Nasopharyngeal Cancer
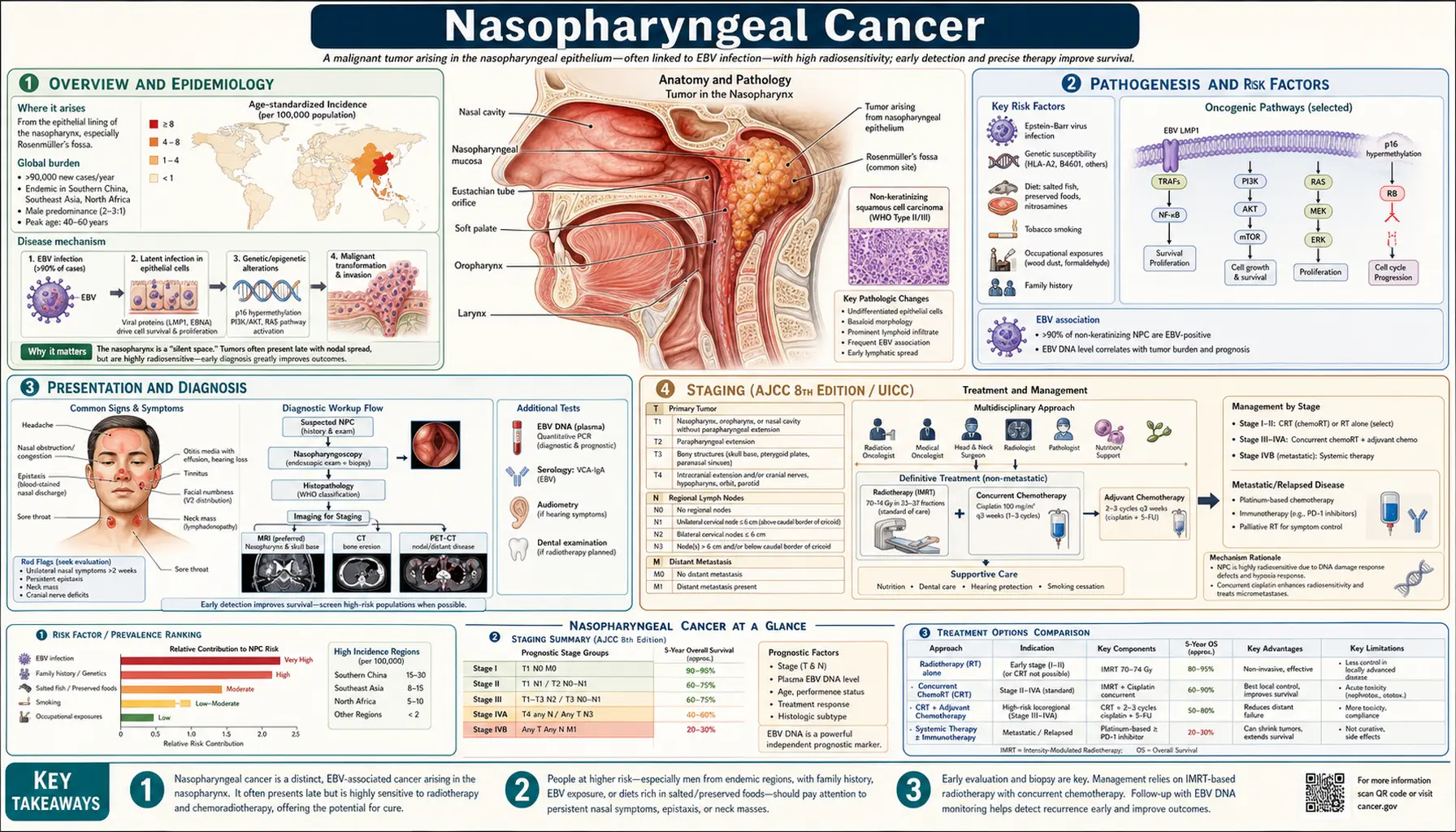
Table of Contents
- Overview and Epidemiology
- Pathogenesis and Risk Factors
- Presentation and Diagnosis
- Staging (AJCC 8th Edition)
- Treatment
- EBV DNA as Biomarker
- Long-Term Effects and Survivorship
- Surveillance and Screening
- Salvage Treatment for Recurrence
- Prevention
- Key Research Papers
- Featured Videos
Overview and Epidemiology
Nasopharyngeal carcinoma (NPC) is a cancer of the epithelial cells lining the nasopharynx — the upper part of the throat directly behind the nose, above the soft palate. Unlike most head and neck cancers that are tied to tobacco and alcohol use, NPC has a uniquely strong geographic and ethnic pattern driven by Epstein-Barr virus (EBV) and specific dietary and genetic factors.
Where it is common: NPC is one of the most geographically unequal cancers in the world. In Southern China — particularly Canton (Guangdong) Province and among Cantonese-speaking populations — incidence reaches 20 to 30 cases per 100,000 people per year. It is also elevated in Southeast Asia (Vietnam, Malaysia, Thailand, Philippines), North Africa (Morocco, Tunisia, Egypt), and among Alaska Native (Inuit) populations. In North America and Western Europe, NPC is rare: roughly 0.5 to 1 case per 100,000 per year. Importantly, Chinese immigrants to low-incidence countries maintain elevated risk for one to two generations, suggesting both genetic and dietary exposures from childhood matter.
WHO classification — three types: The World Health Organization divides NPC into three histological subtypes, and the type matters for prognosis and treatment response:
- Type I — Keratinizing squamous cell carcinoma: Most resembles typical head and neck squamous cancer. Associated with HPV in some endemic settings. Worst prognosis of the three types. Less sensitive to radiation and chemotherapy than Types II and III.
- Type II — Non-keratinizing differentiated carcinoma: Intermediate presentation. Strongly EBV-associated in endemic regions.
- Type III — Non-keratinizing undifferentiated carcinoma: The most common type in endemic regions (Southern China, Southeast Asia). Driven by EBV. Best response to concurrent chemoradiation — cure rates exceeding 80–90% for early-stage disease. Also called lymphoepithelioma in older literature.
Who gets it: NPC affects men approximately three times as often as women (M:F ratio 3:1). Age distribution is bimodal in endemic regions: a smaller peak in teenagers and young adults (15–25 years), then a larger peak in middle-aged adults (40–60 years). In non-endemic regions, most cases occur in adults over 50. Cantonese Chinese, whether living in China or abroad, carry the highest lifetime risk worldwide.
Pathogenesis and Risk Factors
NPC develops through a combination of viral, dietary, genetic, and environmental factors. Understanding how these interact explains why certain populations are so much more vulnerable than others.
Epstein-Barr Virus (EBV)
EBV is the central driver of Type II and Type III NPC. Nearly all undifferentiated NPC tumors carry EBV DNA within the cancer cells. The virus establishes a latency pattern called Latency Type II in NPC, expressing specific viral proteins and RNA molecules:
- EBER1 and EBER2: Small non-coding RNAs expressed at very high levels in latently infected cells. Their detection by in-situ hybridization is the gold standard for confirming EBV in tumor tissue.
- LMP1 (Latent Membrane Protein 1): The main viral oncogene in NPC. LMP1 mimics a constitutively active receptor and continuously activates three major cancer-driving pathways: NF-kB (promotes survival and anti-apoptosis), AP-1 (promotes invasion and growth), and JAK/STAT (promotes proliferation). LMP1 is arguably the primary reason EBV-driven NPC cells survive and multiply.
- LMP2A and LMP2B: LMP2A mimics B-cell receptor (BCR) signaling, helping infected cells survive without normal growth signals.
- EBNA1: Maintains the viral episome through cell division. EBNA1 has immune evasion properties — it resists proteasomal degradation, helping infected cells hide from cytotoxic T cells.
Despite EBV's central role, EBV infection alone is not sufficient — the vast majority of the world's population is infected with EBV (over 90%) yet NPC remains uncommon outside endemic regions. Additional genetic and environmental co-factors are required.
Dietary Factors
Salted fish is the most consistently documented dietary risk factor for NPC, particularly among Southern Chinese populations. Traditional Cantonese salted fish — preserved with large amounts of salt through bacterial fermentation — produces volatile nitrosamines during preparation and consumption. Nitrosamines are potent carcinogens. Epidemiological studies consistently show that childhood exposure to salted fish is the strongest dietary predictor of NPC in adulthood. The declining incidence of NPC in younger generations of Chinese diaspora communities, who eat less traditional preserved food, supports this association. Other nitrosamine-rich preserved foods (salted vegetables, fermented shrimp paste) carry related risks.
Genetic Susceptibility
Several genetic factors are known to modify NPC risk:
- HLA associations: Certain HLA alleles (antigen-presenting immune molecules) influence susceptibility. HLA-A2 appears protective in Chinese populations, while specific HLA-B and HLA-DR types confer higher risk.
- Chromosome 3p21 deletions: Loss of heterozygosity at chromosome 3p21 is one of the earliest and most consistent genetic events in NPC. This region contains tumor suppressor genes including RASSF1A, which is frequently silenced by methylation in NPC tumors.
- Familial clustering: First-degree relatives of NPC patients have a 4- to 10-fold elevated risk, even in low-incidence regions, pointing to shared genetic and environmental factors.
Other Risk Factors
- Occupational exposures: Formaldehyde and wood dust exposure are associated with modestly elevated NPC risk.
- Tobacco: Associated specifically with Type I (keratinizing) NPC; less clearly linked to Types II and III.
- HPV: Some Type I NPC tumors in endemic regions show HPV positivity (particularly HPV-16), similar to oropharyngeal cancer. HPV's role in NPC is smaller than EBV's overall.
Presentation and Diagnosis
NPC is particularly treacherous because the nasopharynx is anatomically hidden — tucked behind the nose and above the soft palate, it is not visible on routine oral examination. Symptoms are often subtle and easily attributed to more common conditions (ear infections, sinusitis, postnasal drip). As a result, most patients are diagnosed at Stage III or IV, when the cancer has already spread to lymph nodes or nearby structures.
Classic Presenting Symptoms
NPC presents with a characteristic triad of symptom clusters:
1. Neck mass (cervical lymphadenopathy): The single most common first symptom, present in approximately 80% of patients at diagnosis. The lymph nodes in the neck — particularly Levels II and III (upper and mid jugular chain) — enlarge as cancer spreads from the nasopharynx. Nodes can be massive (several centimeters), bilateral, and firm. Many patients first see their doctor for a "lump in the neck" with no other symptoms.
2. Nasal symptoms: Nosebleeds (epistaxis), nasal obstruction (one or both sides), and postnasal drip that does not respond to allergy or sinus treatment. Blood-tinged nasal discharge in a middle-aged person from a high-risk population should prompt urgent evaluation.
3. Ear symptoms: Unilateral serous otitis media — fluid behind the eardrum — caused by the tumor blocking the Eustachian tube, which connects the middle ear to the nasopharynx. This causes hearing loss, a feeling of ear fullness, and tinnitus on one side. Unilateral "glue ear" in an adult without a clear cause warrants nasopharyngoscopy.
Advanced Symptoms
When NPC invades surrounding structures, additional symptoms appear:
- Cranial nerve palsies: The skull base is immediately adjacent to the nasopharynx. Tumor invasion through the skull base can compress cranial nerves. The most common is CN VI (abducens nerve) — causing double vision (diplopia) from cavernous sinus involvement. CN V (trigeminal) involvement causes facial numbness or pain. CN IX, X, and XI compression at the jugular foramen causes difficulty swallowing, hoarse voice, and shoulder weakness. Multiple cranial nerve involvement is a red flag for skull base invasion.
- Trismus: Difficulty opening the mouth, caused by tumor invading the pterygoid muscles of the jaw.
- Headache: Often from skull base involvement or raised intracranial pressure.
Diagnostic Workup
When NPC is suspected, the following steps are taken:
- Nasopharyngoscopy with biopsy: Flexible endoscopy allows direct visualization of the nasopharynx and targeted biopsy of suspicious areas under topical anesthesia. This is the definitive diagnostic step — tissue diagnosis is required to confirm NPC and determine histological type.
- MRI of nasopharynx, skull base, and brain: MRI is superior to CT for evaluating soft tissue extent, parapharyngeal space involvement, skull base erosion, and intracranial extension. It is the primary imaging study for local staging.
- CT of chest, abdomen, and pelvis: To evaluate for distant metastases, particularly to lungs, liver, and bone.
- PET-CT scan: Highly sensitive for detecting nodal disease and distant metastases, especially bone involvement. PET-CT is increasingly standard for initial staging and post-treatment surveillance.
- Plasma EBV DNA (quantitative PCR): A blood test that measures circulating tumor DNA from EBV. Elevated pre-treatment EBV DNA is a powerful independent prognostic factor. Clearance to undetectable after treatment signals complete response. This test is central to NPC management in ways that have no parallel in most other cancers.
- Bone marrow biopsy: Occasionally performed if there is suspected bone marrow involvement.
Staging (AJCC 8th Edition / UICC)
NPC is staged using the American Joint Committee on Cancer (AJCC) 8th Edition system, which defines the extent of the primary tumor (T), lymph nodes (N), and distant spread (M). The staging system was updated in 2017 specifically to reflect modern imaging and outcomes data for NPC.
T Stage — Primary Tumor
- T1: Tumor confined to the nasopharynx, or extends into the oropharynx and/or nasal cavity, without parapharyngeal space involvement.
- T2: Tumor extends into the parapharyngeal space and/or adjacent soft tissues (medial pterygoid, lateral pterygoid, prevertebral muscles).
- T3: Tumor invades bony skull base, cervical vertebrae, pterygoid structures, or paranasal sinuses.
- T4: Tumor invades the intracranial compartment, cranial nerves, hypopharynx, orbit, or masticator space with lateral pterygoid involvement.
N Stage — Regional Lymph Nodes
- N0: No regional lymph node involvement.
- N1: Unilateral cervical nodes and/or unilateral or bilateral retropharyngeal nodes, 6 cm or smaller, above the caudal border of the cricoid cartilage.
- N2: Bilateral cervical nodes, 6 cm or smaller, above the caudal border of the cricoid cartilage.
- N3: Cervical nodes larger than 6 cm, or nodes below the caudal border of the cricoid cartilage (supraclavicular fossa).
M Stage and Overall Stage
M0 means no distant metastasis; M1 means distant metastasis is present (most commonly to bone, lungs, and liver).
Overall stage groupings and approximate 5-year overall survival (OS):
- Stage I (T1 N0 M0): ~90% 5-year OS. Rare at diagnosis outside screening programs.
- Stage II (T2 N0-1 or T1 N1): ~80% 5-year OS.
- Stage III (T3 or N2): ~60–70% 5-year OS.
- Stage IVA–IVB (T4 or N3): ~40–50% 5-year OS with modern chemoradiation.
- Stage IVC (M1): Metastatic disease; median survival approximately 2–3 years with systemic therapy.
The unfortunate reality is that most patients are diagnosed at Stage III or IV because early NPC produces few symptoms. In high-incidence regions with active screening programs (particularly Hong Kong), a much higher proportion of patients are diagnosed at early stages, with dramatically better outcomes.
Treatment
NPC is one of the most treatable head and neck cancers when caught early or at locoregional stage. Unlike many solid tumors, even Stage III NPC can be cured in the majority of patients using radiation combined with chemotherapy — a testament to the radiosensitivity of EBV-driven undifferentiated NPC (Type III).
Concurrent Chemoradiation (Standard of Care for Stage II–IVB)
The backbone of NPC treatment is intensity-modulated radiotherapy (IMRT) delivered concurrently with platinum-based chemotherapy.
Radiation: IMRT is the modern standard, replacing older 2D and 3D conformal techniques. IMRT sculpts the radiation dose precisely around the tumor while minimizing dose to nearby critical structures (parotid glands for saliva production, brainstem, cochlea for hearing, optic nerves). Typical doses are:
- 70 Gy to the primary tumor and involved lymph nodes (in 33–35 fractions over 7 weeks)
- 54–60 Gy to elective nodal regions (nodes at risk but not visibly involved)
- Brainstem maximum dose constrained to 54 Gy; cochlear dose limited where possible to reduce hearing loss
Concurrent cisplatin: Cisplatin is given during radiotherapy as a radiosensitizer — it makes cancer cells more vulnerable to radiation damage. Standard dosing is either 100 mg/m² every 3 weeks (three cycles during RT) or 40 mg/m² weekly. The landmark INT 0099 trial (Al-Sarraf et al., 1998) established that concurrent cisplatin + RT followed by adjuvant cisplatin + 5-FU was superior to RT alone, with dramatically improved 3-year progression-free and overall survival (PMID 9440738).
Induction Chemotherapy Before Chemoradiation
For locally advanced disease (Stage III–IVB), adding induction chemotherapy before concurrent chemoRT has become standard practice in China and Asia-Pacific and is increasingly used elsewhere.
Gemcitabine + Cisplatin (GP) induction: The landmark phase III trial by Zhang et al. (2019, New England Journal of Medicine) randomly assigned 480 patients with Stage III–IVB NPC to GP induction (3 cycles) followed by concurrent chemoRT, versus concurrent chemoRT alone. Induction GP significantly improved 3-year failure-free survival (85.3% vs 76.5%; hazard ratio 0.51; p < 0.001; Search PubMed). This trial is now widely cited as practice-changing.
Adjuvant Chemotherapy
The original INT 0099 protocol included adjuvant cisplatin + 5-FU after concurrent chemoRT, and many guidelines continue to recommend it for high-risk patients. Whether adjuvant chemo adds benefit after induction + chemoRT remains an active research question. The MAC-NPC meta-analysis (pooled individual patient data from multiple trials) confirmed that adding chemotherapy to RT improves overall survival, with the greatest absolute benefit from concurrent chemotherapy.
Recurrent and Metastatic NPC
When NPC returns after initial treatment or has spread to distant sites, treatment shifts to systemic chemotherapy and, increasingly, immunotherapy.
Gemcitabine + Cisplatin (GC) — first-line for recurrent/metastatic: The phase III trial by Zhang et al. (2016, New England Journal of Medicine) showed that GC was significantly superior to the older 5-FU + cisplatin regimen as first-line treatment for recurrent or metastatic NPC: median overall survival 29.1 months vs 20.9 months (hazard ratio 0.62; p = 0.001; Search PubMed). GC is now the accepted first-line standard worldwide for R/M NPC.
Immunotherapy (checkpoint inhibitors): PD-1/PD-L1 inhibitors have shown significant activity in NPC, which is logical given the heavy EBV-driven immune environment in these tumors.
- CameL trial: Camrelizumab (a PD-1 inhibitor approved in China) plus GC chemotherapy significantly improved progression-free survival versus GC alone in first-line R/M NPC. This combination has become standard in China.
- Pembrolizumab and nivolumab are being evaluated in ongoing trials. Early data show meaningful response rates in previously treated NPC.
EBV-specific T-cell therapy (emerging): Because NPC tumor cells express EBV antigens (LMP1, LMP2), they are potentially targetable by T cells that recognize these proteins. Adoptive T-cell therapies using EBV-specific cytotoxic T lymphocytes (CTLs) have produced complete responses in some patients with refractory NPC in early trials. This approach remains investigational but is one of the most biologically compelling treatment strategies being developed.
EBV DNA as Biomarker
One of the most clinically useful aspects of NPC management — and what distinguishes NPC from almost all other solid tumors — is the availability of a reliable, quantitative blood test for disease activity: plasma EBV DNA. This is cell-free viral DNA shed by NPC tumor cells into the bloodstream, measured by quantitative PCR.
Why It Works
Because essentially all Type II and Type III NPC tumors carry EBV DNA in their cells, as those cells die or shed DNA, detectable EBV DNA circulates in the plasma. The level of circulating EBV DNA correlates closely with tumor burden. No other common cancer has such a specific and sensitive circulating tumor marker derived from an oncovirus.
Clinical Applications
1. Diagnosis: Plasma EBV DNA is elevated in over 90% of patients with Type II and III NPC at diagnosis. A high EBV DNA level in a patient with a neck mass and compatible symptoms strongly supports the diagnosis before tissue confirmation.
2. Prognosis: Pretreatment EBV DNA level is a powerful independent prognostic factor. Chan et al. ( — Search PubMed) demonstrated that higher pretreatment EBV DNA levels predict worse survival, independently of clinical stage. Patients with very high pretreatment levels — say, greater than 4,000 copies/mL — have substantially worse outcomes than patients with lower levels at the same AJCC stage.
3. Treatment monitoring: EBV DNA should fall during chemoradiation as tumor cells are destroyed. Failure of EBV DNA to clear to undetectable levels by the end of treatment, or a rise during treatment, signals incomplete response and may prompt additional imaging or treatment intensification.
4. Surveillance for recurrence: Rising EBV DNA after a complete response — even before symptoms or imaging changes appear — predicts recurrence with a lead time of 6 to 12 months. This allows salvage treatment to begin earlier, when the tumor burden is lower and response rates are higher.
5. Population screening: The Hong Kong NPC Screening Study (Chan et al.) demonstrated that community-level screening using plasma EBV DNA in asymptomatic Chinese men identified NPC at Stage I in approximately 50% of screen-detected cases, compared to only about 15% in historical controls presenting with symptoms. Five-year overall survival in screen-detected Stage I NPC exceeded 97%. This is a proof of concept for population screening in high-incidence communities.
Long-Term Effects and Survivorship
NPC survivors — especially those treated for Stage I–III disease — have long lives ahead of them after successful chemoradiation. The radiation field for NPC encompasses the nasopharynx, skull base, and bilateral neck, meaning several critical structures receive significant radiation dose. Modern IMRT has reduced but not eliminated these late effects.
Radiation-Related Late Effects
- Xerostomia (dry mouth): The parotid glands, which produce the majority of saliva, lie within the radiation field. IMRT spares at least one parotid in most cases, but dry mouth remains common. Severity ranges from mild to severe. Practical management includes frequent sips of water, saliva substitutes, and oral care to prevent dental decay (dry mouth dramatically increases cavity risk). Pilocarpine (a cholinergic drug) can stimulate residual salivary tissue in some patients.
- Trismus: Radiation fibrosis of the pterygoid and masticatory muscles progressively reduces jaw opening (mouth opening). This can make eating and dental care difficult and worsens over time without intervention. Daily jaw-stretching exercises and devices like the TheraBite jaw exerciser can maintain and improve range of motion. Starting exercises early — during or immediately after treatment — is far more effective than waiting until trismus is established.
- Hearing loss: The inner ear (cochlea) lies close to the nasopharynx and receives radiation dose. Cisplatin (used concurrently with radiation) is itself ototoxic. The combination produces cumulative hearing damage, typically high-frequency sensorineural hearing loss. Audiometric monitoring is recommended at regular intervals. Hearing aids are effective when loss is significant.
- Hypothyroidism: The thyroid gland sits in the lower neck, within the radiation field for cervical nodes. Radiation-induced hypothyroidism is common, developing in 20–50% of NPC survivors within 5 years. Annual thyroid function testing (TSH) is standard in follow-up.
- Cranial nerve damage: Radiation can cause delayed cranial nerve injury, particularly affecting CN XII (hypoglossal — tongue movement) and CN IX/X (swallowing). This contributes to chronic swallowing difficulty in some patients.
- Temporal lobe necrosis (TLN): The temporal lobes of the brain are near the superior nasopharynx and skull base. With older radiation techniques, TLN was a significant complication. Modern IMRT substantially reduces the risk; TLN incidence is under 5% with contemporary technique. Re-irradiation for recurrence carries higher risk. Symptoms include headache, memory loss, and seizures.
- Radiation-induced carotid artery disease: Radiation damages the walls of the carotid arteries, accelerating atherosclerosis and increasing stroke risk over decades. Long-term survivors should have vascular risk factors managed aggressively and may benefit from carotid Doppler surveillance.
Psychosocial Concerns
Head and neck cancer survivors face a unique psychosocial burden. Eating difficulties, changes in appearance, voice changes, and fatigue affect quality of life. Depression and anxiety are common in the first 1–2 years. Formal assessment and referral to cancer-specific psychological support improve long-term wellbeing. Speech-language therapists play an important role in managing swallowing rehabilitation. Return to work and social participation are important goals for younger survivors.
Surveillance and Screening
Post-Treatment Surveillance for Treated Patients
After completing treatment, NPC patients require long-term follow-up because:
- Local and regional recurrence most commonly occurs within the first 2 years.
- Distant metastases can appear years later.
- Late radiation-related complications develop and progress over time.
A standard surveillance schedule includes:
- Clinical examination: Every 1–3 months for the first 2 years, every 6 months for years 3–5, then annually thereafter. Each visit includes nasopharyngoscopy to inspect the primary site.
- MRI of nasopharynx and neck: Every 6–12 months for the first 2 years to detect local recurrence, which can be subtle on imaging.
- Plasma EBV DNA: Every 3–6 months. A rising level after a period of undetectability is the most sensitive early indicator of recurrence, often preceding clinical or radiographic evidence by months.
- PET-CT or CT: For equivocal findings on other tests, or if EBV DNA rises without obvious clinical explanation.
- Thyroid function (TSH): Annually, indefinitely — hypothyroidism can develop years after treatment.
- Audiogram: When hearing changes are reported.
- Dental review: Every 6 months, given the long-term caries risk from xerostomia.
Population Screening in High-Incidence Regions
Screening for NPC makes sense in regions where the disease is common enough to justify the effort. Two approaches have been used:
EBV serology: Blood tests measuring IgA antibodies against viral capsid antigen (VCA/EA) have been used for decades in China. However, these tests have limited specificity — many healthy people have positive results — leading to over-investigation.
Plasma EBV DNA: A newer, more specific approach. The Hong Kong NPC Screening Study showed that a single EBV DNA test in asymptomatic high-risk men could identify NPC at early (Stage I) disease with a positive predictive value high enough to justify nasopharyngoscopy confirmation. Stage I NPC detected through screening has approximately 97% 5-year survival — compared to roughly 60–70% for Stage III disease found symptomatically. Opportunistic screening with EBV DNA testing is now recommended for Chinese men aged 40–60 with a family history of NPC, particularly in communities with access to high-volume nasopharyngoscopy.
Salvage Treatment for Recurrence
Despite high cure rates with modern chemoradiation, approximately 10–20% of NPC patients develop local or regional recurrence, and a similar proportion develop distant metastases. The approach to recurrence depends on site, extent, and prior treatment.
Local Recurrence (Nasopharynx)
Re-treating the nasopharynx after full-dose primary radiation is technically challenging because the surrounding normal tissues (brainstem, spinal cord, cranial nerves, carotid arteries) are already at or near tolerance dose. Options include:
- Re-irradiation: Stereotactic body radiotherapy (SBRT) or stereotactic radiosurgery (SRS) can deliver precise high-dose radiation to limited recurrent volumes. Brachytherapy (intracavitary radiation using implanted applicators) is another technique for small, accessible recurrences. Proton therapy, where available, spares surrounding normal tissue better than photons in re-irradiation settings.
- Salvage nasopharyngectomy: Surgical removal of recurrent tumor in the nasopharynx. This is technically demanding given the deep skull-base location. Both endoscopic approaches and open surgery (via infratemporal fossa or midface access) have been described at specialized centers. Surgery is preferred for small, accessible recurrences where re-irradiation risk is high.
Regional (Nodal) Recurrence
Isolated nodal recurrence can be managed with:
- Surgical neck dissection for resectable nodal disease.
- Re-irradiation (regional radiotherapy) when surgery is not feasible.
- Combined approaches in selected patients.
Metastatic Recurrence
Distant metastases are treated with systemic therapy. The standard first-line regimen is gemcitabine + cisplatin (GC). In patients whose disease progresses on GC, immunotherapy (anti-PD-1 agents) is an established second-line option with meaningful response rates. EBV-specific adoptive T-cell therapy is available in clinical trials at specialized centers for refractory disease. Bone metastases can be palliated with stereotactic radiotherapy.
Prevention
Given the well-characterized risk factors for NPC, several prevention strategies are logical — though only dietary change has strong epidemiological evidence at the population level.
Dietary Modification
Reducing salted fish consumption, especially in childhood, is the most evidence-supported preventive measure. The dramatic reduction in NPC incidence in younger generations of Hong Kong Chinese and among Chinese diaspora communities that have adopted Western dietary patterns — with less traditional preserved food — supports the hypothesis that nitrosamines from salted fish during early life are a critical exposure. Parents from high-risk families are advised to limit preserved fish in children's diets.
EBV Vaccination (Research Stage)
Because EBV drives the majority of NPC worldwide, an effective EBV vaccine could theoretically prevent NPC (and also reduce risk of EBV-associated lymphomas and other cancers). Several EBV vaccine candidates are in development and early clinical trials, including virus-like particle (VLP) vaccines targeting the EBV glycoprotein complex required for cell infection. No EBV vaccine is currently approved. This remains one of the most important potential cancer prevention advances in development.
Tobacco Cessation
Smoking is linked specifically to Type I (keratinizing) NPC. Tobacco cessation reduces this risk as well as the risk of many other head and neck and lung cancers.
Occupational Exposure Reduction
Workers with prolonged exposure to formaldehyde (embalmers, certain factory workers) or wood dust have modestly elevated NPC risk. Standard occupational health protective measures (ventilation, personal protective equipment) are advisable.
Genetic Counseling for High-Risk Families
First-degree relatives of NPC patients — particularly those with Cantonese Chinese ancestry — have 4- to 10-fold higher risk and may benefit from targeted education about symptoms, dietary risk factors, and the availability of EBV DNA screening programs where these exist.
Key Research Papers
The following studies have defined how nasopharyngeal carcinoma is treated and understood today. Each citation links to PubMed or the original source.
-
Zhang L et al. (2016) — Gemcitabine plus cisplatin versus fluorouracil plus cisplatin in recurrent or metastatic nasopharyngeal carcinoma: a multicentre, randomised, phase 3, non-inferiority trial. Lancet / New England Journal of Medicine.
Search PubMed — Established GC as the standard first-line regimen for R/M NPC (median OS 29.1 vs 20.9 months). -
Zhang Y et al. (2019) — Gemcitabine and Cisplatin Induction Chemotherapy in Nasopharyngeal Carcinoma. New England Journal of Medicine.
Search PubMed — Phase III trial showing GP induction before concurrent chemoRT significantly improved failure-free survival in Stage III–IVB NPC. -
Chan ATC et al. (2013) — Plasma Epstein-Barr virus (EBV) DNA as a biomarker for NPC: prognostic value in early-stage and locoregionally advanced disease. Journal of Clinical Oncology.
Search PubMed — Demonstrated pretreatment plasma EBV DNA as a powerful independent prognostic factor. -
Al-Sarraf M et al. (1998) — Chemoradiotherapy versus radiotherapy in patients with advanced nasopharyngeal cancer: phase III randomized intergroup study 0099. Journal of Clinical Oncology.
PMID 9440738 — The INT 0099 landmark trial; established cisplatin chemoRT as the standard over RT alone; dramatically improved 3-year PFS (69% vs 24%). -
Lin JC et al. (2003) — Phase III study of concurrent chemoradiotherapy versus radiotherapy alone for advanced nasopharyngeal carcinoma. New England Journal of Medicine.
Search PubMed — Confirmed superiority of concurrent cisplatin + RT over RT alone in a different trial population; pivotal Asian validation of chemoRT. -
Chua MLK et al. (2016) — Nasopharyngeal carcinoma. Lancet.
Search PubMed — Comprehensive review of NPC epidemiology, biology, diagnosis, staging, treatment, and survivorship. -
Wei WI, Sham JST (2005) — Nasopharyngeal carcinoma. Lancet.
Search PubMed — Classic review covering epidemiology, EBV biology, clinical features, and treatment principles from leading Hong Kong experts. -
Chan KCA et al. (2013) — Analysis of plasma Epstein-Barr virus DNA to screen for nasopharyngeal cancer. New England Journal of Medicine.
Search PubMed — Hong Kong community screening study; plasma EBV DNA detected Stage I NPC in ~50% of screen-detected cases vs ~15% historically. -
Loong HH et al. (2021) — Anti-PD-1 immunotherapy in recurrent and metastatic nasopharyngeal carcinoma: evidence from clinical trials. Therapeutic Advances in Medical Oncology.
Search PubMed — Summarizes phase I/II/III data on PD-1 inhibitors (camrelizumab, nivolumab, pembrolizumab) in R/M NPC. -
Lee AWM et al. (2005) — Factors affecting risk of symptomatic temporal lobe necrosis: significance of fractional dose and treatment time. International Journal of Radiation Oncology Biology Physics.
Search PubMed — Key study on temporal lobe necrosis risk factors in NPC radiation; foundational for modern dose constraint guidelines. -
NCCN Clinical Practice Guidelines in Oncology: Head and Neck Cancers (2024) — Covers NPC diagnosis, staging, and treatment algorithms including induction chemotherapy, concurrent chemoRT, and systemic therapy recommendations.
NCCN Guidelines — Head and Neck Cancers -
MAC-NPC Collaborative Group (2015) — Induction or adjuvant chemotherapy in addition to concurrent chemoradiotherapy: Meta-analysis of randomised trials in nasopharyngeal carcinoma. Annals of Oncology.
Search PubMed — Pooled analysis of 19 trials showing the magnitude of survival benefit from adding chemotherapy to RT in NPC, confirming concurrent chemotherapy gives the largest benefit.
Additional PubMed searches for ongoing and emerging NPC research:
- Nasopharyngeal carcinoma immunotherapy (PubMed, sorted by date)
- EBV plasma DNA nasopharyngeal cancer (PubMed, sorted by date)
- Nasopharyngeal carcinoma IMRT outcomes (PubMed, sorted by date)
- NPC induction chemotherapy gemcitabine (PubMed, sorted by date)
Connections
- Oncology
- All Conditions
- Cancer Overview
- Head and Neck Cancer
- Oral Cancer
- Lymphoma
- Thyroid Cancer
- Brain Cancer
- Epstein-Barr Virus (EBV)
- Turmeric
- Vitamin D3
- Selenium and Cancer Prevention