Tourette Syndrome
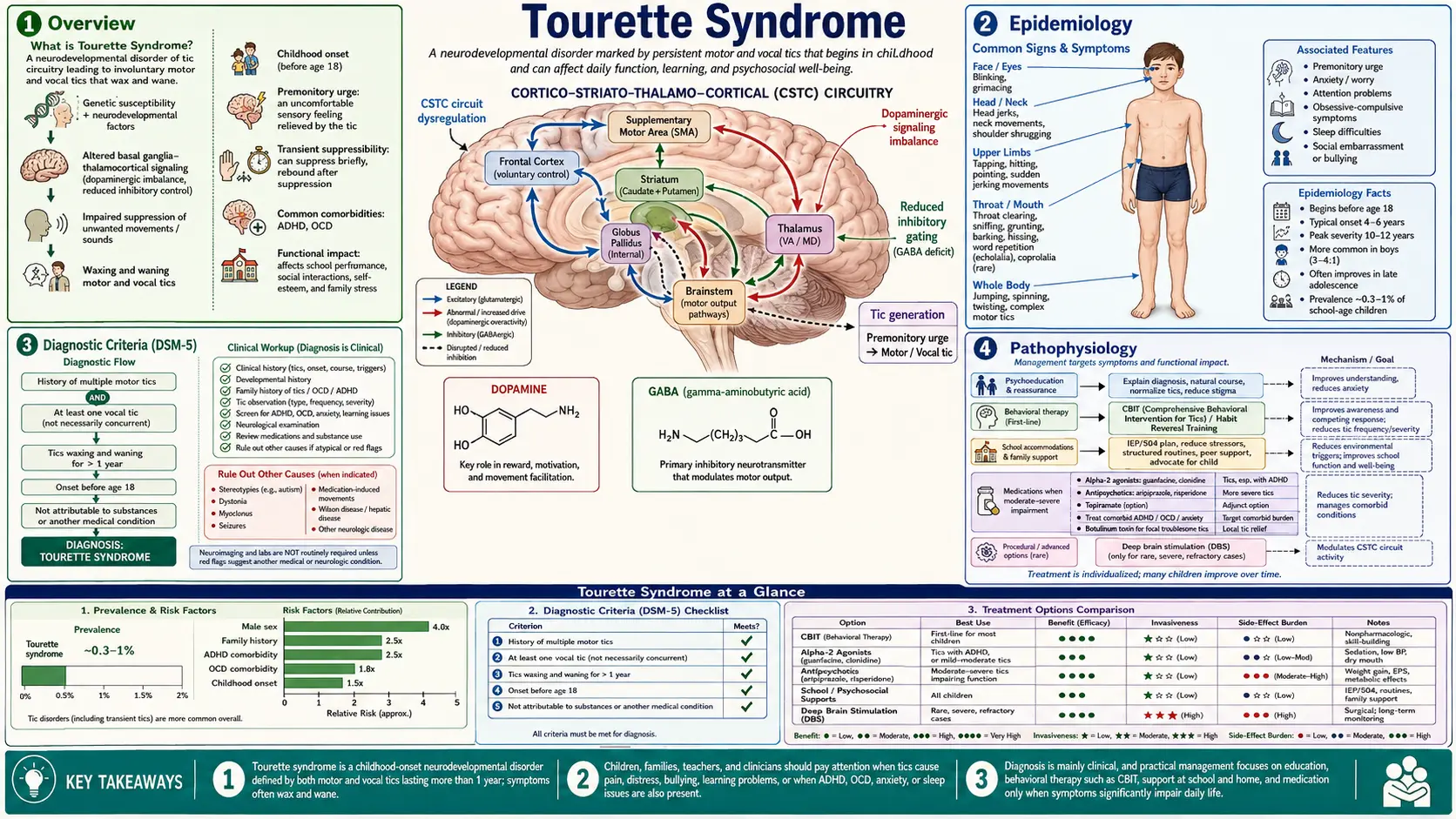
Table of Contents
- Overview
- Epidemiology
- Diagnostic Criteria (DSM-5)
- Pathophysiology
- Clinical Presentation
- Natural History
- Comorbidities
- Diagnosis
- Treatment
- Living with Tourette Syndrome
- Recent Research and Advances
- References & Research
- Research Papers
- Connections
Overview
Tourette syndrome (TS) is a neurodevelopmental disorder characterized by multiple motor tics and at least one vocal (phonic) tic, present for more than one year, with onset before age 18. It is named after French neurologist Gilles de la Tourette, who first formally described the condition in 1885 after observing a group of patients with involuntary movements and vocalizations.
Four critical facts about Tourette syndrome that most people — including newly diagnosed families — are not told upfront:
- TS is far more common than most people think. It affects approximately 1 in 100 school-age children. Many children with mild tics are never formally diagnosed.
- Coprolalia (involuntary swearing) is NOT typical. The popular media image of TS as a condition defined by involuntary obscene language occurs in only 10–15% of cases and is not required for diagnosis. Most people with TS never have coprolalia.
- Most children significantly improve by adulthood. The natural history of TS is favorable — approximately 50–60% of children experience meaningful improvement by late adolescence, and some achieve near-complete remission. The course is typically not lifelong and severely debilitating.
- Comorbidities drive more impairment than tics. ADHD, OCD, and anxiety disorders co-occur in the majority of people with TS, and these associated conditions often cause far greater day-to-day difficulty than the tics themselves. Effective treatment must address the full picture.
TS is classified as a tic disorder, a category that includes milder and briefer forms: provisional tic disorder (formerly called transient tic disorder, lasting less than 1 year) and persistent (chronic) motor or vocal tic disorder (one type of tic only, lasting more than 1 year). Full Tourette syndrome requires both motor and vocal tics for over a year. Most children who develop tics have one of the milder forms, not full TS.
Epidemiology
Tourette syndrome affects approximately 0.3–0.9% of school-age children in most population-based studies, with some estimates approaching 1%. When milder tic disorders are included, the proportion of children who experience some form of tics rises considerably — provisional tic disorder alone may affect up to 20% of children at some point during childhood.
Key epidemiological facts:
- Sex ratio: Males are affected approximately 3–4 times more often than females. The reason for this disparity is not fully understood but likely involves sex-linked differences in dopaminergic and serotonergic neurodevelopment.
- Age of onset: Motor tics typically emerge first, usually between ages 4 and 6. Vocal tics appear somewhat later, often ages 6–8. Peak tic severity occurs around ages 10–12.
- Family history: TS has a strong genetic component. First-degree relatives of individuals with TS have roughly a 15% risk of TS themselves and a higher risk of other tic disorders or OCD. Twin studies show concordance rates of ~50–60% in monozygotic twins and ~10% in dizygotic twins, indicating both genetic and environmental contributions.
- Ethnicity: Some studies report higher prevalence in White and Hispanic children compared to Black children, though this may partly reflect ascertainment bias and differential access to diagnosis.
- Socioeconomic factors: Lower income families may have higher rates of undiagnosed TS due to reduced healthcare access, yet also face greater functional burden from untreated comorbid ADHD.
Because many children with mild tics are never referred to specialists and never formally diagnosed, the true population prevalence of the full TS phenotype is almost certainly underestimated by clinical studies.
Diagnostic Criteria (DSM-5)
The DSM-5 (Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition) defines Tourette's Disorder with four criteria:
- Multiple motor tics AND at least one vocal (phonic) tic. Both types must be present at some point during the illness, though not necessarily simultaneously at any single observation.
- Duration of more than one year. Tics may wax and wane — they do not need to be present continuously. However, there must be no tic-free interval longer than 3 consecutive months during this year.
- Onset before age 18 years.
- Not attributable to another medical condition or substance. The tics cannot be better explained by the physiological effects of a substance (such as cocaine), another medical condition (such as Huntington disease, post-viral encephalitis, or other neurological conditions), or medication side effects.
An important change from earlier editions: the DSM-IV requirement that symptoms cause "marked distress or significant impairment" was removed in DSM-5. Many people with TS are not significantly impaired, yet still meet diagnostic criteria. This acknowledges the spectrum nature of TS and enables earlier identification of individuals who may benefit from monitoring or support even before impairment develops.
Other DSM-5 Tic Disorders
- Persistent (Chronic) Motor or Vocal Tic Disorder: One type of tic only (either motor or vocal, but not both), present for more than one year, onset before age 18.
- Provisional Tic Disorder: Motor and/or vocal tics present for less than one year since first tic onset. Very common in children; most resolve without treatment.
- Other Specified and Unspecified Tic Disorder: Tic disorder that does not meet full criteria for the above categories.
Pathophysiology
The core pathophysiology of TS involves dysfunction in the cortico-striato-thalamo-cortical (CSTC) circuits — the same neural loops implicated in OCD, ADHD, and other neurodevelopmental conditions. These circuits normally function to filter and gate sensorimotor signals, selecting appropriate actions and suppressing inappropriate ones. In TS, this filtering mechanism fails, allowing motor and vocal programs to "escape" into expression as tics.
Basal Ganglia and Striatal Dysfunction
The striatum (particularly the caudate nucleus and putamen) plays a central role. In TS, reduced activity of inhibitory GABAergic interneurons within the striatum — specifically cholinergic interneurons and parvalbumin-positive fast-spiking interneurons — is thought to impair local inhibition, allowing unwanted motor programs to reach the thalamus and cortex unchecked. Post-mortem studies have confirmed reductions in these interneuron populations in individuals with TS.
Dopamine Dysregulation
Dopamine is the central neurotransmitter implicated in TS, supported by several lines of evidence:
- Dopamine-blocking medications (antipsychotics such as haloperidol, fluphenazine, aripiprazole) reduce tics.
- Dopamine agonists and stimulants can transiently worsen or precipitate tics in susceptible individuals.
- PET imaging shows altered dopamine transporter and D2 receptor binding in the striatum of TS patients.
- VMAT2 inhibitors (valbenazine, deutetrabenazine), which deplete presynaptic dopamine stores, are effective tic-reducing treatments.
Other Neurotransmitters
The pathophysiology is not solely dopaminergic. Glutamate (excitatory) and GABA (inhibitory) imbalances within corticostriatal circuits are well-documented. Serotonin may modulate the OCD and anxiety components. The noradrenergic system is implicated by the efficacy of alpha-2 adrenergic agonists (guanfacine, clonidine) in reducing tics.
Neuroimaging Findings
Structural and functional MRI studies in TS have shown:
- Hyperactivation of the supplementary motor area (SMA) and sensorimotor cortex during tic generation
- Differences in caudate nucleus volume (typically reduced in TS)
- Increased activation of frontal inhibitory regions during periods of voluntary tic suppression — consistent with the effort required to hold back tics
- Thinning of sensorimotor cortex in some adult TS populations
The Premonitory Urge
A distinctive and clinically important feature of TS is the premonitory urge — an uncomfortable, buildup sensation in the body region where a tic is about to occur, similar to the urge to sneeze or scratch an itch. The tic temporarily relieves this sensation. This partially voluntary character of tics — the fact that they can be suppressed at the cost of increasing urge — is precisely why behavioral therapies such as Habit Reversal Training are effective. Patients learn to recognize the urge and redirect it before the tic fires.
Clinical Presentation
Tics are sudden, rapid, recurrent, nonrhythmic movements or vocalizations. They are classified by complexity (simple vs. complex) and by type (motor vs. vocal/phonic).
Motor Tics
Simple motor tics (most common first presentation):
- Eye blinking — typically the first tic to appear in most children with TS
- Nose twitching, facial grimacing
- Head jerking or nodding
- Shoulder shrugging
- Abdominal tensing, arm or leg jerking
Complex motor tics (sequential movements that appear more purposeful):
- Touching objects or other people
- Jumping, bending, twisting
- Dystonic postures (sustained abnormal positions)
- Copropraxia — making obscene gestures (occurs in a minority of cases)
- Echopraxia — imitating the movements of others
Vocal (Phonic) Tics
Simple vocal tics (among the most commonly misidentified — often dismissed as "habits"):
- Throat clearing — one of the most common vocal tics, frequently misinterpreted as a nervous habit or allergy symptom
- Sniffing, grunting, barking, squeaking
- Hissing or clicking sounds
Complex vocal tics:
- Words or phrases out of context
- Echolalia — repeating the words of others
- Palilalia — repeating one's own last words or syllables
- Coprolalia — involuntary uttering of obscene or socially inappropriate words or phrases. Despite popular perception, this occurs in only 10–15% of people with TS and is not required for the diagnosis. When present, it is often distressing to the individual, who experiences it as entirely unwanted.
Characteristic Tic Behaviors
- Suppressibility: Tics can typically be suppressed voluntarily for short periods, at the cost of a mounting sense of tension or urge that is released when the tic is finally allowed to occur.
- Waxing and waning: Tic type, location, frequency, and severity fluctuate over days, weeks, and months — even without any change in treatment. A parent who notices tics change from eye blinking to throat clearing is observing normal TS variability, not a new or worsening disorder.
- Situational variation: Tics worsen with stress, anxiety, excitement, fatigue, and illness. They typically diminish with focused concentration on absorbing tasks (such as playing a video game), and are often absent during sleep.
- Social reinforcement: Attention or reaction to tics — even negative attention — can transiently worsen them. Telling a child to "stop that" usually does not help and may increase anxiety, which worsens tics.
Natural History
The natural course of Tourette syndrome is broadly favorable, and this is one of the most important messages to convey to newly diagnosed families. Symptom improvement by late adolescence is the rule, not the exception.
Typical developmental trajectory:
- Ages 4–6: Simple motor tics emerge, most commonly eye blinking.
- Ages 6–10: Tic repertoire may expand; vocal tics typically appear. Tics may change in character and location.
- Ages 10–12: Peak tic severity. This is the most symptomatic period for most children with TS and often the time of initial referral for evaluation and treatment.
- Adolescence: Gradual improvement begins for the majority. Approximately 50–60% of children experience meaningful reduction in tic severity by late adolescence.
- Adulthood: Roughly 30% have mild, residual tics with minimal functional impact. Approximately 10% have persistent moderate-to-severe tics that continue to require active management into adulthood.
Long-term predictors of worse outcome (persistent tics into adulthood) include:
- Greater tic severity at age 10
- Comorbid OCD (especially if OCD symptoms are severe)
- Persistent ADHD
Even in adults with persistent TS, many develop improved capacity to suppress or manage tics with age and experience. Social and occupational functioning in adults with TS is often better than childhood severity would predict. TS does not affect intelligence, and people with TS succeed across every field of endeavor.
Comorbidities
The comorbid conditions associated with Tourette syndrome — particularly ADHD, OCD, and anxiety — frequently cause more day-to-day functional impairment than tics themselves. A complete clinical evaluation must assess for each of these conditions independently.
ADHD (Attention-Deficit/Hyperactivity Disorder)
Approximately 50% of individuals with TS also have ADHD. Combined TS+ADHD is associated with greater academic difficulties, social problems, and behavioral challenges than either condition alone. An important clinical point: stimulant medications (methylphenidate, amphetamine salts) do not uniformly worsen tics — the landmark TACTS (Treatment of ADHD in Children with Tics) trial demonstrated that methylphenidate was effective for ADHD symptoms and did not significantly worsen tics on average, with some individuals experiencing mild transient tic increases. For most children with TS+ADHD, treating the ADHD is appropriate and generally safe.
OCD (Obsessive-Compulsive Disorder)
OCD is present in approximately 30–40% of individuals with TS. Interestingly, "tic-related OCD" (OCD occurring in the context of TS) may differ phenomenologically from sporadic OCD:
- More likely to involve symmetry obsessions, "just right" or "not quite" sensations, ordering, and touching compulsions
- Less likely to involve contamination fears or elaborate harm-avoidance rituals
- May respond similarly to SSRIs and CBT (specifically exposure and response prevention, ERP)
Anxiety Disorders
Generalized anxiety disorder and social anxiety disorder each affect approximately 30% of individuals with TS. Anxiety also worsens tic severity directly, creating a reinforcing cycle. CBT for anxiety is an important component of comprehensive TS management.
Mood and Behavioral Comorbidities
- Rage attacks and explosive outbursts: Often underrecognized but reported in a significant minority of TS patients. These can be among the most disruptive features for families and may have roots in dysregulation of frontal-subcortical circuits.
- Depression: More common in adolescents and adults with TS, particularly those with greater tic severity and social difficulties.
- Learning disabilities: Visuomotor and executive function difficulties are more common in TS even after controlling for ADHD.
- Sleep disturbances: Difficulty falling asleep, motor activity during sleep, parasomnias.
- Sensory processing issues: Hypersensitivity to certain textures, sounds, or sensations is reported by many individuals with TS, consistent with broader sensorimotor dysregulation.
Diagnosis
Tourette syndrome is a clinical diagnosis. There is no blood test, imaging study, or biomarker that confirms TS. Diagnosis depends on a thorough history and clinical examination.
Clinical History
Key elements of the diagnostic history include:
- Exact age of first tic onset and type of first tic
- Full inventory of all motor and vocal tics observed or reported over the course of illness
- Duration: has the patient had tics for more than 12 months?
- Waxing and waning pattern: do tics change in type and frequency over time?
- Presence or absence of the premonitory urge
- Impact on daily life: school performance, social relationships, self-esteem
- Family history of tics, OCD, ADHD
- Assessment of all comorbid conditions (ADHD, OCD, anxiety, depression)
- Medication history: any prior or current use of stimulants, antipsychotics, antihistamines, or other agents that might affect tics
Ruling Out Secondary Causes
Several conditions can cause tic-like movements and must be considered:
- PANDAS/PANS (Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal Infections / Pediatric Acute-onset Neuropsychiatric Syndrome): Characterized by acute, dramatic onset of tics and/or OCD in temporal relationship to streptococcal infection. Diagnosed clinically; supported (but not confirmed) by elevated anti-streptococcal antibodies (ASO titer, anti-DNase B). A controversial but clinically important diagnosis to consider when onset is abrupt rather than gradual.
- Sydenham's chorea: Post-streptococcal chorea; irregular, flowing movements rather than repetitive tics; associated with rheumatic fever.
- Huntington disease: Adult-onset; genetic testing distinguishes.
- Drug-induced tics: Stimulants (amphetamine, cocaine), levodopa.
- Stereotypies of autism spectrum disorder: Usually more rhythmic and patterned than tics; context-dependent.
- Myoclonus, dystonia: Distinguished by clinical features and, when needed, neurophysiological testing.
Standardized Assessment Tools
The Yale Global Tic Severity Scale (YGTSS) is the gold-standard instrument for measuring tic severity in both clinical care and research. It rates motor and vocal tics separately on dimensions of number, frequency, intensity, complexity, and interference, producing a Total Tic Score (0–50) and an Overall Impairment Rating (0–50).
When to Order Tests
- Neuroimaging (MRI): Not routinely indicated. Consider when onset is atypical (adult onset, focal neurological signs, acute onset without family history).
- EEG: Not needed for routine TS. Consider only if seizure disorder is a question (tics and seizures are clinically distinct).
- Genetic testing: Not routine. May be warranted in atypical presentations.
- Streptococcal titers (ASO, anti-DNase B): Consider when PANDAS/PANS presentation is suspected.
Treatment
A fundamental principle guides TS treatment: treat tics only if they cause significant impairment. Many children with TS have tics that are mild, not distressing, and do not interfere with function. For these children, psychoeducation and watchful waiting are entirely appropriate — and often the kindest approach, since medications carry real side effects. Treatment targets should be identified collaboratively with the patient and family, and may include tics, ADHD, OCD, or anxiety depending on which causes the most impairment.
1. Psychoeducation (First Step for All Patients)
Educating the patient, family, school, and when appropriate peers and teachers, about the nature of TS is therapeutic in itself. Key messages: tics are involuntary (or semi-voluntary), they are not "acting out," the child is not doing this on purpose, reprimanding tics does not help and often makes them worse, and the prognosis is generally favorable. Connecting families with the Tourette Association of America provides peer support, camp programs, and advocacy resources.
2. Behavioral Therapies (First-Line for Mild to Moderate Tics)
Comprehensive Behavioral Intervention for Tics (CBIT) is now considered first-line treatment for children and adults with TS causing functional impairment. CBIT combines:
- Habit Reversal Training (HRT): The core technique. The patient learns to identify the premonitory urge signaling an impending tic, then practices a competing response — a sustained, incompatible voluntary movement or tension that prevents the tic from occurring. For example, if the tic is head jerking, a competing response might be slowly tensing the neck muscles to hold the head still. The competing response is held for 1 minute or until the urge subsides.
- Functional analysis: Identifying situations, environments, or emotional states that worsen tics, followed by strategies to modify those contexts.
- Relaxation training: Reducing the baseline anxiety that amplifies tic expression.
A landmark randomized controlled trial (Piacentini et al., JAMA 2010; PMID 20483968) demonstrated CBIT superiority over psychoeducation and supportive therapy in children, with a 52.5% vs. 18.5% responder rate. A parallel adult trial (Wilhelm et al., 2012) confirmed efficacy in adults. CBIT is effective, durable, and free of the side effects associated with medications.
3. Pharmacotherapy
Medications are considered when tics are moderate to severe, cause significant impairment, and have not responded adequately to behavioral therapy, or when behavioral therapy is not accessible.
Alpha-2 adrenergic agonists (preferred first-line medications for most patients):
- Guanfacine (extended-release formulation: Intuniv): Reduces tics and also treats comorbid ADHD and anxiety. Starting dose 0.5–1 mg/day; typically titrated to 1–4 mg/day. Main side effects: sedation (often improves with time), mild blood pressure reduction, occasional irritability on dose reduction. Better tolerated than clonidine in most children.
- Clonidine: Older agent, more sedating. Available in patch formulation (useful for children who cannot swallow tablets). Effective for tics and ADHD. More pronounced cardiovascular effects than guanfacine.
Antipsychotics (dopamine blockers — effective but requiring careful side-effect monitoring):
- Aripiprazole: Atypical antipsychotic with partial D2 agonist activity; currently the most commonly used antipsychotic for TS. Moderate tic-reduction efficacy with a better metabolic profile than older agents. Side effects: weight gain, sedation, akathisia (inner restlessness).
- Risperidone: Effective for tic reduction; metabolic monitoring (weight, glucose, lipids) is required with chronic use.
- Fluphenazine: Typical antipsychotic; effective for tics with less metabolic burden than atypicals in some comparisons. Requires monitoring for extrapyramidal symptoms and tardive dyskinesia with long-term use.
- Haloperidol: The first antipsychotic demonstrated to reduce tics. Effective but associated with significant extrapyramidal side effects, sedation, and tardive dyskinesia risk with prolonged use. Less preferred today.
VMAT2 inhibitors (newer, FDA-approved, no tardive dyskinesia risk):
- Valbenazine (Ingrezza): FDA-approved for Tourette syndrome in adults in 2023, representing the first new drug class approved specifically for TS. Mechanism: inhibits vesicular monoamine transporter 2 (VMAT2), depleting presynaptic dopamine stores without blocking dopamine receptors — this is why it does not cause tardive dyskinesia. Evidence: the T-FORCE randomized controlled trial demonstrated significant tic reduction vs. placebo. Side effects: sedation, QTc prolongation (monitor ECG), anticholinergic effects.
- Deutetrabenazine: Also a VMAT2 inhibitor studied for TS; used more widely for Huntington chorea.
Treating ADHD comorbidity:
- Stimulants (methylphenidate, amphetamine salts): Evidence supports use in TS+ADHD. The TACTS trial showed methylphenidate was effective for ADHD in children with tics without significant tic worsening on average. Individual responses vary; some patients experience transient mild tic increases. Clinical benefit from ADHD treatment often outweighs this risk.
- Atomoxetine: Norepinephrine reuptake inhibitor; effective for ADHD; some evidence for modest tic reduction as well.
- Guanfacine or clonidine: Address both tics and ADHD, particularly the hyperactivity/impulsivity component.
Treating OCD comorbidity:
- SSRIs (sertraline, fluvoxamine, fluoxetine) combined with cognitive-behavioral therapy using exposure and response prevention (ERP) are first-line for OCD in TS.
4. Deep Brain Stimulation (DBS)
DBS is reserved for severe, refractory adults (typically not children) with TS who have not responded adequately to multiple medications and behavioral therapies. DBS is not FDA-approved specifically for TS but is used at specialized centers under compassionate use or clinical trial protocols. Common targets include the centromedian nucleus of the thalamus, globus pallidus internus (GPi), and anterior limb of the internal capsule. Response rates vary; DBS for TS is considered experimental but promising for carefully selected patients.
Living with Tourette Syndrome
The daily experience of living with TS extends well beyond tics themselves. Social stigma, school challenges, exhaustion from tic suppression, and the ripple effects of comorbid ADHD and OCD on relationships and self-esteem are often the most significant burdens.
School and Social Environment
Many children voluntarily suppress tics throughout the school day — an effortful process that consumes cognitive and emotional resources. A common and important pattern: the child appears relatively tic-free at school (having suppressed them successfully) but "explodes" with worse tics, irritability, and behavioral dysregulation after returning home. This is sometimes mistaken for oppositional or manipulative behavior, when in fact it reflects exhaustion from a full day of effortful suppression. Educating parents and teachers about this phenomenon is essential.
Formal school accommodations may be warranted: extended time on tests, preferential seating, permission to step out briefly, or reduced pressure to suppress tics in class. Many schools can implement a 504 Plan or IEP to support children with TS and comorbid ADHD or learning disabilities.
Disclosure Decisions
Whether and how to disclose a TS diagnosis to classmates, teachers, or employers is a personal decision. Proactive, matter-of-fact disclosure — perhaps a classroom presentation about TS — often dramatically reduces teasing and social difficulties. Many children report that once peers understand what tics are, the teasing stops. Employers are legally required to provide reasonable accommodations under the Americans with Disabilities Act (ADA) for individuals with TS whose symptoms significantly affect work performance.
Peer Support and Community
The Tourette Association of America (TAA) offers summer camps, online communities, a national conference, and a network of local chapters. Peer support from others who have lived experience with TS — including adults who have successfully navigated careers, relationships, and family life with TS — is powerfully normalizing for newly diagnosed children and their families.
Notable Individuals with Tourette Syndrome
A number of accomplished individuals have publicly disclosed their TS diagnoses, demonstrating that TS does not limit human potential:
- Tim Howard — professional soccer goalkeeper and U.S. national team player
- Dan Aykroyd — actor and comedian (Blues Brothers, Ghostbusters)
- Billie Eilish — Grammy Award-winning musician (self-reported)
- Michael Wolff — jazz pianist
Wellbeing and Long-Term Perspective
Studies of adults with TS generally find levels of quality of life, employment, and relationship satisfaction that are comparable to or better than would be predicted from childhood tic severity alone. For most people, TS is a manageable condition — one that requires understanding, appropriate treatment of comorbidities, and self-advocacy, but that does not define the ceiling of what a person can achieve.
Recent Research and Advances
Research into Tourette syndrome has accelerated significantly in recent years, driven by advances in genetics, neuroimaging, and treatment development.
Genetics
Large-scale genome-wide association studies (GWAS) are beginning to identify specific genetic loci associated with TS risk. The genetic architecture appears complex, involving many common variants of small effect rather than a single gene. Rare copy number variants (CNVs) and point mutations in genes affecting neuronal development (including histidine decarboxylase, SLITRK1, and others) have been implicated in some families. The overlap in genetic risk between TS, OCD, and ADHD is being actively studied and supports their shared neurobiological roots.
Immunological Hypotheses
Growing evidence links TS to immune dysregulation. The PANDAS/PANS hypothesis proposes that molecular mimicry between streptococcal antigens and basal ganglia proteins triggers autoimmune tic exacerbations. Beyond streptococcus, broader inflammatory processes may modulate tic severity, explaining why infections commonly worsen tics. Research into anti-neuronal antibodies, microglial activation, and the gut-brain axis continues.
Novel Therapeutics
The FDA approval of valbenazine (Ingrezza) for TS in adults in 2023 marked the first new drug class specifically approved for TS in decades. VMAT2 inhibitors offer tic control without the tardive dyskinesia risk of antipsychotics — a meaningful advance for patients requiring long-term pharmacotherapy. Clinical trials of deutetrabenazine and other VMAT2 inhibitors in pediatric TS populations are ongoing.
Digital CBIT delivery — behavioral therapy via app or telehealth — is expanding access to first-line non-pharmacological treatment in regions without specialist behavioral therapists.
Transcranial Magnetic Stimulation (TMS)
Non-invasive brain stimulation with TMS is under investigation for TS, targeting the supplementary motor area and motor cortex. Early evidence suggests potential tic reduction, but large randomized trials are needed before TMS becomes a standard recommendation.
References & Research
- Robertson MM. Tourette syndrome, associated conditions and the complexities of treatment. Brain. 2000;123(3):425–462. PMID: 10686169. DOI: 10.1093/brain/123.3.425
- Leckman JF. Tourette's syndrome. Lancet. 2002;360(9345):1577–1586 — Search PubMed. DOI: 10.1016/S0140-6736(02)11526-1
- Pringsheim T, Jette N, Frolkis A, Steeves TDL. The prevalence of Tourette syndrome: a systematic review and meta-analysis. Mov Disord. 2014;29(8):1089–1099 — Search PubMed. DOI: 10.1002/mds.25945
- Piacentini J, Woods DW, Scahill L, et al. Behavior therapy for children with Tourette disorder: a randomized controlled trial. JAMA. 2010;303(19):1929–1937 — Search PubMed. DOI: 10.1001/jama.2010.607
- Wilhelm S, Peterson AL, Piacentini J, et al. Randomized trial of behavior therapy for adults with Tourette syndrome. Arch Gen Psychiatry. 2012;69(8):795–803. PMID: 22868933. DOI: 10.1001/archgenpsychiatry.2011.1528
- Bloch MH, Leckman JF. Clinical course of Tourette syndrome. J Psychosom Res. 2009;67(6):497–501 — Search PubMed. DOI: 10.1016/j.jpsychores.2009.09.002
- Treatment of ADHD in Children with Tics (TACTS) Study Group. Treatment of ADHD in children with tics: a randomized controlled trial. N Engl J Med. 2002;347(18):1313–1321 — Search PubMed. DOI: 10.1056/NEJMoa021164
- Pringsheim T, Doja A, Gorman D, et al. Canadian guidelines for the evidence-based treatment of tic disorders: pharmacotherapy. Can J Psychiatry. 2012;57(3):133–143. PMID: 22397999. DOI: 10.1177/070674371205700302
- Cavanna AE, Servo S, Monaco F, Robertson MM. The behavioral spectrum of Gilles de la Tourette syndrome. J Neuropsychiatry Clin Neurosci. 2009;21(1):13–23. PMID: 19359447. DOI: 10.1176/jnp.2009.21.1.13
- Albin RL, Mink JW. Recent advances in Tourette syndrome research. Trends Neurosci. 2006;29(3):175–182. PMID: 16430974. DOI: 10.1016/j.tins.2006.01.001
- Schrock LE, Mink JW, Woods DW, et al. Tourette syndrome deep brain stimulation: a review and updated recommendations. Mov Disord. 2015;30(4):448–471. PMID: 25476818. DOI: 10.1002/mds.26094
- Jankovic J. Tourette's syndrome. N Engl J Med. 2001;345(16):1184–1192 — Search PubMed. DOI: 10.1056/NEJMra010032
Research Papers
Search PubMed for the latest peer-reviewed research on Tourette syndrome:
- Tourette syndrome treatment review
- Habit reversal training CBIT tics
- Tourette syndrome ADHD comorbidity
- Tourette syndrome OCD
- Alpha-2 agonist guanfacine tics
- Aripiprazole Tourette syndrome
- Valbenazine VMAT2 tic disorder
- Tourette syndrome natural history prognosis
- Tourette syndrome pathophysiology corticostriatal
- PANDAS streptococcal tic disorder
- Deep brain stimulation Tourette syndrome
- Tourette syndrome prevalence epidemiology
Connections
- Neurology
- Epilepsy
- Huntington's Disease
- Parkinson's Disease
- Alzheimer's Disease
- Restless Legs Syndrome
- Multiple Sclerosis
- Fatigue
- Anxiety
- GABA