intensity or focus (strong attachment to or preoccupation with unusual objects, perseverative interest)
- B4: Hyper- or hyporeactivity to sensory input or unusual interest in sensory aspects of the environment (apparent indifference to pain/temperature, adverse responses to specific sounds or textures, excessive smelling or touching of objects, visual fascination with lights or movement)
Additional Requirements
- Symptoms must be present in the early developmental period (though they may not fully manifest until social demands exceed limited capacities, or may be masked by learned strategies later in life)
- Symptoms cause clinically significant impairment in social, occupational, or other important areas of functioning
- Not better explained by intellectual disability alone or global developmental delay (though ASD and ID frequently co-occur)
DSM-5 Severity Levels
- Level 1 — "Requiring Support" (formerly Asperger Syndrome / High-Functioning Autism): Without supports in place, deficits in social communication cause noticeable impairments. Inflexibility of behavior causes significant interference in one or more contexts. Difficulty switching between activities.
- Level 2 — "Requiring Substantial Support": Marked deficits in verbal and nonverbal social communication skills; social impairments apparent even with supports in place. Inflexibility and distress with change is obvious to casual observers.
- Level 3 — "Requiring Very Substantial Support": Severe deficits in verbal and nonverbal social communication cause severe functional impairments. Very limited initiation of social interactions. Extreme difficulty coping with change.
Note: Severity levels may vary across the two domains and can change over time. Many autistic self-advocates note that "Level 1" (formerly "high-functioning") does not mean low support needs — it means the autistic person's struggles are less visible to others.
6. Clinical Presentation
Early Signs and Red Flags
Developmental red flags that should prompt immediate ASD evaluation include:
- No babbling by 12 months
- No pointing or other gestures (joint attention) by 12 months
- No single words by 16 months
- No two-word spontaneous phrases by 24 months (echolalia does not count)
- Any loss of language or social skills at any age (developmental regression)
- Inconsistent social smile, reduced or atypical eye contact, unusual sensory responses in infancy
Toddler and School-Age Presentation
- Echolalia — immediate (repeating what was just said) or delayed (repeating scripts from TV, books, or past conversations)
- Pronoun reversal — saying "you want water" instead of "I want water"
- Special interests — intense, encyclopedic knowledge of a specific topic (trains, dinosaurs, video game lore, maps, weather patterns)
- Rigid routines — significant distress when routines are disrupted (different route to school, food on wrong plate, unexpected schedule change)
- Meltdowns — neurological responses to overwhelm that differ from willful tantrums; the child cannot "calm down on demand"
- Stimming (self-stimulatory behavior) — hand-flapping, rocking, spinning, finger-flicking; serves a sensory regulation function and is not inherently harmful
Female Presentation and Masking
Autistic females, on average, show different presentations that lead to systematic underdiagnosis:
- Better social mimicry — studying and copying neurotypical social scripts consciously
- Stronger motivation to form social connections — even when it is effortful and exhausting
- More socially accepted special interests — animals, celebrities, reading, horses (vs. trains or mathematics, which trigger clinician recognition more readily)
- Camouflaging/masking — the conscious or unconscious suppression of autistic traits to fit in; associated with significantly higher rates of anxiety, depression, burnout, and suicidality in adulthood
- Later diagnosis — autistic females are diagnosed on average 2–4 years later than males
Sensory Processing Differences
Sensory differences (DSM-5 B4) are among the most impactful and underrecognized features of ASD:
- Auditory — hypersensitivity to certain sounds (vacuum cleaners, sirens, certain voices), or hyposensitivity with apparent hearing loss
- Tactile — intolerance of clothing tags, seams, certain fabrics, or unexpected touch
- Taste/smell — extreme food selectivity driven by texture, color, smell, or temperature (ARFID is highly comorbid)
- Pain — hyposensitivity to pain in some individuals, creating safety risks from unrecognized injuries
- Proprioception/interoception — difficulty sensing body position, hunger, thirst, or bladder fullness
Gastrointestinal Symptoms
GI problems occur in 40–70% of autistic individuals — far above the general population rate. Constipation, diarrhea, abdominal pain, and GERD are most common. The gut-brain axis and GI discomfort may contribute to behavioral presentations; a nonverbal autistic person in pain may present as aggressive or self-injurious. GI symptoms should always be evaluated before attributing behavioral changes solely to ASD.
7. Diagnosis and Screening
Universal Screening
The American Academy of Pediatrics (AAP) recommends universal ASD screening at the 18-month and 24-month well-child visits using the Modified Checklist for Autism in Toddlers, Revised with Follow-Up (M-CHAT-R/F). A positive screen should trigger referral for comprehensive diagnostic evaluation without waiting to see if the child "grows out of it" — early identification is the most modifiable factor in long-term outcomes.
Comprehensive Diagnostic Evaluation
ASD diagnosis requires a multidisciplinary evaluation including:
- ADOS-2 (Autism Diagnostic Observation Schedule, 2nd Edition) — the gold standard observational assessment; a structured play or conversation session that elicits social communication behaviors for scoring across five modules by developmental/language level
- ADI-R (Autism Diagnostic Interview-Revised) — semi-structured caregiver interview covering developmental history across social, communication, and behavioral domains
- Cognitive testing (WISC-V for school-age children, WPPSI for younger) — to characterize intellectual profile and identify co-occurring intellectual disability
- Speech-language evaluation — comprehensive language assessment including pragmatic language skills
- Occupational therapy assessment — sensory processing profile, fine motor skills, activities of daily living
Medical Workup
- Chromosomal microarray (CMA) — first-line genetic test; identifies etiology in 10–20% of ASD cases
- FMR1 testing — to rule out Fragile X syndrome
- MECP2 sequencing — for females with regression, especially if Rett syndrome features are present
- Audiological evaluation — to rule out hearing loss as a contributing factor before ASD diagnosis is finalized
- Electroencephalogram (EEG) — if seizures are suspected
- There is no diagnostic blood test, biomarker, or brain scan for ASD; diagnosis remains clinical
Diagnostic Delays
The average age of ASD diagnosis in the United States is approximately 4–5 years, with many children not diagnosed until school age or later. Disparities are significant: Black children are diagnosed on average 2.5 years later than white children; girls and Asians are diagnosed 2–3 years later than white males. Late diagnosis means years of inadequate support during critical developmental windows.
8. Treatment and Interventions
There are no FDA-approved medications for the core features of ASD (social communication deficits, restricted and repetitive behaviors). Treatment is behavioral and educational, with medications used only for associated symptoms. Early, intensive intervention during the preschool years has the strongest evidence base.
Early Intensive Behavioral Intervention
- Early Intensive Behavioral Intervention (EIBI) — based on Applied Behavior Analysis (ABA) principles; 20–40 hours per week beginning before age 3. The most extensively researched intervention in ASD, with multiple randomized trials showing gains in IQ, language, and adaptive behavior.
- Early Start Denver Model (ESDM) — specifically designed for children ages 12–48 months; integrates ABA principles with developmental and relationship-based approaches; Dawson et al. (2010) RCT showed significant IQ and language gains at 2 years (PMID: 19948568).
- Pivotal Response Training (PRT) — naturalistic ABA targeting pivotal areas (motivation, responsivity to multiple cues) to produce broad behavioral improvements
Communication Therapies
- Speech-language therapy — for language development, pragmatic language skills, and conversation skills
- Augmentative and Alternative Communication (AAC) — for minimally verbal or nonverbal individuals; includes picture exchange (PECS), speech-generating devices (SGDs), and tablet-based systems. AAC does not impede speech development and frequently facilitates it.
- Social skills training — PEERS (Program for the Education and Enrichment of Relational Skills) is a well-validated manualized program for teenagers and young adults
Occupational Therapy
OT addresses sensory processing difficulties, fine motor development, activities of daily living (dressing, feeding, grooming), and handwriting. Sensory integration therapy is widely used though evidence is mixed; sensory diet approaches (scheduled sensory activities) are commonly implemented.
ABA Controversy
Modern ABA, particularly EIBI, has robust evidence for improving functional outcomes. However, controversy exists: older ABA approaches focused heavily on eliminating autistic behaviors (including stimming, which has regulatory functions) and used aversive techniques. Many autistic adults who received intensive ABA report significant trauma. Contemporary best practice focuses on improving quality of life, developing meaningful communication and adaptive skills, and building on the individual's strengths — not on producing neurotypical appearances. Stimming should not be suppressed unless it causes self-injury.
Medications for Associated Symptoms
- Risperidone — FDA-approved (2006) for irritability associated with ASD in children ages 5–16; targets aggression, self-injurious behavior, and severe tantrums
- Aripiprazole — FDA-approved (2009) for irritability associated with ASD in children ages 6–17
- SSRIs (sertraline, fluoxetine) — used for anxiety and repetitive behaviors; evidence is mixed in children, more support in adults
- Stimulants / atomoxetine — for co-occurring ADHD symptoms; response rates slightly lower than in non-autistic ADHD but still meaningful
- Melatonin — widely used for sleep onset difficulties; well-tolerated, effective; most autistic children have altered melatonin secretion profiles
- Anticonvulsants — for comorbid epilepsy (choice of agent should consider behavioral side effects and teratogenicity considerations for females of reproductive age; valproate is avoided)
Adult Supports
- Supported employment — job coaching, workplace accommodations, disclosure planning; significantly improves employment outcomes
- Supported living — for individuals requiring ongoing assistance with daily living; residential supports range from host homes to congregate settings
- Cognitive behavioral therapy (CBT) — adapted for autistic individuals addresses anxiety, depression, and emotion regulation; modifications include more structured/explicit format, visual supports, and focus on practical strategies over insight
- Autistic community and peer support — connection with other autistic adults is increasingly recognized as important for identity, self-acceptance, and mental health
9. Comorbidities
ASD rarely occurs in isolation. The majority of autistic individuals have at least one — often multiple — comorbid conditions:
- Intellectual disability (ID) — approximately 30–40% of autistic individuals have co-occurring ID; conversely, ~70% of those with severe ID have ASD features
- Epilepsy — 20–30% lifetime prevalence of seizures in ASD; seizure onset has a bimodal distribution (early childhood and adolescence). Risk increases with severity of intellectual disability.
- ADHD — 40–70% of autistic individuals also meet ADHD criteria; DSM-5 (2013) removed the prior exclusion that prevented dual diagnosis
- Anxiety disorders — 40–60%; generalized anxiety, social anxiety, and specific phobias are most common. Anxiety may be the primary driver of behavioral difficulties in many autistic individuals.
- OCD — 17–37%; distinguishing ASD restricted/repetitive behaviors from OCD compulsions can be clinically challenging; key distinction is ego-dystonic nature of OCD vs. ego-syntonic in ASD
- Depression — 12–70% in autistic adults; rates increase with age and are particularly elevated in women and those with higher cognitive ability (who are more aware of social differences and experience more masking burden)
- Sleep disorders — 50–80%; sleep-onset insomnia is most common; altered melatonin profiles contribute; sleep difficulties worsen behavioral and cognitive symptoms
- Gastrointestinal problems — 40–70%; constipation, diarrhea, GERD, abdominal pain; may be related to altered gut microbiome, diet restriction, or autonomic nervous system differences
- Tourette syndrome / tic disorders — 11% in some samples; tics and ASD share genetic risk factors
- Avoidant/Restrictive Food Intake Disorder (ARFID) — sensory-based food selectivity; affects a significant proportion of autistic children and can lead to nutritional deficiencies
- Hypermobility / hypermobile Ehlers-Danlos syndrome (hEDS) — emerging evidence of a higher-than-expected co-occurrence, currently under active investigation
- Elopement and safety risks — 49% of autistic children have wandered or eloped from safe settings; drowning is the leading cause of death in autistic children, underscoring critical safety intervention needs
10. Complications and Quality of Life
The challenges faced by autistic individuals extend far beyond core diagnostic features and have profound impacts on health, safety, and well-being across the lifespan:
- Employment — 70–80% of autistic adults are underemployed or unemployed despite many having the cognitive ability to work. Sensory environments, communication demands, and social complexity of workplaces create barriers that accommodations can often address but rarely do without advocacy.
- Education barriers — college completion rates are substantially lower for autistic students; sensory overwhelm, executive function demands, and social complexity of college environments create barriers not addressed by typical disability accommodations
- Social isolation and loneliness — Mazurek (2014) found that autistic adults have significantly fewer friendships and higher loneliness scores than both neurotypical adults and adults with other disabilities (PMID: 23147515)
- Safety — 49% of autistic children have eloped (wandered from safe supervision); drowning accounts for 91% of ASD-related deaths due to wandering. Medical alert bracelets, fencing, swimming lessons, and community first responder training are critical safety interventions.
- Bullying victimization — autistic youth are bullied at rates 3–4 times higher than neurotypical peers; bullying significantly worsens anxiety, depression, and school avoidance
- Suicide — autistic adults have markedly elevated suicidality; Hirvikoski et al. (2016) found 35–66% of autistic adults report suicidal ideation, and suicide is a leading cause of death in autistic adults without intellectual disability (PMID: 26541693)
- Premature mortality — Hirvikoski et al. (2016) demonstrated that autistic adults die on average 16 years earlier than the general population, driven by epilepsy, accidents, drowning, and suicide; medical comorbidities and barriers to healthcare access contribute
- The "high-functioning" paradox — the label "high-functioning" (now Level 1 or formerly Asperger's) is frequently used to deny accommodations and supports. An autistic person who can speak, attend school, and hold conversation may still struggle profoundly with sensory overwhelm, executive function, and social energy demands — and may spend enormous effort masking, contributing to autistic burnout.
- Late diagnosis consequences — women and minorities diagnosed in adulthood often describe decades of misdiagnosis (depression, borderline personality disorder, anxiety, "giftedness") and inadequate support, leading to compounded mental health challenges. A late ASD diagnosis can be both validating and grief-provoking.
- Autistic burnout — a phenomenon described by autistic adults as long-term exhaustion from the effort of masking and coping with a neurotypical world; characterized by loss of skills, reduced capacity to function, and increased mental health crises; not yet an official diagnostic category but increasingly recognized clinically
11. Prognosis and Adult Outcomes
Outcomes across the autism spectrum are highly variable and are influenced by a complex interplay of individual characteristics, early intervention access, and the degree to which environments are adapted to accommodate autistic needs.
Predictors of Better Outcomes
- Higher IQ — consistently the strongest predictor of functional independence in adulthood
- Functional language by age 5 — having phrase speech by school entry is associated with better educational and social outcomes
- Early access to intensive intervention — particularly before age 3
- Absence of severe intellectual disability and epilepsy
- Responsive, adaptable family environment
- Access to appropriate educational and vocational supports
Trajectory Over Time
Approximately 10–20% of children diagnosed with Level 2 or Level 3 ASD show significant improvements that move them to a Level 1 presentation with intensive early intervention. A smaller subset — the "optimal outcomes" group studied by Fein and colleagues — no longer meets ASD diagnostic criteria by early adulthood. However, research shows these individuals continue to show subtle social and cognitive differences compared to typical controls, and many continue to identify as autistic.
Many autistic adults do not achieve full independent living: approximately 50% of autistic adults live with family members; supported living arrangements serve many others. Only a minority achieve fully independent community living without any formal support.
Employment and Community Integration
- Only approximately 16% of autistic adults in the UK are in full-time paid employment (National Autistic Society data)
- US estimates suggest 58% of young autistic adults ages 21–25 have ever held a paying job, compared to 74% of those with other disabilities
- Supported employment programs show significantly better outcomes than segregated day programs or sheltered workshops
- Many autistic adults report finding meaningful work in technology, STEM fields, the arts, and skilled trades — contexts where their specialist interests and systematic thinking styles are assets
The Neurodiversity Perspective
The neurodiversity movement, led by autistic self-advocates, frames autism not primarily as a deficit but as a different neurological configuration — one that brings both challenges and genuine strengths (pattern recognition, attention to detail, systematic thinking, honesty, deep expertise). The goal of intervention, from this perspective, is not to make autistic people appear neurotypical but to reduce suffering, build skills, and create accessible environments. This perspective does not deny that autism involves real challenges — particularly for those with severe support needs — but challenges the framing of autism as a disorder to be eliminated.
12. Research Papers and References
Key Research Papers
- Maenner MJ, et al. Prevalence and Characteristics of Autism Spectrum Disorder Among Children Aged 8 Years — Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2020. MMWR. 2023;72(2):1-14 — Search PubMed. DOI: 10.15585/mmwr.ss7202a1
- Tick B, et al. Heritability of autism spectrum disorders: a meta-analysis of twin studies. J Child Psychol Psychiatry. 2016;57(5):585-595. PMID: 26709141. DOI: 10.1111/jcpp.12499
- Lord C, et al. Autism spectrum disorder. Lancet. 2020;395(10224):562-574 — Search PubMed. DOI: 10.1016/S0140-6736(19)32153-X
- Sandin S, et al. The familial risk of autism. JAMA. 2017;317(17):1770-1777 — Search PubMed. DOI: 10.1001/jama.2017.4144
- Rubenstein JL, Merzenich MM. Model of autism: increased ratio of excitation/inhibition in key neural systems. Genes Brain Behav. 2003;2(5):255-267. PMID: 14606691. DOI: 10.1034/j.1601-183x.2003.00037.x
- Madsen KM, et al. A population-based study of measles, mumps, and rubella vaccination and autism. NEJM. 2002;347(19):1477-1482. PMID: 12421889. DOI: 10.1056/NEJMoa021134
- Dawson G, et al. Randomized, controlled trial of an intervention for toddlers with autism: the Early Start Denver Model. Pediatrics. 2010;125(1):e17-23. PMID: 19948568. DOI: 10.1542/peds.2009-0958
- Aman MG, et al. The effects of risperidone on the behavior problems of children with autism. Am J Psychiatry. 2002;159(8):1337-1346 — Search PubMed. DOI: 10.1176/appi.ajp.159.8.1337
- Hirvikoski T, et al. Premature mortality in autism spectrum disorder. Br J Psychiatry. 2016;208(3):232-238. PMID: 26541693. DOI: 10.1192/bjp.bp.114.159426
- Mazurek MO. Loneliness, friendship, and well-being in adults with autism spectrum disorders. Autism. 2014;18(3):223-232 — Search PubMed. DOI: 10.1177/1362361312474121
- Lovaas OI. Behavioral treatment and normal educational and intellectual functioning in young autistic children. J Consult Clin Psychol. 1987;55(1):3-9. PMID: 3571656. DOI: 10.1037/0022-006x.55.1.3
- Fombonne E, et al. Pervasive developmental disorders in Montreal, Quebec, Canada: prevalence and links with immunizations. Pediatrics. 2006;118(1):e139-150. PMID: 16818529. DOI: 10.1542/peds.2005-2993
PubMed Topic Searches
- PubMed: autism spectrum disorder prevalence epidemiology
- PubMed: autism genetics heritability twin studies
- PubMed: autism early intervention ABA
- PubMed: autism comorbidity ADHD anxiety
- PubMed: autism diagnosis ADOS screening
- PubMed: autism adult outcomes employment
- PubMed: autism vaccines MMR safety
- PubMed: autism female camouflaging masking
Connections
- ADHD
- OCD
- Anxiety
- Depression
- Insomnia
- Eating Disorders
- Tic Disorders
- Tourette Syndrome
- Epilepsy
- Magnesium
- Vitamin B6
- Vitamin D3