Stomach Cancer
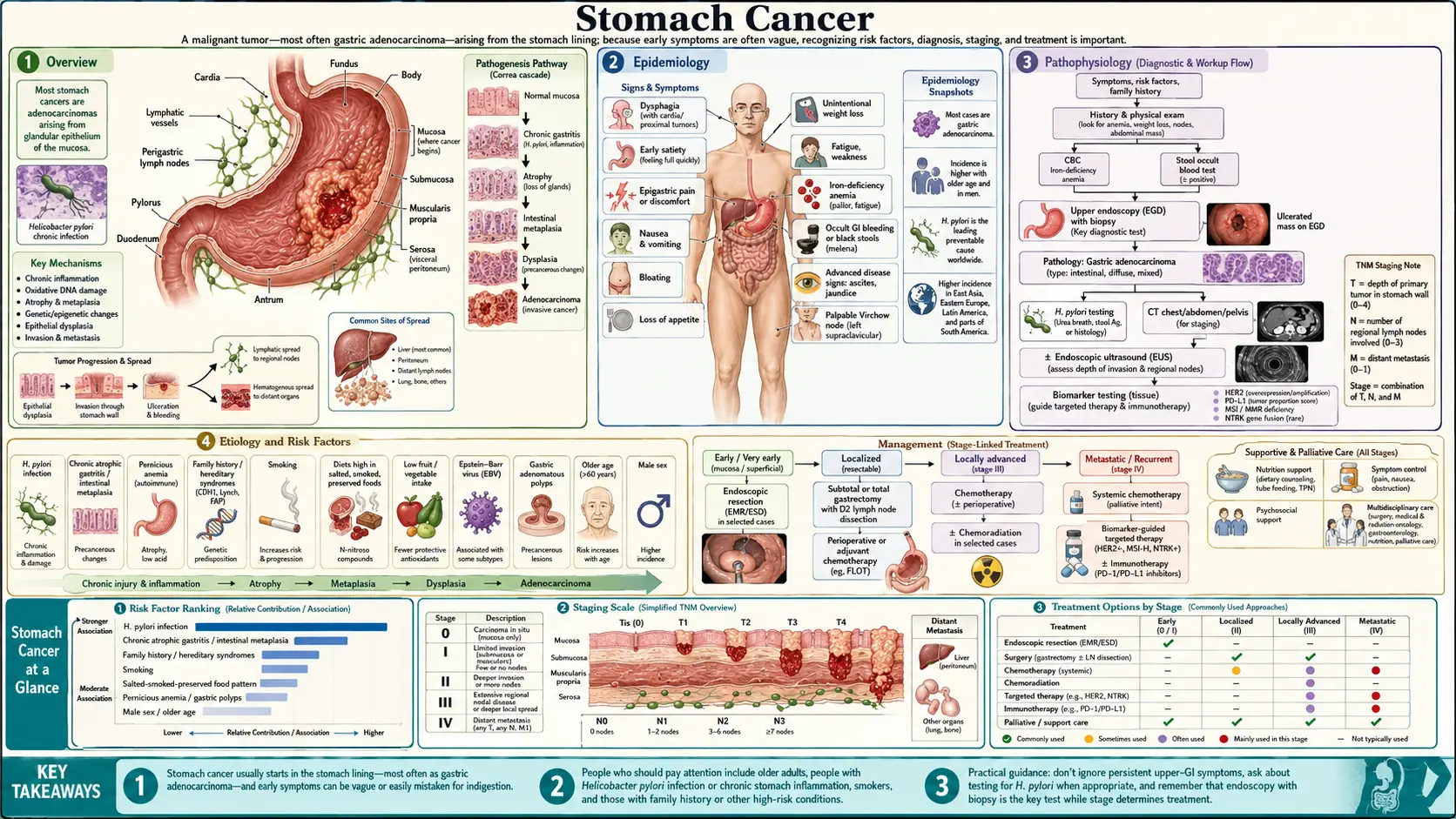
Table of Contents
- Overview
- Epidemiology
- Pathophysiology
- Etiology and Risk Factors
- Clinical Presentation
- Diagnosis
- Treatment
- Complications
- Prognosis
- Prevention
- Recent Research and Advances
- Research Papers
- Connections
- Featured Videos
1. Overview
Stomach cancer — also called gastric cancer — is a malignancy that begins in the lining of the stomach, the muscular pouch that holds and breaks down the food you eat. The great majority of cases (about 90–95%) are adenocarcinomas, meaning they start in the mucus-producing gland cells of the stomach wall. The rest are rarer types: lymphomas (often linked to the same bacterium that drives adenocarcinoma), gastrointestinal stromal tumors (GISTs), and neuroendocrine tumors. This page focuses on gastric adenocarcinoma, the form most people mean when they say "stomach cancer."
Here is the single most important thing to know, and the reason this disease is so different from most cancers: stomach cancer is, for the most part, an infectious disease with a long fuse. A common stomach bacterium called Helicobacter pylori (H. pylori) is responsible for the large majority of cases worldwide. The World Health Organization's cancer agency (IARC) classifies H. pylori as a Group 1 carcinogen — the same definitive-cause category as tobacco smoke and asbestos. It takes decades of low-grade inflammation to turn a healthy stomach lining into cancer, which means there is a long window in which a simple test and a one-week course of antibiotics can stop the process. Most people never get tested. That is the tragedy and the opportunity at the heart of this disease.
The other thing worth understanding early is where the cancer sits. Tumors near the top of the stomach where it meets the esophagus (the cardia) behave more like esophageal cancer and are tied to reflux and obesity. Tumors in the body and lower stomach (non-cardia) are the classic H. pylori–driven kind. Most of the prevention story on this page is about non-cardia cancer, which is the type that has been falling for a century and the type you can most directly protect yourself against.
2. Epidemiology
Worldwide, stomach cancer is the fifth most common cancer and one of the leading causes of cancer death, with roughly one million new cases and about 770,000 deaths each year (GLOBOCAN 2020). But the burden is wildly uneven across the globe. More than half of all cases occur in East Asia — Japan, Korea, China, and Mongolia have the highest rates on Earth — with additional hotspots in Eastern Europe and parts of Central and South America. Sub-Saharan Africa and North America have comparatively low rates.
In the United States, stomach cancer is now relatively uncommon: roughly 26,000–27,000 new cases and about 11,000 deaths a year. Within the US it is not evenly distributed — incidence is two to three times higher in Hispanic, Black, Asian/Pacific Islander, and Native American populations than in non-Hispanic white populations, largely tracking rates of H. pylori infection in countries of origin.
The long-term American trend is one of medicine's great unplanned victories. In 1930, stomach cancer was the number-one cause of cancer death in the United States, killing more men than any other malignancy. Over the following decades its incidence fell by roughly 90%. No screening program or drug did this. The leading explanation is the spread of refrigeration, which replaced salt-curing and smoking as the main way to preserve food and also made fresh fruit and vegetables available year-round, alongside falling rates of childhood H. pylori infection as sanitation improved. The disease quietly retreated as the conditions that fed it disappeared.
A few patterns are worth knowing. Stomach cancer is roughly twice as common in men as in women, and the average age at diagnosis in the US is around 68, so it is mostly a disease of later life — though the diffuse type can strike adults in their 30s and 40s, especially in hereditary families. The two anatomical subtypes are also moving in opposite directions: classic non-cardia cancer (lower stomach, H. pylori–driven) has fallen steadily, while cardia cancer (at the junction with the esophagus, tied to reflux and obesity) has held steady or risen in some Western countries — a reminder that the two halves of "stomach cancer" have different causes and different futures.
3. Pathophysiology
Most stomach cancers do not appear overnight. They develop through a slow, stepwise deterioration of the stomach lining first mapped out by the pathologist Pelayo Correa in the 1970s and 80s. This sequence — the Correa cascade — is the backbone of how we understand and prevent gastric cancer. Walking through it explains exactly where intervention works:
- Normal mucosa. A healthy stomach lining.
- Chronic gastritis. H. pylori colonizes the stomach and triggers persistent, low-grade inflammation that can smolder for years or decades without symptoms.
- Atrophic gastritis. Ongoing inflammation gradually destroys the normal acid- and enzyme-producing glands. The lining thins and acid output drops.
- Intestinal metaplasia. The damaged stomach lining is replaced by cells that resemble intestinal tissue — a kind of cellular "repair gone wrong." This is a marker that the stomach has been chronically injured.
- Dysplasia. Cells become genuinely abnormal and disorganized. This is the immediate pre-cancer stage.
- Invasive carcinoma. Abnormal cells break through the lining and become cancer.
The crucial point for patients is the timeline: this cascade typically unfolds over 20 to 40 years. That long runway is precisely why prevention works. Eradicate the bacterium early (steps 2–3) and the process can be halted or reversed before metaplasia sets in. Even at the metaplasia stage, eradication slows further progression, and the abnormal lining can be watched with periodic endoscopy. Few cancers give you decades of warning. Stomach cancer does — but only if someone is looking.
At the tissue level, pathologists also sort gastric adenocarcinoma into two classic patterns described by the Finnish pathologist Pekka Lauren in 1965:
- Intestinal type. Cells form recognizable gland-like structures. This is the type that follows the Correa cascade most faithfully, is more common in older patients and high-incidence regions, and is the type whose rates have fallen with declining H. pylori infection.
- Diffuse type. Cells spread through the stomach wall as scattered, poorly cohesive cells — including the distinctive signet-ring cell, whose nucleus is shoved to one side by a balloon of mucus. Diffuse cancer can thicken and stiffen the whole stomach (a pattern called linitis plastica, or "leather bottle stomach"), tends to strike younger patients, is less clearly linked to diet, and carries the worst prognosis. The inherited form (CDH1) is almost always diffuse type.
4. Etiology and Risk Factors
Helicobacter pylori — the leading cause
If you remember one thing from this page, make it this: H. pylori is the single largest cause of stomach cancer. Population studies attribute roughly 75–90% of all non-cardia gastric cancers to chronic H. pylori infection. Two landmark 1991 studies — Parsonnet and colleagues in a California cohort, and Nomura and colleagues among Japanese-American men in Hawaii — independently showed that people infected with H. pylori had several-fold higher odds of later developing stomach cancer, establishing the link that earned the bacterium its Group 1 carcinogen designation.
H. pylori is one of the most common chronic infections on Earth, carried by perhaps half of all humans. Most people who carry it never get sick. The bacterium causes harm in a minority — but because so many people are infected, that minority adds up to most of the world's stomach cancer. The cancer risk is highest with more virulent bacterial strains (those carrying the cagA gene) and when infection is acquired in early childhood, giving it the longest time to drive the Correa cascade.
The practical takeaway is hopeful: this is a treatable, curable infection. A simple stool antigen test or urea breath test detects it, and a 10–14 day course of antibiotics plus an acid-blocking drug clears it in most people. We will return to what eradication does to cancer risk in the Prevention section — the numbers are striking.
Diet and lifestyle
- Salt and salt-preserved foods. Diets heavy in salted, smoked, pickled, and cured foods are consistently tied to higher gastric cancer risk. High salt damages the stomach lining directly and appears to make it more vulnerable to H. pylori. This dietary shift away from salt-curing is the leading theory for the century-long decline in US cases.
- Low fruit and vegetable intake. Diets rich in fresh fruit and vegetables are associated with lower risk, likely through antioxidants and vitamin C that buffer the stomach against carcinogenic byproducts.
- Processed and red meats; nitrites. Cured meats and other sources of nitrites/nitrosamines have been linked to higher risk in several studies.
- Smoking. Tobacco roughly doubles the risk of gastric cancer and is a well-established cause — especially for cancers near the top of the stomach.
- Alcohol and obesity. Heavy alcohol use is a probable contributor; obesity and reflux are tied specifically to cardia (upper-stomach) cancers.
Medical conditions and genetics
- Pernicious anemia / autoimmune gastritis. When the immune system attacks the stomach's acid-producing cells, the resulting atrophic gastritis raises gastric cancer risk and also causes vitamin B12 deficiency. People with this condition warrant endoscopic surveillance.
- Epstein–Barr virus (EBV). A distinct subset — about 9% of gastric cancers worldwide (Murphy 2009) — carry EBV inside the tumor cells. These EBV-positive cancers have unique molecular features and a somewhat better prognosis, and represent one of the four molecular classes defined by The Cancer Genome Atlas.
- Family history and hereditary syndromes. Having a first-degree relative with stomach cancer roughly doubles to triples your own risk. A small fraction of cases are due to inherited syndromes — most importantly hereditary diffuse gastric cancer (HDGC), caused by mutations in the CDH1 gene. People in CDH1 families face a very high lifetime risk of aggressive diffuse-type cancer that is nearly invisible on standard endoscopy, so guidelines often recommend prophylactic (preventive) total gastrectomy — removing the entire stomach before cancer can take hold. Lynch syndrome and a few other syndromes also raise gastric risk.
- Prior gastric surgery and chronic gastric ulcers. The stump of a stomach after partial removal, and longstanding inflammation, can raise long-term risk.
5. Clinical Presentation
The cruel feature of stomach cancer is that its early symptoms are vague and ordinary — exactly the kind of "indigestion" that millions of people have and shrug off. There is no early warning that feels alarming. Common early complaints include:
- Persistent indigestion, heartburn, or a burning ache in the upper belly
- Feeling full after only a few bites (early satiety)
- Mild nausea or loss of appetite
- Bloating after meals
By the time more obvious symptoms appear, the cancer is often advanced: unintended weight loss, vomiting (sometimes of blood, which looks like coffee grounds), black tarry stools from internal bleeding, iron-deficiency anemia (showing up as fatigue and pallor), difficulty swallowing if the tumor is near the top of the stomach, and a feeling of fullness or a mass in the upper abdomen.
Alarm symptoms — when to get an endoscopy now
This is the most actionable part of the page. Most indigestion is harmless, but certain "alarm features" mean you should be referred for an upper endoscopy promptly rather than just being handed an acid blocker:
- New indigestion or dyspepsia starting after age 55–60
- Unintended weight loss
- Early satiety — getting full unusually fast
- Iron-deficiency anemia or any sign of GI bleeding (black stools, vomiting blood)
- Difficulty or pain swallowing (dysphagia)
- Persistent vomiting
- A family history of stomach cancer plus new upper-GI symptoms
If you have any of these, do not let "it's probably just acid reflux" be the end of the conversation. Ask specifically about an endoscopy. The whole survival gap between the US and Asia (below) comes down to whether the cancer is found at this stage or much later.
6. Diagnosis
Upper endoscopy (EGD) with biopsy is the cornerstone. A thin flexible camera is passed through the mouth into the stomach; the doctor inspects the lining directly and takes tissue samples of anything suspicious. Biopsy under the microscope confirms cancer, identifies the Lauren type, and tests for biomarkers (HER2, the protein PD-L1, the Claudin-18.2 marker, and EBV) that determine which modern drugs may work. The same endoscopy tests for H. pylori.
Once cancer is confirmed, staging determines how far it has spread and therefore how it is treated:
- CT scan of the chest, abdomen, and pelvis to look for spread to lymph nodes, liver, or beyond.
- Endoscopic ultrasound (EUS), which puts an ultrasound probe right next to the tumor to measure how deeply it invades the stomach wall (the "T" stage) and check nearby nodes — critical for deciding whether an early tumor can be removed endoscopically.
- Staging laparoscopy, a keyhole look inside the abdomen with washings, to catch tiny seeds of cancer on the peritoneum (the abdominal lining) that scans miss. This commonly changes the plan and spares some patients an operation that would not help.
- PET-CT in selected cases.
Why US cases are caught late — an honest systems comparison
Japan and Korea have so much stomach cancer that they run national endoscopic (and, historically, barium) screening programs, inviting adults over 40–50 for regular checks. As a result they find a large share of cancers while still confined to the stomach lining and curable. Their overall five-year survival is roughly 60–70%.
The United States has no such program, and for a defensible reason: stomach cancer is now rare enough here that mass screening of the whole population would not pay off. The downside is that American cancers are usually found late, prompted only by alarm symptoms, when survival is poor. The honest conclusion is not "the US is doing it wrong" but that the strategy that fits a country depends on how common the disease is. For higher-risk individuals in the US — by family history or ethnic background — the lesson is to be screened or tested individually rather than waiting for a national program that, for a rare disease, may never come.
7. Treatment
Treatment depends almost entirely on stage, and the field has changed dramatically in the past 15 years. Decisions are made by a multidisciplinary team.
Very early disease — endoscopic removal
When cancer is caught confined to the most superficial layer of the lining, it can often be cured without major surgery using endoscopic submucosal dissection (ESD) — peeling the cancerous patch off the stomach wall through the endoscope, leaving the stomach intact. This is routine in Asia precisely because screening finds cancers this early, and it is increasingly used in Western centers for suitable early tumors.
Localized but invasive disease — surgery plus chemotherapy
For cancers that have grown into the stomach wall but not spread distantly, the goal is cure through surgery — partial or total gastrectomy with a thorough lymph-node removal known as a D2 lymphadenectomy, the standard pioneered in Asia and now adopted worldwide.
Surgery is paired with chemotherapy given before and after the operation (perioperative chemotherapy). The current standard regimen in Europe and increasingly the US is FLOT (fluorouracil, leucovorin, oxaliplatin, docetaxel). The FLOT4 trial (Al-Batran 2019) showed FLOT improved median overall survival to about 50 months versus 35 months with the older ECF/ECX regimen — a meaningful gain that established FLOT as the new benchmark. Earlier trials such as MAGIC (perioperative ECF) and the REAL-2 study of oxaliplatin/capecitabine combinations (Cunningham 2008) built the foundation.
Advanced and metastatic disease — chemotherapy plus targeted and immune drugs
When cancer has spread, treatment aims to control it and extend good-quality life. Biomarker testing now steers therapy:
- HER2-positive cancer (~15–20%): adding the antibody trastuzumab to chemotherapy improved survival in the landmark ToGA trial (Bang 2010), the first targeted therapy proven to work in gastric cancer.
- Immunotherapy: the checkpoint inhibitor nivolumab added to chemotherapy improved survival in the CheckMate-649 trial (Janjigian 2021), and is now a first-line standard, especially for tumors expressing PD-L1.
- Claudin-18.2–positive cancer: the newer antibody zolbetuximab, which targets the Claudin-18.2 protein on tumor cells, improved survival when added to chemotherapy in the SPOTLIGHT trial (Shitara 2023) — opening a fresh treatment avenue for roughly a third of patients whose tumors carry this marker.
Radiation therapy has a role in some localized cases and for relieving symptoms such as bleeding or obstruction. Palliative care, started early, helps with pain, nutrition, and quality of life regardless of stage.
What "biomarker testing" actually means for you
It is worth pausing on this, because it is where modern stomach-cancer treatment differs most from the past. Twenty years ago, almost everyone with advanced gastric cancer got the same chemotherapy. Today, a few protein and gene tests run on your biopsy decide which extra drug — if any — gets added, and those additions can change survival by months. The four tests that matter most are HER2 (which opens the door to trastuzumab), PD-L1 (which predicts benefit from immunotherapy like nivolumab), Claudin-18.2 (the target of zolbetuximab), and microsatellite instability / mismatch-repair status (a marker of tumors that respond especially well to immunotherapy). If you or a family member is being treated for advanced stomach cancer, it is entirely reasonable to ask the oncologist, "Has my tumor been tested for HER2, PD-L1, Claudin-18.2, and MSI?" These tests are standard of care, but in a busy system it is fair to confirm they were done — they determine whether the newest, most effective drugs are even on the table.
8. Complications
Complications arise both from the cancer and from its treatment. From the disease: bleeding, blockage at the stomach inlet or outlet, perforation, malnutrition, and spread to the liver, peritoneum (causing fluid buildup, or ascites), and beyond.
Life after gastrectomy — the practical reality
Removing part or all of the stomach changes eating permanently, and patients deserve straight talk about it. The good news is that people adapt and live full lives; the honest news is that it takes adjustment. Common, manageable challenges:
- Small, frequent meals. Without a full-sized reservoir, you eat little and often — typically six or more small meals a day rather than three big ones.
- Dumping syndrome. Food, especially sugary food, can rush too fast into the intestine, causing cramping, sweating, racing heart, and diarrhea soon after eating, or shakiness an hour or two later. Eating smaller portions, limiting simple sugars, and separating drinks from meals usually controls it.
- Vitamin B12 — for life. The stomach makes a protein (intrinsic factor) needed to absorb vitamin B12. After total gastrectomy you can no longer absorb it from food, so you need B12 injections (or high-dose supplements) permanently. Skipping this leads to anemia and nerve damage over time.
- Iron and calcium. Absorption of iron and calcium drops, so iron-deficiency anemia and bone thinning are common and need monitoring and supplementation.
- Weight and nutrition. Weight loss is expected; a dietitian is part of the recovery team, not an optional extra.
9. Prognosis
Survival depends overwhelmingly on stage at diagnosis — and this is where the late-detection problem in the US shows up in the numbers. Honest figures:
- Overall US five-year relative survival: about 36%. Roughly one in three.
- Localized disease (still confined to the stomach): about 75%. Three in four.
- Spread to regional lymph nodes: roughly 35%.
- Distant metastatic disease: about 7%.
The contrast with Japan and Korea — overall survival of 60–70% — is almost entirely explained by stage at diagnosis, not by better surgeons or drugs. Their screening programs find the cancer when it is localized and survival is high; the US tends to find it late, when survival is low. The number that matters is the difference between 75% (localized) and 7% (distant). Everything in prevention and early detection is aimed at moving patients from the second number to the first.
10. Prevention
Stomach cancer is one of the most preventable of all cancers, because its main cause is a treatable infection acting over decades.
H. pylori "test and treat" — the centerpiece
Finding and eradicating H. pylori is the most powerful single thing that lowers gastric cancer risk. The evidence is strong and consistent:
- A meta-analysis of randomized trials found that eradicating H. pylori reduced the risk of developing gastric cancer by roughly 46% in treated people compared with placebo.
- The Choi NEJM 2020 Korean trial studied people at especially high risk — those with a first-degree relative who had stomach cancer. Eradicating H. pylori cut their risk of gastric cancer by more than half over the following years, and the benefit was greatest in those whose bacterium was successfully cleared. This is the kind of family in which "ask your doctor to test you" is concrete, actionable advice.
- The Fukase 2008 Lancet trial showed that in patients who had already had an early gastric cancer removed endoscopically, eradicating H. pylori cut the rate of a new (metachronous) cancer roughly threefold.
Who should consider getting tested? Anyone with a family history of stomach cancer, people from regions or ethnic backgrounds with higher incidence, those with peptic ulcers or chronic dyspepsia, and anyone found to have gastric atrophy or intestinal metaplasia. The test is cheap and noninvasive — a stool antigen test or a urea breath test — and treatment is a one-to-two-week course of pills. Because myhealthcare.com covers the bacterium itself in depth, you can read more on the dedicated Helicobacter pylori page.
Diet and lifestyle
- Eat more fruit and vegetables. A diet rich in fresh produce is consistently linked to lower risk.
- Cut back on salt-preserved, smoked, and pickled foods, and on processed meats. Refrigeration did this for the population a century ago; you can do it for yourself.
- Don't smoke. Smoking roughly doubles risk, and quitting lowers it over time.
- Moderate alcohol and maintain a healthy weight, which especially protects against upper-stomach (cardia) cancer.
For higher-risk individuals — people with atrophic gastritis, intestinal metaplasia, pernicious anemia, prior gastric cancer, or strong family history — periodic endoscopic surveillance catches problems early while they are still curable. And for the rare families with a CDH1 mutation, preventive total gastrectomy is a drastic but life-saving option discussed with a genetics and surgical team.
A realistic personal checklist
Prevention can feel abstract, so here is what it looks like in practice for an ordinary person:
- Know your family history. If a parent, sibling, or child had stomach cancer, mention it to your doctor and ask about H. pylori testing — this is exactly the group the Choi 2020 trial showed benefits most.
- Don't ignore persistent indigestion, especially if it is new after your mid-50s or comes with weight loss, early fullness, anemia, or trouble swallowing. Ask whether an endoscopy is warranted rather than accepting open-ended acid blockers.
- If you test positive for H. pylori, finish the full treatment and confirm it cleared with a follow-up breath or stool test. Eradication only protects you if the bacterium is actually gone.
- Shift your plate toward fresh fruit and vegetables and away from heavily salted, smoked, pickled, and processed-meat foods.
- Don't smoke.
None of this requires a screening program or a specialist. It is the kind of low-cost, high-leverage prevention that fits a disease with a decades-long fuse.
11. Recent Research and Advances
Stomach cancer research is moving on several fronts at once. The most exciting development of the past decade is molecular subtyping: The Cancer Genome Atlas (2014) sorted gastric cancer into four genomic classes — EBV-positive, microsatellite-unstable, chromosomally unstable, and genomically stable — each with distinct biology and treatment implications. This framework is steadily turning "stomach cancer" from one disease into several, each with its own targeted strategy.
In the clinic, the run of positive trials — ToGA (trastuzumab), CheckMate-649 (nivolumab immunotherapy), and SPOTLIGHT (zolbetuximab against Claudin-18.2) — means more patients now receive a treatment matched to a specific marker in their tumor. Antibody-drug conjugates and next-generation immunotherapy combinations are in active testing. On the prevention side, the durable results of H. pylori eradication trials, especially the family-history data, are pushing professional societies toward broader "test and treat" recommendations in higher-risk groups. Blood-based "liquid biopsy" tests that detect tumor DNA are being studied for earlier detection and for monitoring response, which could one day narrow the survival gap that screening programs created.
12. References & Research
Historical Background
Stomach cancer's history is a story of two discoveries that changed everything. The first was accidental and population-wide: in 1930, gastric cancer was the leading cause of cancer death in the United States, yet over the next several decades its incidence fell by roughly 90% — a decline now credited largely to refrigeration replacing salt-curing and smoking, and to year-round access to fresh produce. Nobody set out to prevent stomach cancer; an appliance did it. The second discovery was deliberate and Nobel-worthy. In 1984, Australian physicians Barry Marshall and Robin Warren reported curved bacteria in the stomachs of patients with gastritis and ulcers, overturning the dogma that the stomach was too acidic for bacteria to survive. To prove the bug caused disease, Marshall famously drank a culture of H. pylori himself and developed gastritis. Their work — which won the 2005 Nobel Prize in Physiology or Medicine — recast peptic ulcers and most stomach cancer as infectious diseases. Alongside, pathologist Pelayo Correa published his stepwise "cascade" model of gastric carcinogenesis in 1975 and refined it through the 1980s and 1990s, giving clinicians the roadmap of intervention this page is built around.
Key Research Papers
- Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA: A Cancer Journal for Clinicians. 2021;71(3):209-249.
- Arnold M, Abnet CC, Neale RE, et al. Global Burden of 5 Major Types of Gastrointestinal Cancer. Gut. 2020;69(9):1564-1571.
- Marshall BJ, Warren JR. Unidentified Curved Bacilli in the Stomach of Patients with Gastritis and Peptic Ulceration. The Lancet. 1984;323(8390):1311-1315.
- Parsonnet J, Friedman GD, Vandersteen DP, et al. Helicobacter pylori Infection and the Risk of Gastric Carcinoma. New England Journal of Medicine. 1991;325(16):1127-1131.
- Nomura A, Stemmermann GN, Chyou PH, et al. Helicobacter pylori Infection and Gastric Carcinoma among Japanese Americans in Hawaii. New England Journal of Medicine. 1991;325(16):1132-1136.
- Correa P. A New Paradigm for Human Carcinogenesis: Gastric Cancer and the Correa Cascade. Journal of Clinical Gastroenterology. 2000;30(4):341-342.
- Leung WK, Lin SR, Ching JYL, et al. Factors Predicting Progression of Gastric Intestinal Metaplasia: Results of a Randomised Trial on Helicobacter pylori Eradication. Gut. 2004;53(9):1244-1249.
- Choi IJ, Kim CG, Lee JY, et al. Family History of Gastric Cancer and Helicobacter pylori Treatment. New England Journal of Medicine. 2020;382(5):427-436.
- Fukase K, Kato M, Kikuchi S, et al. Effect of Eradication of Helicobacter pylori on Incidence of Metachronous Gastric Carcinoma after Endoscopic Resection of Early Gastric Cancer: An Open-Label, Randomised Controlled Trial. The Lancet. 2008;372(9636):392-397.
- The Cancer Genome Atlas Research Network. Comprehensive Molecular Characterization of Gastric Adenocarcinoma. Nature. 2014;513(7517):202-209.
- Murphy G, Pfeiffer R, Camargo MC, Rabkin CS. Meta-analysis Shows That Prevalence of Epstein–Barr Virus-Positive Gastric Cancer Differs Based on Sex and Anatomic Location. Gastroenterology. 2009;137(3):824-833.
- Fitzgerald RC, Hardwick R, Huntsman D, et al. Hereditary Diffuse Gastric Cancer: Updated Consensus Guidelines for Clinical Management. Journal of Medical Genetics. 2010;47(7):436-444.
- Al-Batran SE, Homann N, Pauligk C, et al. Perioperative Chemotherapy with Fluorouracil plus Leucovorin, Oxaliplatin, and Docetaxel versus Fluorouracil or Capecitabine plus Cisplatin and Epirubicin for Locally Advanced Gastric or Gastro-oesophageal Junction Adenocarcinoma (FLOT4). The Lancet. 2019;393(10184):1948-1957.
- Bang YJ, Van Cutsem E, Feyereislova A, et al. Trastuzumab in Combination with Chemotherapy versus Chemotherapy Alone for Treatment of HER2-positive Advanced Gastric or Gastro-oesophageal Junction Cancer (ToGA). The Lancet. 2010;376(9742):687-697.
- Janjigian YY, Shitara K, Moehler M, et al. First-line Nivolumab plus Chemotherapy versus Chemotherapy Alone for Advanced Gastric, Gastro-oesophageal Junction, and Oesophageal Adenocarcinoma (CheckMate 649). The Lancet. 2021;398(10294):27-40.
- Shitara K, Lordick F, Bang YJ, et al. Zolbetuximab plus mFOLFOX6 in Patients with CLDN18.2-positive, HER2-negative, Untreated, Locally Advanced Unresectable or Metastatic Gastric or Gastro-oesophageal Junction Adenocarcinoma (SPOTLIGHT). The Lancet. 2023;401(10389):1655-1668.
Research Papers
The links below run live searches on PubMed, the US National Library of Medicine's database of biomedical literature. Use them to find the latest peer-reviewed research on stomach cancer and its prevention. Each opens in a new tab.
- Gastric cancer epidemiology
- H. pylori eradication and gastric cancer
- Correa cascade and gastric carcinogenesis
- Gastric intestinal metaplasia surveillance
- Hereditary diffuse gastric cancer (CDH1)
- Endoscopic submucosal dissection for gastric cancer
- FLOT perioperative chemotherapy
- Gastric cancer immunotherapy
- Claudin-18.2 and zolbetuximab
- Gastric cancer screening in Japan and Korea
- Epstein–Barr virus gastric carcinoma
- Nutrition after gastrectomy
Connections
- Cancer — Overview
- Metastatic Cancers
- Esophageal Cancer
- Helicobacter pylori
- Peptic Ulcer Disease
- Gastroesophageal Reflux Disease (GERD)
- Anemia
- Loss of Appetite
- Nausea and Vomiting
- Vitamin B12
- Broccoli
- Garlic
- Oncology
- All Conditions