Acanthamoeba Symptoms and Diagnosis
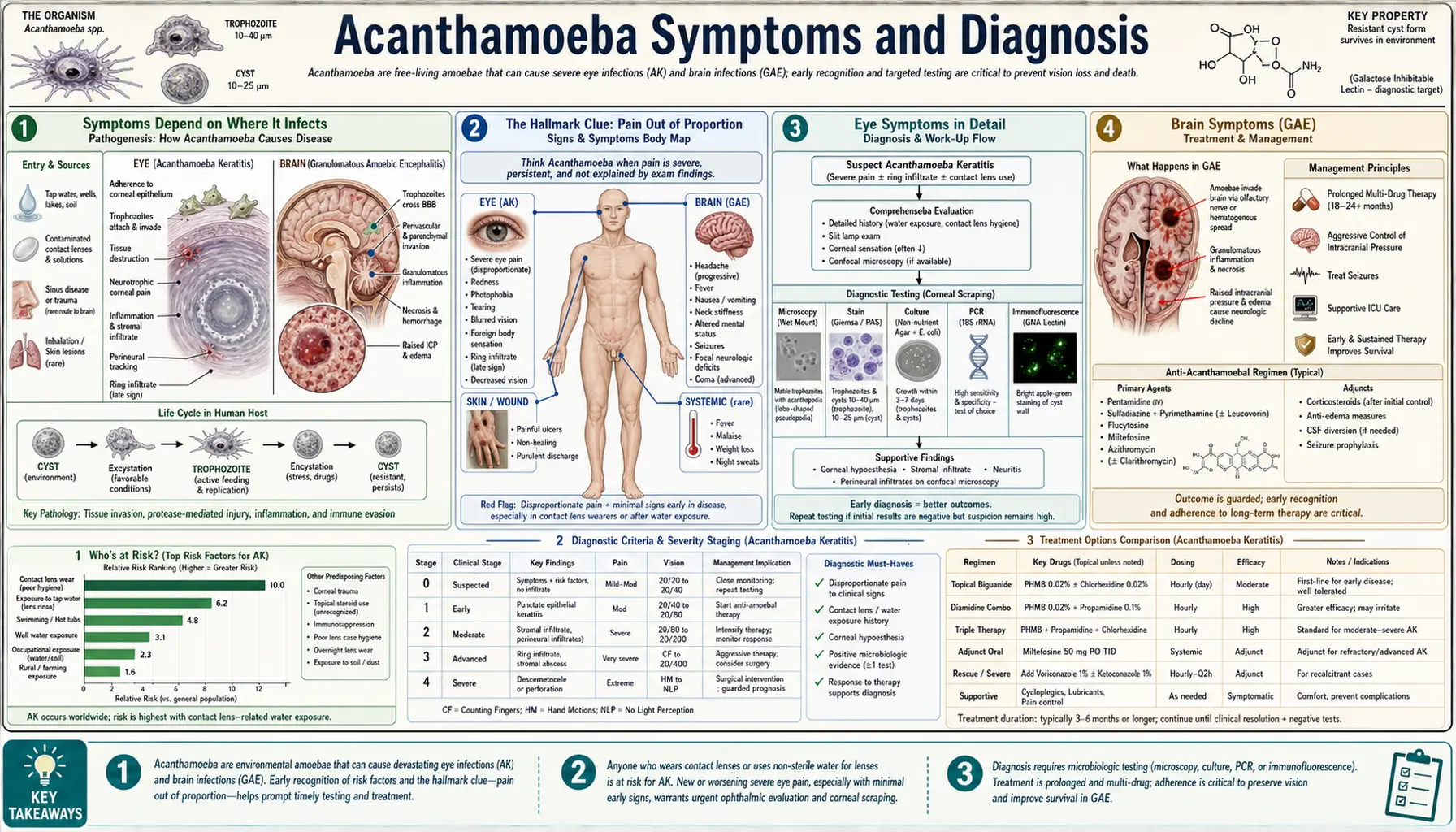
Acanthamoeba is a single microbe that can cause three strikingly different illnesses, depending on which part of the body it reaches. By far the most common is a sight-threatening eye infection in contact lens wearers; far rarer but often fatal are a slow brain infection and skin infections that strike people with weakened immune systems. The thread that ties the eye disease together — and the clue clinicians most often miss — is pain that seems wildly out of proportion to how the eye actually looks. This page explains what each form feels like, why the infection is so frequently mistaken for something else, and how doctors confirm the diagnosis.
Acanthamoeba Keratitis (Eye)
The sight-threatening corneal infection of contact lens wearers — severe pain, light sensitivity, and the telltale ring-shaped corneal infiltrate.
Granulomatous Amebic Encephalitis (Brain)
A slow, insidious brain infection that develops over weeks, almost exclusively in people with weakened immune systems.
Cutaneous & Disseminated Infection (Skin)
Firm nodules, non-healing ulcers, and abscesses — mainly in immunocompromised patients, sometimes spreading to other organs.
Table of Contents
- Symptoms Depend on Where It Infects
- The Hallmark Clue: Pain Out of Proportion
- Eye Symptoms in Detail
- Brain Symptoms (GAE)
- Skin Symptoms
- Why It Is So Often Misdiagnosed
- How Doctors Diagnose It
- Red Flags: When to Seek Emergency Eye Care
- Key Research Papers
- Featured Videos
1. Symptoms Depend on Where It Infects
One of the most confusing things about Acanthamoeba is that the very same amoeba produces three completely different illnesses. There is no single "Acanthamoeba symptom" — what you experience depends entirely on which tissue the organism manages to colonize. Understanding this is the first step to recognizing the infection, because a patient and a clinician thinking about an eye problem will never connect it to a brain or skin problem unless they know all three are caused by the same microbe.
The three forms are:
- Eye infection (Acanthamoeba keratitis) — an infection of the cornea, the clear dome at the front of the eye. This is overwhelmingly the most common presentation and is strongly tied to contact lens wear. It threatens vision but is usually not life-threatening.
- Brain infection (granulomatous amebic encephalitis, GAE) — a slow, smoldering infection of the brain and its lining. It is very rare, develops over weeks, and occurs almost exclusively in people whose immune systems are weakened. It is frequently fatal.
- Skin and spreading infection (cutaneous and disseminated disease) — firm skin nodules, non-healing ulcers, and abscesses, again mostly in immunocompromised patients. From the skin the infection can spread (disseminate) to the lungs, sinuses, and even the brain.
The same organism behaves so differently because the eye, the brain, and the skin offer very different conditions. The healthy immune system normally clears Acanthamoeba from the bloodstream and internal organs, which is why brain and skin disease are seen almost only in people whose defenses are compromised. The cornea, by contrast, has no blood vessels and limited immune surveillance, so the amoeba can establish itself there even in otherwise healthy young people — provided it is given a foothold, usually by a contact lens.
2. The Hallmark Clue: Pain Out of Proportion
If there is one feature that should make any clinician think of Acanthamoeba in the eye, it is pain that is wildly out of proportion to how the eye looks. A patient may be in agony, yet on examination the eye appears only mildly red or even nearly normal. This mismatch is the single most useful early warning sign.
The reason is anatomical. As the infection takes hold, Acanthamoeba attacks the corneal nerves. The cornea is the most densely innervated tissue in the entire human body — it has the highest concentration of sensory nerve endings of any surface, which is why even a tiny eyelash or grain of sand on the eye is so intensely uncomfortable. When the amoeba inflames and damages this exceptionally rich nerve network (a process called radial keratoneuritis when the inflamed nerves become visible), the result is severe, often disabling pain.
Patients struggle to describe it, but a recurring phrase is that it "feels like there's glass in my eye." The pain can keep people awake at night and is frequently far worse than the redness or visible damage would suggest. An ordinary-looking eye combined with agonizing pain is, in effect, the signature of Acanthamoeba keratitis — and tragically, it is also the clue most easily brushed aside as an overreaction.
3. Eye Symptoms in Detail
The eye form — Acanthamoeba keratitis — usually affects one eye and develops over days to weeks. Early on, the symptoms are non-specific and overlap with many common eye problems, which is exactly why it is so often missed. The typical features include:
- Severe eye pain — often the dominant complaint, and characteristically out of proportion to the visible findings (see above).
- Redness — the eye is inflamed, though sometimes surprisingly little given the pain.
- Extreme light sensitivity (photophobia) — bright light becomes painful, and many patients keep the affected eye shut or wear sunglasses indoors.
- Watering and tearing — the eye streams, and the eyelid may be in spasm.
- Foreign-body sensation — the persistent feeling that something is in the eye, often described as a "grain of sand" or piece of grit that cannot be washed out.
- Blurred vision — sight becomes hazy as the cornea is affected.
As the disease progresses over several weeks, a more specific sign can appear: a ring-shaped infiltrate in the cornea — a circular zone of inflammatory cells encircling the central infection. This ring is a classic (though late) feature of Acanthamoeba keratitis. Unfortunately, by the time the ring is visible the infection is usually well established.
Because the early symptoms are so generic, Acanthamoeba keratitis is frequently misread at first as herpes simplex keratitis (a viral infection of the cornea) or as bacterial keratitis. Patients are often started on antiviral or antibiotic drops that do nothing against an amoeba, and the diagnosis is only reconsidered when the eye fails to improve — or gets worse — over the following weeks.
4. Brain Symptoms (GAE)
Granulomatous amebic encephalitis (GAE) is the brain form of Acanthamoeba infection. Unlike the dramatic, fast-moving amebic meningitis caused by a different organism (Naegleria fowleri), GAE is insidious — it creeps up slowly, typically over weeks to months, which often delays recognition until the disease is advanced.
GAE occurs almost exclusively in people with weakened immune systems: those with advanced HIV/AIDS, organ transplant recipients on immunosuppressant drugs, people receiving chemotherapy, and others with chronic illness or long-term steroid use. The amoeba reaches the brain through the bloodstream, usually after entering the body through the skin, lungs, or sinuses.
The symptoms reflect a slowly expanding infection and inflammation within the brain, and may include:
- Persistent headache — often the earliest and most constant symptom, building gradually.
- Low-grade fever — usually mild rather than the high fevers of acute meningitis.
- Stiff neck — a sign of irritation of the membranes covering the brain.
- Behavioral and mental-status changes — confusion, personality change, drowsiness, or altered awareness.
- Focal neurological deficits — weakness, numbness, vision changes, or speech difficulty affecting one part of the body, depending on which area of the brain is involved.
- Seizures — which can occur as the infection irritates the brain tissue.
Because these features develop slowly and resemble other neurological conditions — brain tumors, tuberculosis of the brain, or other opportunistic infections — GAE is notoriously difficult to diagnose during life, and is often only confirmed at autopsy.
5. Skin Symptoms
The cutaneous (skin) form of Acanthamoeba infection, like GAE, occurs mainly in people whose immune systems are compromised. It can appear on its own or as part of a wider, disseminated infection that spreads through the body. The skin lesions are persistent and do not respond to ordinary treatment, which is often what eventually prompts a biopsy.
Typical skin findings include:
- Firm nodules — hard, often tender lumps under the skin.
- Non-healing ulcers — open sores that fail to heal despite standard wound care and antibiotics.
- Abscesses — collections of pus within or beneath the skin.
From the skin, the infection can extend to involve the sinuses and lungs, and in disseminated disease it may reach the brain, producing GAE. Because skin lesions can be the first visible sign of a deeper, spreading infection, their appearance in an immunocompromised patient is taken seriously and investigated with biopsy and culture.
6. Why It Is So Often Misdiagnosed
Acanthamoeba infection is one of the most frequently missed diagnoses in its category, and the reasons are worth understanding — because the delay itself is what causes much of the harm.
It is rare. Many clinicians, including some experienced eye doctors, may go an entire career without seeing a single case. When a condition is this uncommon, it simply does not come to mind, and the mind tends to reach for the common explanations first.
Early on, it mimics common infections. In the eye, the first symptoms are indistinguishable from herpes or bacterial keratitis; in the brain, GAE looks like other neurological illnesses; on the skin, the lesions resemble ordinary infections. The default assumption is almost always the more common condition, and patients are treated accordingly — with drops or antibiotics that have no effect on an amoeba.
The best clue is easy to dismiss. The telltale sign — eye pain wildly out of proportion to the visible findings — is precisely the kind of thing that can be written off as a patient overreacting or being unusually sensitive. When the most distinctive feature of a disease can be mistaken for exaggeration, that disease will be missed.
The cost of these delays is real. Every week that passes while the wrong treatment is given, the amoeba burrows deeper into the cornea (or, in the rarer forms, into deeper tissue). In the eye, early diagnosis and treatment dramatically improve the chances of saving vision, while late diagnosis can mean months of treatment, corneal scarring, and sometimes the need for a corneal transplant. Recognizing the pattern early is the single most important factor in a good outcome.
7. How Doctors Diagnose It
Confirming Acanthamoeba requires specialized testing, because the organism does not show up on the routine tests used for ordinary infections. The approach differs by which form is suspected.
Diagnosing the eye infection (keratitis)
- In vivo confocal microscopy — a specialized, painless eye-imaging technique that lets an examiner look at the living cornea at very high magnification, layer by layer, without touching or cutting it. It can directly visualize Acanthamoeba cysts — the dormant, double-walled form of the amoeba — as bright round structures within the cornea. When available, it is one of the fastest non-invasive ways to support the diagnosis.
- Corneal scraping with culture — the doctor gently scrapes a small sample of cells from the surface of the infected cornea and sends it to the laboratory. Acanthamoeba will not grow on ordinary culture plates, so the sample is placed on a special non-nutrient agar plate that has been seeded with a lawn of E. coli bacteria. The amoebae feed on the bacteria and crawl across the plate, leaving visible tracks that confirm their presence.
- PCR (polymerase chain reaction) — a molecular test that detects Acanthamoeba DNA in the corneal sample. PCR is highly sensitive and can give a faster answer than waiting for the amoebae to grow in culture.
Diagnosing the brain and skin forms
- Skin biopsy and PCR — for cutaneous disease, a small piece of the affected skin is removed and examined under the microscope for amoebae, and tested by PCR for Acanthamoeba DNA.
- Cerebrospinal fluid (CSF) analysis — for suspected GAE, fluid drawn from around the spinal cord by lumbar puncture can be examined, though the amoeba is often hard to find this way.
- Neuroimaging — CT and MRI scans of the brain can reveal areas of inflammation, swelling, or mass-like lesions that raise suspicion for GAE, although the appearance is not unique to Acanthamoeba.
- Brain biopsy — in many cases of GAE, a definitive diagnosis requires sampling brain tissue directly, which is why the condition is so often confirmed only late or after death.
In practice, the diagnosis often depends on a clinician thinking of Acanthamoeba in the first place and then ordering the right specialized test — which is why awareness of the symptom pattern matters so much.
8. Red Flags: When to Seek Emergency Eye Care
For the vast majority of people, the practical takeaway concerns the eye. The most important warning pattern is simple:
A contact lens wearer with worsening eye pain and light sensitivity that is NOT improving on antibiotic drops should be evaluated urgently by a corneal specialist for Acanthamoeba.
Specific red flags that warrant prompt, in-person evaluation rather than waiting it out include:
- Eye pain that feels out of proportion to how the eye looks — the classic "glass in my eye" sensation.
- Severe light sensitivity that keeps you from opening the eye normally.
- An eye that is getting worse, not better, after several days of prescribed antibiotic or antiviral drops.
- A persistent foreign-body or "grain of sand" sensation that does not resolve.
- Any of the above in someone who wears contact lenses, especially with a history of swimming, showering, or using tap water while wearing lenses.
Why the urgency? Because in Acanthamoeba keratitis, time changes the outcome. Caught early, the infection can often be brought under control with a good chance of preserving vision. Allowed to progress, it can scar the cornea, threaten sight, and require many months of intensive treatment or even corneal transplantation. If you wear contact lenses and your eye is painfully not improving, do not assume it is a stubborn ordinary infection — ask specifically to be evaluated for Acanthamoeba by an eye specialist.
Key Research Papers
Peer-reviewed studies and authoritative reviews on the symptoms, diagnosis, and biology of Acanthamoeba infection — spanning keratitis (the eye disease), granulomatous amebic encephalitis (the brain disease), and confocal-microscopy diagnosis. Each citation links to the full text via DOI.
- Lorenzo-Morales J, Khan NA, Walochnik J. An update on Acanthamoeba keratitis: diagnosis, pathogenesis and treatment. Parasite. 2015;22:10.
- Marciano-Cabral F, Cabral G. Acanthamoeba spp. as agents of disease in humans. Clinical Microbiology Reviews. 2003;16(2):273–307.
- Visvesvara GS, Moura H, Schuster FL. Pathogenic and opportunistic free-living amoebae: Acanthamoeba spp., Balamuthia mandrillaris, Naegleria fowleri, and Sappinia diploidea. FEMS Immunology & Medical Microbiology. 2007;50(1):1–26.
- Khan NA. Acanthamoeba: biology and increasing importance in human health. FEMS Microbiology Reviews. 2006;30(4):564–595.
- Maycock NJR, Jayaswal R. Update on Acanthamoeba keratitis: diagnosis, treatment, and outcomes. Cornea. 2016;35(5):713–720.
- Carnt N, Hoffman JJ, Verma S, et al. Acanthamoeba keratitis: confirmation of the UK outbreak and a prospective case-control study identifying contributing risk factors. British Journal of Ophthalmology. 2018;102(12):1621–1628.
- Lee HJ, Alipour F, Cruzat A, et al. Utility of in vivo confocal microscopy in diagnosis of Acanthamoeba keratitis: a comparison of patient outcomes. Cornea. 2023;42(2):135–140.
- Kalra SK, Sharma P, Shyam K, Tejan N, Ghoshal U. Acanthamoeba and its pathogenic role in granulomatous amebic encephalitis. Experimental Parasitology. 2020;208:107788.
Live PubMed Searches
Each link opens a live PubMed query so results stay current as new papers are indexed.
- Acanthamoeba keratitis diagnosis
- Acanthamoeba keratitis confocal microscopy
- Acanthamoeba keratitis contact lens
- Acanthamoeba radial keratoneuritis pain
- Granulomatous amebic encephalitis
- Cutaneous Acanthamoeba immunocompromised
- Acanthamoeba keratitis misdiagnosis
- Acanthamoeba PCR and culture
Connections
- Acanthamoeba
- Acanthamoeba Keratitis
- Granulomatous Amebic Encephalitis
- Cutaneous & Disseminated Infection
- Acanthamoeba Treatments
- Parasites
- Ophthalmology
- Dry Eye Disease
- Meningitis
- Escherichia coli
- Infectious Disease
- Neurology
- Dermatology
- All Conditions