Acanthamoeba — The Free-Living Amoeba That Lives in Water
Symptoms & Diagnosis
How the three forms of Acanthamoeba infection announce themselves, and the lab tests — confocal microscopy, culture, and PCR — used to confirm the diagnosis.
Acanthamoeba Keratitis
The painful, sight-threatening corneal infection that strikes mostly contact lens wearers — warning signs, diagnosis, and why early recognition saves vision.
Granulomatous Amebic Encephalitis
The rare, slow, usually fatal brain infection that almost exclusively affects people with weakened immune systems.
Cutaneous & Disseminated Infection
Skin nodules and ulcers that can seed the bloodstream and spread to the lungs, sinuses, and other organs in immunocompromised patients.
Treatment Overview
Why the cyst stage makes Acanthamoeba so hard to kill, and a survey of the medical and adjunct approaches used against it.
Conventional Treatment
The standard biguanide-and-diamidine eye-drop regimens for keratitis and the combination drug strategies used for brain and skin disease.
Ivermectin
What is — and is not — known about ivermectin in the context of Acanthamoeba, kept strictly to the evidence.
Castor Oil
A look at castor oil claims set against what the research actually supports, with honest framing of the limits.
Table of Contents
- What Is Acanthamoeba?
- Two Life Forms: Trophozoite and Cyst
- How It Damages Tissue
- The Three Diseases It Causes
- How People Get Infected
- The “Trojan Horse” Problem
- Acanthamoeba vs. Naegleria fowleri
- Epidemiology and Why Cases Are Rising
- Prevention
- Key Research Papers
- Featured Videos
1. What Is Acanthamoeba?
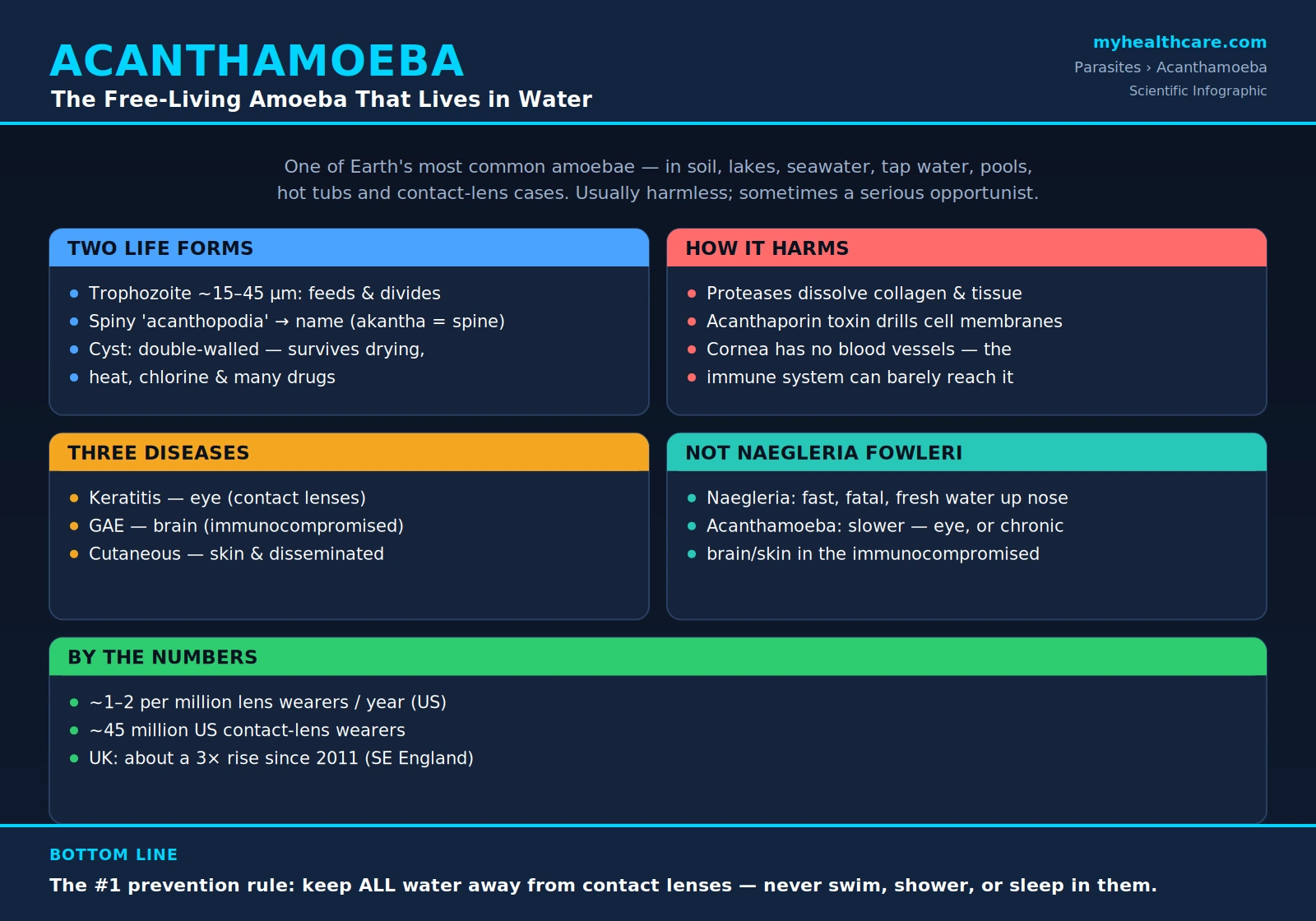
Acanthamoeba is one of the most common free-living amoebae on Earth. “Free-living” means it does not need a host to survive — unlike a tapeworm or malaria parasite that can only live inside an animal, Acanthamoeba spends almost its entire existence on its own in the environment. It is a single-celled protozoan, a microscopic creature far larger and more complex than a bacterium but still invisible to the naked eye.
Where does it live? Almost anywhere there is moisture. It has been recovered from soil, dust, lakes, rivers, ponds, seawater, swimming pools, hot tubs, drinking-water systems and tap water, bottled water, heating and air-conditioning units, dental-unit waterlines, dialysis machines, and the inside of contact lens cases. It is genuinely everywhere — one of the reasons it took microbiologists a long time to take it seriously as a cause of disease, since finding the amoeba in a sample does not automatically prove it caused an illness.
For the vast majority of its life, Acanthamoeba is completely harmless to people. Out in a pond or in the soil it behaves as a tiny grazer, crawling along surfaces and eating bacteria, algae, and other microbes. It plays a normal ecological role, helping to keep microbial populations in check. The trouble starts only under particular conditions — when the amoeba is pressed against a vulnerable surface like the cornea of the eye, or when it encounters a person whose immune system is badly weakened. In those settings it becomes an opportunistic pathogen: an organism that normally minds its own business but will cause serious disease if the opportunity arises.
2. Two Life Forms: Trophozoite and Cyst
Acanthamoeba has two distinct life stages, and understanding the difference between them explains almost everything about why its infections are so stubborn. The first is the trophozoite — the active, feeding, dividing form. A trophozoite is roughly 15 to 45 micrometers across (a few hundredths of a millimeter) and moves by pushing out fine, spiky projections called acanthopodia. The name of the entire genus comes from these spines: the Greek word akantha means “spine” or “thorn.” In this stage the amoeba grazes on bacteria, grows, and reproduces by simply splitting in two.
The second form is the cyst, and it is the reason Acanthamoeba is so hard to eradicate. When conditions turn hostile — the food runs out, the water dries up, the temperature swings, or it is hit with a disinfectant or a drug — the trophozoite can transform itself into a tough, dormant cyst. The cyst seals itself inside a double-layered protective wall and effectively shuts down, waiting out the bad times. In this armored state the amoeba can survive being dried out completely, frozen, heated, and bathed in chlorine. It can persist for years and then, when conditions improve, crack open and release a living trophozoite again.
This double-walled cyst is precisely why Acanthamoeba infections are notoriously difficult to cure. Many antibiotics and antiseptics that readily kill the active trophozoite cannot penetrate the cyst wall. A treatment can wipe out every trophozoite in sight, only for surviving cysts to reactivate weeks later and restart the infection. Effective therapy therefore has to either kill the cysts directly or be continued long enough to catch each amoeba as it emerges — one of the central challenges in treating any disease this organism causes.
3. How It Damages Tissue
When Acanthamoeba does cause disease, it injures the body through a combination of mechanical attachment and chemical weapons. First it grips onto host cells, using surface proteins (notably a mannose-binding adhesin) to lock on. Once attached, it goes to work breaking the tissue down.
The amoeba secretes a battery of enzymes — in particular proteases, which are protein-cutting enzymes, including ones that degrade collagen, the structural scaffolding that holds tissue together. In the eye, this collagen-dissolving activity is part of why Acanthamoeba keratitis can eat into the cornea and threaten sight. These secreted enzymes also help the amoeba push through tissue barriers and dampen local defenses.
One of its most striking weapons is a pore-forming toxin called acanthaporin. A pore-forming toxin works exactly as it sounds: it inserts itself into the outer membrane of a host cell and drills an open channel straight through it. Punching holes in a cell’s membrane causes its contents to leak out and its internal balance to collapse, killing the cell. Acanthaporin is also directly toxic to certain bacteria, a clue that this machinery first evolved for the amoeba’s ordinary job of hunting microbes — only to double as a tool for destroying human cells when the amoeba turns pathogenic. Together, the grip, the tissue-dissolving enzymes, and the pore-forming toxin allow Acanthamoeba to break down and invade tissue.
4. The Three Diseases It Causes
Despite being everywhere, Acanthamoeba causes human disease only rarely, and when it does it produces three quite different illnesses depending on how and where it gets in.
(a) Acanthamoeba keratitis is an infection of the cornea — the clear front window of the eye. It is painful, slow to diagnose, and potentially blinding. It occurs overwhelmingly in contact lens wearers and is the form of Acanthamoeba infection that an otherwise healthy person is most likely to face. Severe pain that seems out of proportion to what the eye looks like, redness, light sensitivity, and the feeling of something stuck in the eye are typical warning signs. Caught early it can often be treated; caught late it can scar the cornea and destroy vision.
(b) Granulomatous amebic encephalitis (GAE) is a rare infection of the brain. Unlike a sudden, explosive brain infection, GAE develops slowly over weeks, with headaches, confusion, personality changes, seizures, and neurological decline. It occurs almost exclusively in people whose immune systems are seriously compromised — for example those with advanced HIV/AIDS, organ-transplant recipients on immune-suppressing drugs, or patients on chemotherapy. GAE is very difficult to diagnose in time and is usually fatal.
(c) Cutaneous and disseminated infection shows up as firm skin nodules, ulcers, or non-healing sores, again mainly in immunocompromised people. The danger is that the infection does not always stay in the skin: it can seed the bloodstream and spread (disseminate) to the lungs, sinuses, and other organs, and from there potentially reach the brain. Skin involvement is therefore taken as a serious warning sign in a vulnerable patient.
5. How People Get Infected
The route of infection differs sharply between the eye disease and the brain or skin disease, and the difference comes down to who is exposed and how.
For keratitis, the key culprit is the combination of water and a contact lens. The amoeba is present in tap water, shower water, swimming-pool and hot-tub water, lake and ocean water. Normally, even if a little splashes into the eye, the constant blinking and tear flow flush it away. A contact lens changes that. The lens can trap the amoeba in the thin layer of fluid between the plastic and the cornea, holding it pressed against the eye’s surface long enough to take hold. In effect, a contact lens “props the door open” for an organism the eye would otherwise wash out. This is why swimming, showering, or rinsing lenses in tap water while wearing or storing them is so strongly discouraged.
For GAE and cutaneous infection, the entry routes are different: inhalation of the amoeba (in dust or aerosolized water) into the lungs or sinuses, or its entry through a break in the skin, after which it can seed the bloodstream. Crucially, these severe forms develop almost only in people who are already immunocompromised — a healthy immune system normally clears the amoeba before it can establish itself.
One reassuring point cuts across all of this: Acanthamoeba cannot penetrate healthy, intact skin. It needs a cut, a wound, a mucous membrane, or the trapped-water situation created by a contact lens to gain a foothold. Simply touching pond water or soil with unbroken skin does not, by itself, cause infection.
6. The “Trojan Horse” Problem
Acanthamoeba creates a public-health headache that has nothing to do with infecting people directly. Because it is a hunter that eats bacteria, it interacts constantly with the microbial world — and some bacteria have learned to turn the tables. Certain disease-causing bacteria can be taken up by the amoeba but then resist being digested, surviving and even multiplying inside it.
The classic example is Legionella, the bacterium that causes Legionnaires’ disease. Legionella can live and replicate inside Acanthamoeba, using the amoeba as a sheltered nursery. This is the “Trojan Horse” problem: when water systems are treated with disinfectants to kill bacteria, the bacteria hiding inside amoebae — and especially inside the tough amoebic cysts — are shielded from the chemicals. The amoeba acts like an armored transport that smuggles live pathogens past defenses meant to destroy them.
This matters enormously for the safety of plumbing, cooling towers, hospital water systems, and any engineered water network. Controlling Legionella and similar organisms is much harder when they can take refuge inside an amoeba that resists the very treatments designed to sanitize the water. The presence of Acanthamoeba in a water system is therefore a concern not only for the amoeba itself but for the bacterial passengers it can protect.
7. Acanthamoeba vs. Naegleria fowleri
It is very easy to confuse Acanthamoeba with another free-living amoeba, Naegleria fowleri, the famous “brain-eating amoeba” — but they behave completely differently, and conflating them causes needless fear and misunderstanding.
Naegleria fowleri causes primary amebic meningoencephalitis (PAM), which is fast and almost always fatal. It strikes when warm fresh water — typically from a lake, river, or hot spring — is forced up the nose, often during swimming or diving. From the nasal passages the amoeba travels along the olfactory nerve directly into the brain and destroys tissue within days. PAM is an acute, explosive, rapidly lethal infection of otherwise healthy young people, and it is genuinely the “brain-eating” scenario the headlines describe. (See our page on meningitis for context on infections of the brain’s coverings.)
Acanthamoeba is the slower, more insidious cousin. It does not race up the nose into the brain of a healthy swimmer. Instead it targets the eye in contact lens wearers, or causes a chronic, weeks-long brain or skin disease almost exclusively in the immunocompromised. Where Naegleria is a sudden catastrophe in the healthy, Acanthamoeba is a slow-burning opportunist. Keeping the two straight is essential: the risk situations, the people affected, the speed, and the prevention measures are all different.
8. Epidemiology and Why Cases Are Rising
Acanthamoeba keratitis is rare in absolute terms but is closely tied to contact lens use. In the United States it strikes on the order of one to two cases per million contact lens wearers per year. That sounds tiny — until you consider that an estimated 45 million Americans wear contact lenses, which means even a low per-person risk translates into a meaningful number of cases nationwide, the overwhelming majority of them in lens wearers.
There is also evidence that cases have been climbing in some regions. A 2018 study from a leading London eye hospital documented a roughly threefold rise in Acanthamoeba keratitis in southeast England since 2011 (Carnt and colleagues). The same body of work underscored how damaging the disease can be: roughly one in four affected patients ended up with less than 25 percent of their vision or were left blind. Suspected drivers of the increase include patterns of contact lens hygiene, reusable lenses and storage cases, and exposure of lenses to water — all modifiable behaviors, which is encouraging because it means much of the risk is preventable.
It is worth keeping perspective. For the individual contact lens wearer the chance of ever getting Acanthamoeba keratitis is low, and good lens habits push it lower still. But because the disease can be so destructive when it does occur, and because the number of lens wearers is so large, it remains a serious and worthwhile target for prevention.
9. Prevention
The good news running through this entire topic is that the most common and most preventable form — keratitis — is largely under your own control. The single most important rule is captured in the simple public-health message: keep water away from your contact lenses.
For contact lens wearers, that means: never rinse or store your lenses in tap water (or any other water); use only fresh, proper contact lens disinfecting solution, never “topped up” old solution; remove your lenses before swimming, before using a hot tub, before showering, and before sleeping; replace your lens case regularly (every few months) and let it air-dry face-down between uses; and wash and dry your hands before handling lenses. Daily disposable lenses, which are thrown away after one use, avoid the storage-case reservoir altogether.
For the severe forms — brain and skin disease — prevention centers on protecting people who are immunocompromised. Those with weakened immune systems (from HIV/AIDS, transplant medication, chemotherapy, and similar conditions) benefit from reducing heavy exposure to soil and untreated water, promptly cleaning and covering skin wounds, and seeking medical attention early for unexplained skin nodules, persistent headaches, or neurological changes, since early recognition is one of the few advantages available against these hard-to-treat infections.
Key Research Papers
Peer-reviewed studies and authoritative reviews on Acanthamoeba — its biology and cyst resistance, the three diseases it causes, the contact-lens risk factors and recent UK outbreak, and the drug regimens used against it. Each citation links to the full text via DOI.
- Marciano-Cabral F, Cabral G. Acanthamoeba spp. as Agents of Disease in Humans. Clinical Microbiology Reviews. 2003;16(2):273–307.
- Khan NA. Acanthamoeba: Biology and Increasing Importance in Human Health. FEMS Microbiology Reviews. 2006;30(4):564–595.
- Visvesvara GS, Moura H, Schuster FL. Pathogenic and Opportunistic Free-Living Amoebae: Acanthamoeba spp., Balamuthia mandrillaris, Naegleria fowleri, and Sappinia diploidea. FEMS Immunology & Medical Microbiology. 2007;50(1):1–26.
- Lorenzo-Morales J, Khan NA, Walochnik J. An Update on Acanthamoeba Keratitis: Diagnosis, Pathogenesis and Treatment. Parasite. 2015;22:10.
- Carnt N, Hoffman JJ, Verma S, et al. Acanthamoeba Keratitis: Confirmation of the UK Outbreak and a Prospective Case-Control Study Identifying Contributing Risk Factors. British Journal of Ophthalmology. 2018;102(12):1621–1628.
- Radford CF, Bacon AS, Dart JKG, Minassian DC. Risk Factors for Acanthamoeba Keratitis in Contact Lens Users: A Case-Control Study. BMJ. 1995;310(6994):1567–1570.
- Stehr-Green JK, Bailey TM, Visvesvara GS. The Epidemiology of Acanthamoeba Keratitis in the United States. American Journal of Ophthalmology. 1989;107(4):331–336.
- Stehr-Green JK, Bailey TM, Brandt FH, Carr JH, Bond WW, Visvesvara GS. Acanthamoeba Keratitis in Soft Contact Lens Wearers: A Case-Control Study. JAMA. 1987;258(1):57–60.
- Lim N, Goh D, Bunce C, et al. Comparison of Polyhexamethylene Biguanide and Chlorhexidine as Monotherapy Agents in the Treatment of Acanthamoeba Keratitis. American Journal of Ophthalmology. 2008;145(1):130–135.
- Kalra SK, Sharma P, Shyam K, Tejan N, Ghoshal U. Acanthamoeba and Its Pathogenic Role in Granulomatous Amebic Encephalitis. Experimental Parasitology. 2020;208:107788.
- Parija SC, Dinoop K, Venugopal H. Management of Granulomatous Amebic Encephalitis: Laboratory Diagnosis and Treatment. Tropical Parasitology. 2015;5(1):23–28.
- Seal D, Hay J, Kirkness C. Chlorhexidine or Polyhexamethylene Biguanide for Acanthamoeba Keratitis. The Lancet. 1995;345(8942):136.
Live PubMed Searches
Each link opens a live PubMed query so results stay current as new papers are indexed.
- Acanthamoeba biology review
- Acanthamoeba keratitis contact lens
- Acanthamoeba keratitis treatment
- Granulomatous amebic encephalitis
- Acanthamoeba cyst resistance
- Acanthamoeba cutaneous infection
- Acanthamoeba Legionella host
- Acanthaporin pore-forming toxin
- Acanthamoeba keratitis epidemiology
- Naegleria fowleri PAM comparison
Connections
- All Parasites
- Symptoms & Diagnosis
- Acanthamoeba Keratitis
- Granulomatous Amebic Encephalitis
- Cutaneous & Disseminated Infection
- Treatment Overview
- Conventional Treatment
- Ivermectin
- Castor Oil
- All Conditions
- Ophthalmology
- Dry Eye Disease
- Meningitis
- Escherichia coli
- Castor Oil Remedy