Liver Cancer
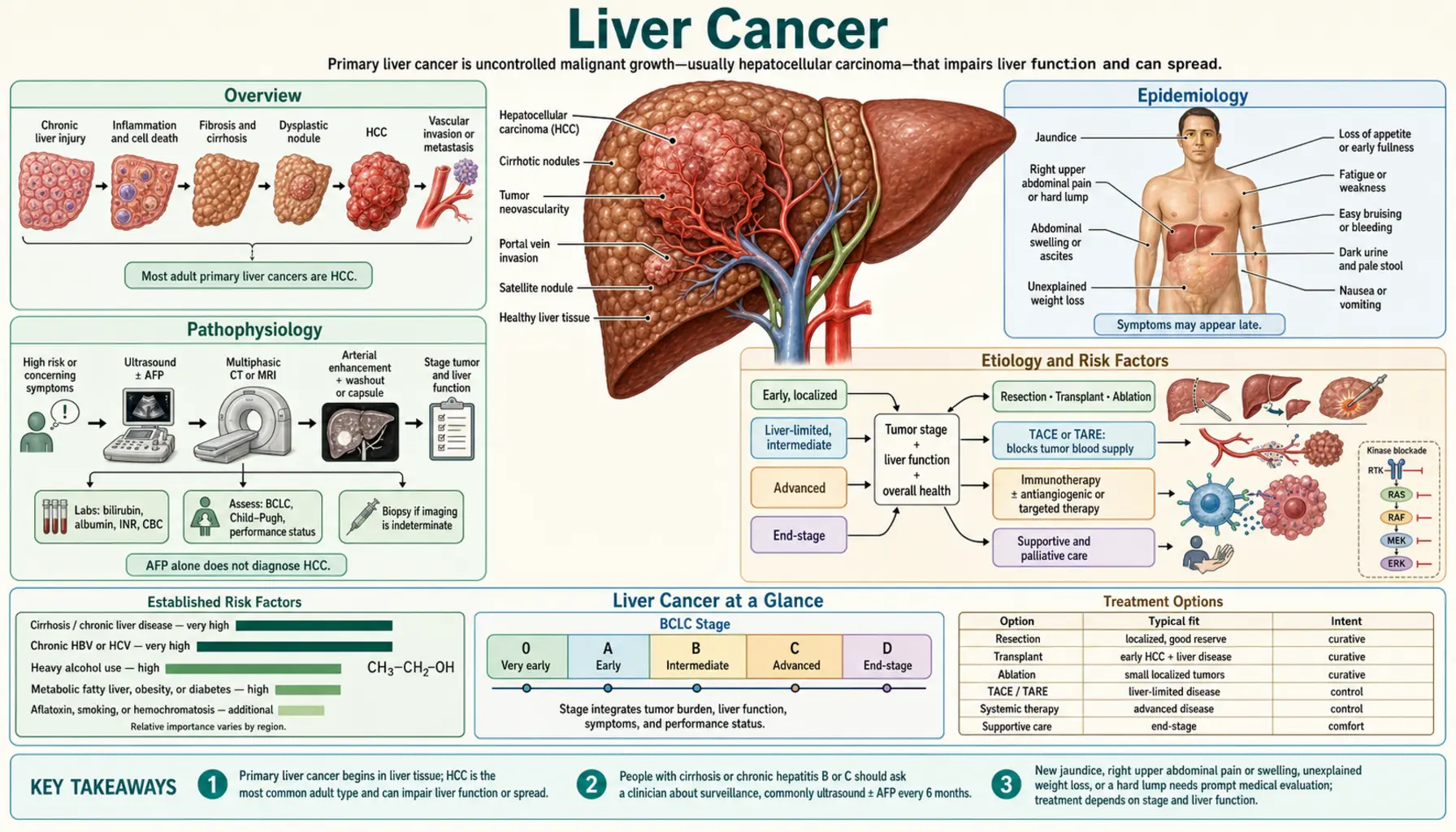
Table of Contents
- Overview
- Epidemiology
- Pathophysiology
- Etiology and Risk Factors
- Clinical Presentation
- Diagnosis
- Treatment
- Complications
- Prognosis
- Prevention
- Recent Research and Advances
- Research Papers
- Connections
- Featured Videos
1. Overview
Liver cancer means cancer that starts in the liver itself — and in about 90% of cases, that cancer is hepatocellular carcinoma (HCC), a tumor arising from hepatocytes, the workhorse cells that make up most of the liver. (Cancers that spread to the liver from the colon, breast, pancreas, or lung are far more common, but those are metastatic cancers and are treated according to where they started — they are covered on the Metastatic Cancers page.) A smaller share of primary liver cancers are cholangiocarcinomas, which arise from the bile ducts; this article focuses on HCC.
Two facts make liver cancer different from almost every other cancer, and they shape everything else on this page.
First: liver cancer is one of the few cancers in the United States whose death rate has been rising while deaths from most other cancers fall. The engine behind that rise is not a mystery. It is the fatty liver epidemic — non-alcoholic fatty liver disease (NAFLD, now formally renamed MASLD, metabolic dysfunction-associated steatotic liver disease), driven by obesity and type 2 diabetes. Roughly one in three American adults has fat accumulating in the liver. In a fraction of them, that fat triggers years of smoldering inflammation, then scarring (cirrhosis), and eventually, in some, cancer. Liver cancer is in a real sense the oncologic endpoint of the metabolic disease epidemic.
Second: 80–90% of hepatocellular carcinomas arise in livers that are already cirrhotic. Unlike pancreatic or ovarian cancer, which strike out of nowhere, liver cancer almost always announces its territory decades in advance. It is usually the final stage of a chronic liver disease that the patient — and the medical system — had every opportunity to know about: hepatitis B, hepatitis C, alcohol-related liver disease, fatty liver disease, or hemochromatosis. That is grim, but it carries an enormous practical silver lining: the at-risk population is identifiable, which means surveillance is possible. We can watch the livers most likely to develop cancer and catch tumors while they are still small and curable. The single most important message on this page is in Section 10: if you have cirrhosis from any cause, or chronic hepatitis B, you should be getting a liver ultrasound (usually with an AFP blood test) every six months — and most people who qualify are not getting it.
Treatment has also changed dramatically. For patients diagnosed early, ablation, surgery, and especially liver transplantation — which removes both the cancer and the diseased liver that produced it — offer genuine cures. For advanced disease, immunotherapy combinations introduced since 2020 have, for the first time, meaningfully extended survival beyond what the older pill sorafenib could achieve. The gap between an early diagnosis and a late one has never been wider, which is exactly why surveillance matters so much.
2. Epidemiology
Worldwide, liver cancer is the sixth most commonly diagnosed cancer and the third leading cause of cancer death, with roughly 900,000 new cases and over 800,000 deaths each year. The global map of liver cancer has historically followed the map of chronic hepatitis B: East Asia and sub-Saharan Africa carry the heaviest burden, where HBV is often acquired at birth and aflatoxin-contaminated food multiplies the risk.
In the United States, the story is one of unwelcome growth. Liver cancer incidence roughly tripled between 1980 and the mid-2010s, and while incidence has recently begun to plateau, liver cancer remains one of the few major cancers with a rising death rate. The American Cancer Society estimates over 40,000 new primary liver cancer diagnoses and around 30,000 deaths in the US annually. Men are affected two to three times more often than women, and the typical age at diagnosis is in the 60s.
The causes behind US cases have shifted in a single generation:
- Hepatitis C drove the first wave of the increase — the large group of Americans infected in the 1960s–1980s (often via blood transfusion before 1992 screening, or injection drug use) aged into cirrhosis and cancer decades later. Curative antiviral pills (DAAs, available since 2014) are now shrinking this group.
- Fatty liver disease (MASLD/NAFLD) is the fastest-growing cause and is projected to become the leading cause of HCC in the US and much of the West. Because fatty liver is so common, even a small per-person cancer risk translates into a large number of cancers — and because many fatty-liver patients have never been told they have liver disease at all, their cancers are disproportionately found late, outside of any surveillance program.
- Alcohol-related cirrhosis remains a major, stable contributor.
- Hepatitis B matters most among Americans born in regions where HBV is common (Asia, the Pacific Islands, sub-Saharan Africa) and is the reason screening recommendations specifically include foreign-born populations.
Survival statistics reflect how late most liver cancers are found: the overall 5-year relative survival in the US is about 22% — but for localized disease it exceeds 37%, and for small tumors treated with transplant or ablation it is above 70%. The difference between those numbers is mostly a difference in when the cancer was found.
3. Pathophysiology
Hepatocellular carcinoma is best understood as the end product of decades of injury, repair, and regeneration. The liver is the body's most regenerative organ — it can regrow most of its mass after injury — but that superpower comes with a cost. Every cycle of cell death and replacement is another round of DNA copying, and chronic liver disease forces hepatocytes through thousands of extra division cycles in an environment full of inflammation and oxidative stress. Mutations accumulate. Eventually a clone of hepatocytes escapes normal growth control.
The usual sequence runs: chronic injury → inflammation (hepatitis) → fibrosis (scarring) → cirrhosis → dysplastic nodules → carcinoma. Cirrhosis is the critical soil: a cirrhotic liver is a field of regenerative nodules, each one a population of stressed, rapidly dividing cells under selection pressure. This is why 80–90% of HCC arises in cirrhotic livers, and why cirrhosis of any cause — viral, alcoholic, metabolic, genetic — confers HCC risk on the order of 1–4% per year.
The important exceptions and mechanisms worth knowing:
- Hepatitis B can cause cancer without cirrhosis. HBV is a DNA virus that physically integrates its genetic material into the host hepatocyte genome, where it can disrupt tumor-suppressor genes and activate growth pathways directly. The viral HBx protein also interferes with DNA repair. This direct oncogenic action means a person with chronic hepatitis B can develop HCC with little or no scarring — which is why surveillance criteria for hepatitis B are based on age, sex, ancestry, and family history rather than waiting for cirrhosis.
- Hepatitis C is an RNA virus that does not integrate into DNA; its cancer risk works almost entirely through the inflammation-fibrosis-cirrhosis pathway. That is why curing HCV before cirrhosis develops nearly eliminates the risk, while curing it after cirrhosis is established reduces — but does not erase — it.
- Fatty liver disease promotes cancer through lipotoxicity (fat-overloaded hepatocytes under metabolic stress), chronic low-grade inflammation, insulin resistance with elevated insulin and IGF-1 (both growth signals), and changes in the gut microbiome. Notably, a meaningful minority of MASLD-related HCC — perhaps 20–30% — occurs before full cirrhosis, which complicates surveillance.
- Aflatoxin B1, a toxin from Aspergillus molds on improperly stored grain and peanuts, causes a signature mutation in the TP53 tumor-suppressor gene and acts synergistically with hepatitis B — the combination multiplies risk far beyond either alone.
- Iron overload (hemochromatosis) drives oxidative DNA damage via free iron catalyzing reactive oxygen species.
At the molecular level, the most common driver alterations in HCC are TERT promoter mutations (reactivating telomerase, found in over half of tumors), TP53 and CTNNB1 (beta-catenin) mutations. Frustratingly, none of these is currently druggable, which is why HCC treatment has moved toward immunotherapy and anti-angiogenic strategies rather than the mutation-targeted pills used in lung cancer or melanoma.
4. Etiology and Risk Factors
Almost every case of liver cancer has an identifiable cause. In rough order of global importance:
- Chronic hepatitis B (HBV). The leading cause worldwide (around half of all HCC). Risk is highest with infection acquired at birth or in early childhood, high viral loads, male sex, age over 40, a family history of liver cancer, and African or Asian ancestry. Because HBV is directly oncogenic, cirrhosis is not required. The flip side: the hepatitis B vaccine is, quite literally, a cancer-prevention vaccine — the first one ever deployed (see Prevention).
- Chronic hepatitis C (HCV). The historical driver of the US epidemic. Risk concentrates in those who have progressed to advanced fibrosis or cirrhosis. Direct-acting antivirals (DAAs) now cure more than 95% of infections in 8–12 weeks of pills, and achieving cure cuts subsequent HCC risk by roughly 70% — but in patients who were already cirrhotic at the time of cure, a meaningful residual risk persists for years, so surveillance must continue even after the virus is gone.
- Alcohol. Heavy, sustained drinking causes cirrhosis, and alcohol-related cirrhosis carries roughly a 1–2% per year HCC risk. Alcohol also multiplies the risk from coexisting hepatitis or fatty liver. See Addiction for help with alcohol use.
- MASLD/NAFLD, diabetes, and obesity. The fastest-growing cause in the US and Europe. Type 2 diabetes approximately doubles to triples HCC risk independent of other factors; obesity adds further risk. Most MASLD-related cancers arise in patients with advanced fibrosis or cirrhosis, but a substantial minority do not — one reason metabolic liver disease deserves more respect than it usually gets in a primary-care visit.
- Hereditary hemochromatosis. Untreated iron overload with cirrhosis carries among the highest per-year HCC risks of any liver disease. Early diagnosis and phlebotomy (blood removal) largely prevent it — one more argument for checking ferritin and transferrin saturation when liver enzymes are unexplained. See Hemochromatosis.
- Aflatoxin exposure. Mostly a problem in parts of Africa and Asia where grain and groundnut storage conditions favor mold; it synergizes powerfully with hepatitis B. In countries with regulated food supplies, dietary aflatoxin exposure is low.
- Other contributors: tobacco smoking (a genuine, underappreciated liver carcinogen), alpha-1 antitrypsin deficiency, autoimmune hepatitis with cirrhosis, primary biliary cholangitis, and anabolic steroid abuse. Oral contraceptives are linked to benign hepatic adenomas, which rarely transform.
If you recognize yourself in items 1–5, the action item is not anxiety — it is enrollment in surveillance. Every one of these risk groups is identifiable years before cancer develops.
5. Clinical Presentation
Here is the uncomfortable truth: early liver cancer causes no symptoms at all. The liver has no pain fibers in its interior, enormous functional reserve, and plenty of room. A 2 cm tumor — comfortably in the curable range — announces itself in no way whatsoever. This is precisely why surveillance imaging exists, and why waiting for symptoms is a strategy that finds cancers too late.
When symptoms do appear, the tumor is usually large, multifocal, or the underlying cirrhosis is decompensating. Common presentations include:
- Right upper abdominal pain or fullness — a dull ache under the right ribs as the tumor stretches the liver capsule.
- Unintentional weight loss and loss of appetite, sometimes with early satiety.
- Worsening of previously stable cirrhosis — this one matters. New ascites (fluid in the abdomen), new jaundice, new confusion (hepatic encephalopathy), or variceal bleeding in someone whose cirrhosis had been quiet for years should always prompt imaging to look for a tumor, including tumor invading the portal vein.
- A palpable mass or enlarged liver in advanced cases.
- Fatigue, low-grade fever, and generalized itching.
- Paraneoplastic effects (uncommon but classic): low blood sugar, high calcium, high red blood cell count (the tumor can secrete erythropoietin), and watery diarrhea.
Two practical points for patients and families. First, if you have known cirrhosis and you feel fine, that is exactly when surveillance is most valuable — you are looking for the tumor that does not hurt yet. Second, if you or a loved one has cirrhosis that suddenly gets worse without an obvious trigger, ask directly: “Has anyone checked for liver cancer?” It is a reasonable, answerable question, and a multiphase scan settles it quickly.
6. Diagnosis
Surveillance: how liver cancer should be found
In an ideal world, most liver cancers would be discovered the boring way: on a scheduled ultrasound, with or without an alpha-fetoprotein (AFP) blood test, every 6 months, in a patient known to have cirrhosis or high-risk chronic hepatitis B. Ultrasound is painless, radiation-free, takes fifteen minutes, and is inexpensive. AFP is a simple blood draw; it is elevated in many (not all) liver cancers, and adding it to ultrasound improves detection of early tumors. The six-month interval is not arbitrary — it is matched to how fast a typical HCC doubles in size, so that a tumor born just after one scan is still small and curable at the next. Pooled analyses show surveillance roughly doubles the rate of early-stage detection and curative treatment and is associated with significantly better survival. Yet in US studies, fewer than one in four eligible patients receives guideline-concordant surveillance. If you have cirrhosis and nobody has scheduled your next ultrasound, ask.
Confirming the diagnosis: imaging often replaces biopsy
Liver cancer has an unusual diagnostic privilege: in a cirrhotic liver, HCC can be diagnosed definitively by imaging alone, without a biopsy. Here is why that is legitimate and not a shortcut. A growing HCC rewires its blood supply: normal liver tissue is fed mostly by the portal vein, but HCC feeds almost exclusively from the hepatic artery. On a multiphase contrast CT or MRI — where images are captured in timed phases as contrast dye flows through — this produces a fingerprint: the tumor lights up brightly in the arterial phase (arterial hyperenhancement) and then becomes darker than the surrounding liver in later phases (washout). In a patient who already has cirrhosis (a high-prevalence population), this pattern in a nodule over 1–2 cm is so specific — well above 95% — that radiologists grade it using a standardized system called LI-RADS, and a LI-RADS 5 lesion is treated as definite HCC. Avoiding biopsy spares patients bleeding risk in a clotting-impaired cirrhotic liver and a small risk of seeding tumor cells along the needle track.
Biopsy still has a role when imaging is inconclusive, when the liver is not cirrhotic (where the imaging shortcut is not validated), or when the diagnosis could be something else such as cholangiocarcinoma or a metastasis.
Staging: the BCLC framework
Liver cancer staging is unusual because it must grade two diseases at once: the cancer and the cirrhosis underneath it. A small tumor in a failing liver may be less treatable than a larger tumor in a strong one. The dominant system, Barcelona Clinic Liver Cancer (BCLC), therefore combines three things — tumor burden (size, number, vascular invasion, spread), liver function (Child-Pugh score, bilirubin, ascites), and the patient's overall fitness — and maps each combination directly to a recommended treatment:
- Stage 0 (very early) — single tumor under 2 cm, preserved liver function → ablation or resection; potentially curative.
- Stage A (early) — single tumor, or up to 3 tumors each ≤3 cm → resection, transplant, or ablation; potentially curative.
- Stage B (intermediate) — multiple tumors confined to the liver → catheter-based therapy (TACE/TARE), with transplant possible for selected patients.
- Stage C (advanced) — vascular invasion or spread outside the liver → systemic therapy (immunotherapy combinations).
- Stage D (terminal) — severe liver failure or poor functional status → best supportive care, with transplant considered only if the patient qualifies for it.
Workup also includes blood tests of liver function (bilirubin, albumin, INR, platelets), AFP (which, when very high, signals more aggressive biology), and chest/abdomen/pelvis imaging to look for spread — most often to lungs, abdominal lymph nodes, and bone.
7. Treatment
Treatment is chosen by BCLC stage, and the options fall into three tiers: curative (ablation, resection, transplant), liver-directed (TACE, TARE), and systemic (immunotherapy and targeted pills). Patients are best served at centers with a multidisciplinary liver tumor board — hepatology, transplant surgery, interventional radiology, and oncology in one room — because the “right” answer often shifts as the liver and tumor evolve.
Curative options
- Thermal ablation. For tumors up to about 3 cm, an interventional radiologist passes a needle-like probe through the skin into the tumor under imaging guidance and destroys it with heat (radiofrequency or microwave). For the smallest tumors, outcomes rival surgery, with a far smaller procedure — often an overnight stay. The catch: the cirrhotic liver remains, and new tumors arise elsewhere in it at a substantial rate, so surveillance continues for life.
- Surgical resection. Removing the tumor-bearing segment of liver is the preferred cure for patients without cirrhosis and for cirrhotic patients with well-preserved liver function and no significant portal hypertension. The limiting factor is whether the remaining liver is healthy enough to do the body's chemistry; resecting a tumor from a frail cirrhotic liver risks trading cancer for liver failure. Five-year survival after resection of early HCC is on the order of 60–70%, but recurrence — usually new tumors in the remaining cirrhotic liver — exceeds 50% at 5 years.
- Liver transplantation — the most complete cure. Transplant is unique: it removes the cancer and the cirrhotic liver that produced it, simultaneously curing both diseases. The landmark 1996 Milan study established the rule still used today: patients whose tumor burden is within the Milan criteria — one tumor ≤5 cm, or up to three tumors each ≤3 cm, with no vascular invasion or spread — achieve post-transplant survival nearly identical to patients transplanted without cancer, with 4-year survival of 75–85% and recurrence under 10–15%. The realities to understand: donor livers are scarce, so patients within Milan criteria receive standardized priority points on the waiting list (after a 6-month delay designed to let aggressive tumor biology declare itself); typical waits run months to over a year depending on region and blood type; and while waiting, the tumor is held in check with ablation or TACE (“bridging therapy”). Patients whose tumors are modestly beyond Milan can sometimes be “downstaged” into criteria with liver-directed therapy and then transplanted. Living-donor transplant, where a healthy person donates part of their liver, can bypass the waitlist entirely for suitable pairs. If there is any chance you qualify, push for referral to a transplant center early — the evaluation takes time, and eligibility can close if the tumor grows.
Liver-directed (catheter-based) therapy
- TACE (transarterial chemoembolization). Exploits the same arterial blood supply that makes imaging diagnosis possible: a catheter is threaded into the artery feeding the tumor, chemotherapy is delivered directly into it, and the artery is then blocked, starving the tumor while sparing the portal-vein-fed normal liver. TACE is the standard for intermediate-stage (BCLC B) disease and a common bridge to transplant. It controls tumors and extends survival but is rarely curative alone; it is often repeated.
- TARE (transarterial radioembolization, or Y-90). The same catheter approach, but delivering microscopic beads loaded with the radioactive isotope yttrium-90. It is generally better tolerated than TACE (less post-procedure pain and fever) and can shrink tumors enough to enable resection or transplant. High-dose “radiation segmentectomy” of small tumors can approach ablative results.
- External-beam radiation (SBRT) — precisely focused radiation over a few sessions — is an option for tumors that ablation cannot reach safely.
Systemic therapy for advanced disease
For decades, advanced HCC had essentially nothing: traditional chemotherapy does not work well in a cirrhotic liver or against this tumor. The first crack came in 2008, when the targeted pill sorafenib (SHARP trial) extended median survival by about three months — modest, but proof that systemic treatment was possible. Lenvatinib matched sorafenib in 2018. The real shift came in 2020:
- Atezolizumab plus bevacizumab (IMbrave150 trial) — an immune checkpoint inhibitor (anti-PD-L1) paired with an anti-angiogenic antibody (anti-VEGF) — became the first regimen ever to beat sorafenib head-to-head, improving survival and quality of life; median overall survival reached about 19 months in updated analyses. It is now a standard first-line treatment for advanced HCC in patients with preserved liver function. (Because bevacizumab raises bleeding risk, patients need endoscopy first to treat any varices.)
- Durvalumab plus tremelimumab (HIMALAYA trial, 2022) — a dual-immunotherapy combination (anti-PD-L1 plus a single priming dose of anti-CTLA-4, the “STRIDE” regimen) — also beat sorafenib and offers an alternative first-line option, particularly when bevacizumab is unsafe.
- Second-line options after progression include regorafenib, cabozantinib, ramucirumab (for AFP ≥400), and other checkpoint-inhibitor combinations. Trials are now testing immunotherapy earlier — added to TACE and after curative resection or ablation.
Throughout all of this, the underlying liver disease is treated in parallel: antivirals for hepatitis B, cure of hepatitis C, complete alcohol cessation, and management of ascites and encephalopathy. A controlled tumor in a failing liver is still a losing position; protecting liver function is half the battle.
8. Complications
Complications come from three directions — the tumor, the cirrhosis, and the treatments — and they interact.
- Liver failure / decompensation. The most common final pathway. Tumor growth plus cirrhosis progressively erodes liver function, producing jaundice, fluid accumulation (ascites), and hepatic encephalopathy (confusion from toxins the liver no longer clears). Many patients with HCC ultimately die of liver failure rather than of distant cancer spread.
- Portal vein tumor thrombosis. HCC has a notorious tendency to grow directly into the portal vein. This worsens portal hypertension abruptly — triggering ascites and variceal bleeding — and moves the cancer into advanced stage, generally taking resection and transplant off the table.
- Variceal hemorrhage. Bleeding from swollen veins in the esophagus or stomach, a cirrhosis complication intensified by tumor-related portal hypertension. This is a 911-level emergency: vomiting blood or black, tarry stools requires immediate care.
- Tumor rupture. Uncommon but dramatic — a tumor on the liver surface bleeds into the abdomen, causing sudden severe pain and shock. Treated with emergency embolization.
- Metastases. When HCC spreads beyond the liver, it favors the lungs, abdominal lymph nodes, and bone (bone pain or fracture may rarely be the first symptom).
- Biliary obstruction, causing jaundice and itching when tumor compresses bile ducts.
- Paraneoplastic syndromes: hypoglycemia, hypercalcemia, and erythrocytosis.
- Treatment-related effects: post-embolization syndrome after TACE (a few days of pain, fever, fatigue — expected and self-limited); immune-related inflammation of thyroid, gut, skin, or lungs on checkpoint inhibitors (report new symptoms early — these are treatable when caught); hypertension and bleeding on bevacizumab; hand-foot skin reaction and diarrhea on sorafenib/lenvatinib; and lifelong immunosuppression after transplant.
9. Prognosis
Honest numbers, with the context that makes them meaningful.
- Overall, the 5-year relative survival for liver cancer in the US is about 22%. That figure is low because most liver cancers are still diagnosed late — it is an average dominated by missed surveillance.
- Caught early and treated curatively, the picture inverts. Patients transplanted within Milan criteria see 4-year survival of 75–85% — comparable to transplant patients without cancer — and 5-year survival after transplant or successful early resection/ablation exceeds 70%. Very early tumors (<2 cm) treated with ablation or resection do better still.
- Localized disease (still confined to the liver at diagnosis) carries roughly 37% five-year survival as a category; regional spread drops to about 13%; distant metastatic disease to about 3–4%.
- Advanced disease on modern systemic therapy: median overall survival with atezolizumab-bevacizumab is around 19 months, versus about 13 months with sorafenib and 8 months or less untreated — real progress, with a meaningful minority of patients living considerably longer on immunotherapy, though not yet a cure.
What actually determines an individual's outcome is a three-legged stool: tumor stage at diagnosis (the leg you can influence through surveillance), liver function (Child-Pugh class — a strong liver tolerates aggressive treatment; a failing one forecloses options), and access to multidisciplinary care (transplant evaluation, interventional radiology, clinical trials). Recurrence deserves mention too: after resection or ablation, the remaining cirrhotic liver keeps its cancer-forming potential, and new tumors appear in over half of patients within five years — which is why follow-up imaging continues indefinitely, and why transplant, which replaces the whole organ, has the lowest recurrence of any treatment.
If you are reading this with a new diagnosis: the spread between these numbers is exactly why second opinions at a liver transplant center are worth the effort. Patients are regularly told they are “not candidates” for curative options by teams that do not perform them.
10. Prevention
Liver cancer is among the most preventable of all major cancers, because nearly every causal pathway can be interrupted — some with a vaccine, some with a prescription, some at the grocery store.
Interrupt the causes
- Hepatitis B vaccination — the first cancer-prevention vaccine. The HBV vaccine (introduced 1981, universal infant vaccination in the US since 1991) prevents the infection that causes about half the world's liver cancer. Taiwan proved the concept at national scale: after universal newborn vaccination began in 1984, childhood liver cancer incidence fell measurably within 15 years. US adults under 60 who were never vaccinated are now routinely recommended to get the series. If you were born before universal vaccination and have any risk factors, ask for the vaccine — it is cheap, safe, and it prevents cancer.
- Test and treat hepatitis B and C. The CDC recommends every adult be screened at least once for both hepatitis B and hepatitis C — most infected people feel fine and do not know. Chronic HBV is controlled (not cured) with safe daily antivirals that lower cancer risk substantially. Chronic HCV is cured in over 95% of people with 8–12 weeks of well-tolerated pills, cutting subsequent HCC risk by roughly 70%. One crucial caveat: if cirrhosis was already present before the cure, cancer risk persists and 6-month surveillance must continue indefinitely. Cure the virus; keep the ultrasounds.
- Alcohol. The dose-response is real and steep once cirrhosis enters the picture. If you have any chronic liver disease, the safe amount of alcohol is zero. If drinking is hard to stop, that is a medical problem with real treatments — see Addiction.
- Treat the metabolic engine. Because fatty liver is now the fastest-growing cause of liver cancer, weight loss (7–10% of body weight measurably reduces liver fat and inflammation), diabetes control, and exercise are genuine cancer prevention. Observational data suggest metformin use in diabetics is associated with lower HCC risk. See Fatty Liver Disease, Diabetes, and Obesity.
- Screen the family for hemochromatosis if it runs in yours; early phlebotomy prevents the cirrhosis that precedes the cancer.
- Avoid aflatoxin. Globally important: proper drying and storage of grain, corn, and peanuts prevents mold growth. In countries with regulated food supplies, exposure is low — discard visibly moldy nuts and grains and store them dry.
Coffee — yes, really
Coffee drinking is associated with substantially lower liver cancer risk, with a dose-response relationship — one of the most consistent findings in liver epidemiology. A systematic review and dose-response meta-analysis of over 2.2 million participants (Kennedy et al., BMJ Open 2017) found each 2 cups per day associated with roughly a 35% reduction in HCC risk; other meta-analyses estimate 15–40% depending on intake, and the association holds in people with existing liver disease and for decaffeinated coffee (somewhat weaker), suggesting compounds beyond caffeine — chlorogenic acids, kahweol, cafestol — that reduce liver enzyme levels, fibrosis, and oxidative stress. The honest caveats: this is observational evidence, not a randomized trial; coffee drinkers differ from non-drinkers in many ways; and no one should view coffee as an antidote to alcohol, obesity, or untreated hepatitis. But for a habit most people already have, the direction of the evidence is comfortingly one-way — there is no signal of harm to the liver. Guidelines from major liver societies have gone as far as noting coffee's probable benefit in chronic liver disease. Three cups a day is a reasonable, evidence-aligned habit. See Coffee.
Surveillance: prevention's safety net
Prevention sometimes fails, which is why this page keeps returning to one message. If you have cirrhosis from any cause — viral, alcoholic, metabolic, autoimmune, genetic — or chronic hepatitis B with risk factors (men of Asian ancestry over 40, women over 50, African ancestry over 20, anyone with a family history of HCC), you should have a liver ultrasound, usually with AFP, every 6 months. For life. Even if you feel perfectly well. Even after your hepatitis C is cured. Surveillance is how liver cancer is found at the stage where the 5-year survival number starts with a 7 instead of a 2. Fewer than a quarter of eligible Americans actually receive it — not because it is controversial, but because nobody put it on the calendar. Put it on the calendar.
11. Recent Research and Advances
Liver cancer research is moving quickly on several fronts:
- Immunotherapy moving earlier. After IMbrave150 (atezolizumab-bevacizumab) and HIMALAYA (durvalumab-tremelimumab) transformed advanced disease, trials are testing checkpoint inhibitors in earlier settings: combined with TACE for intermediate-stage disease (the EMERALD-1 trial reported longer progression-free survival adding durvalumab-bevacizumab to TACE) and as adjuvant therapy after resection or ablation to reduce recurrence (IMbrave050 showed an early recurrence-free survival signal that attenuated with follow-up — the question remains open).
- Better blood-based surveillance. Ultrasound misses more early tumors in obese patients and fatty livers — precisely the growing MASLD population. Biomarker panels such as GALAD (combining gender, age, AFP, AFP-L3, and des-gamma-carboxy prothrombin) and liquid-biopsy approaches (circulating tumor DNA, methylation signatures) are being validated as supplements or alternatives to ultrasound, with abbreviated MRI protocols studied for high-risk patients.
- Risk stratification within fatty liver disease. With a third of adults having MASLD, surveillance cannot cover everyone. Research is refining who actually needs it: fibrosis staging by elastography (FibroScan), genetic risk variants such as PNPLA3, and clinical scores that concentrate surveillance on the minority with advanced fibrosis.
- Transplant criteria evolving. Centers increasingly use tumor biology (AFP trends, response to bridging therapy) rather than size alone, formalizing downstaging pathways so more patients reach transplant without sacrificing outcomes.
- Hepatitis B cure research. Current antivirals suppress HBV but rarely eliminate it. A “functional cure” pipeline — capsid assembly modulators, siRNA therapies, therapeutic vaccines — aims to do for hepatitis B what DAAs did for hepatitis C, with major implications for global liver cancer rates.
- Mechanisms of MASLD-driven cancer — including how specific gut microbiome changes and immune alterations in fatty livers may blunt immunotherapy response — an active and consequential controversy, since some analyses suggest immunotherapy works less well in non-viral HCC.
12. References & Research
Historical Background
The modern story of liver cancer begins with Baruch Blumberg's 1965 discovery of the “Australia antigen” — the surface protein of the hepatitis B virus — which earned him the 1976 Nobel Prize in Physiology or Medicine and revealed the virus behind most of the world's liver cancer. The first hepatitis B vaccine, approved in 1981, became in effect the world's first cancer-prevention vaccine; Taiwan's universal newborn vaccination program, launched in 1984, later provided direct proof that vaccinating against a virus prevents a human cancer. In 1996, Vincenzo Mazzaferro's Milan group published the criteria that made liver transplantation a standard curative therapy for early HCC. The 2008 SHARP trial of sorafenib delivered the first effective systemic drug for advanced disease after decades of failed chemotherapy, and the 2020 IMbrave150 trial of atezolizumab plus bevacizumab opened the immunotherapy era — the first regimen to outperform sorafenib and the new foundation of advanced-stage treatment.
Key Research Papers
- Finn RS, et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma (IMbrave150). New England Journal of Medicine. 2020;382(20):1894-1905.
- Llovet JM, et al. Sorafenib in advanced hepatocellular carcinoma (SHARP). New England Journal of Medicine. 2008;359(4):378-390.
- Mazzaferro V, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis (Milan criteria). New England Journal of Medicine. 1996;334(11):693-700.
- Llovet JM, et al. Hepatocellular carcinoma. Nature Reviews Disease Primers. 2021;7(1):6.
- Singal AG, et al. AASLD Practice Guidance on prevention, diagnosis, and treatment of hepatocellular carcinoma. Hepatology. 2023;78(6):1922-1965.
- Abou-Alfa GK, et al. Tremelimumab plus durvalumab in unresectable hepatocellular carcinoma (HIMALAYA). NEJM Evidence. 2022;1(8):EVIDoa2100070.
- Kudo M, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma (REFLECT). Lancet. 2018;391(10126):1163-1173.
- Kanwal F, et al. Risk of hepatocellular cancer in HCV patients treated with direct-acting antiviral agents. Gastroenterology. 2017;153(4):996-1005.
- Singal AG, Pillai A, Tiro J. Early detection, curative treatment, and survival rates for hepatocellular carcinoma surveillance in patients with cirrhosis: a meta-analysis. PLoS Medicine. 2014;11(4):e1001624.
- Chang MH, et al. Universal hepatitis B vaccination in Taiwan and the incidence of hepatocellular carcinoma in children. New England Journal of Medicine. 1997;336(26):1855-1859.
- Huang DQ, El-Serag HB, Loomba R. Global epidemiology of NAFLD-related HCC: trends, predictions, risk factors and prevention. Nature Reviews Gastroenterology & Hepatology. 2021;18(4):223-238.
- Reig M, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. Journal of Hepatology. 2022;76(3):681-693.
- Kennedy OJ, et al. Coffee, including caffeinated and decaffeinated coffee, and the risk of hepatocellular carcinoma: a systematic review and dose-response meta-analysis. BMJ Open. 2017;7(5):e013739.
- El-Serag HB. Hepatocellular carcinoma. New England Journal of Medicine. 2011;365(12):1118-1127.
Research Papers
The following PubMed topic searches surface the current peer-reviewed literature on Liver Cancer. Each link opens a live PubMed query; results update as new papers are indexed.
- PubMed search: hepatocellular carcinoma
- PubMed search: hepatocellular carcinoma surveillance cirrhosis
- PubMed search: hepatocellular carcinoma NAFLD MASLD
- PubMed search: hepatitis B hepatocellular carcinoma prevention
- PubMed search: hepatitis C direct-acting antivirals HCC risk
- PubMed search: liver transplantation Milan criteria
- PubMed search: hepatocellular carcinoma radiofrequency ablation
- PubMed search: transarterial chemoembolization TACE
- PubMed search: atezolizumab bevacizumab hepatocellular carcinoma
- PubMed search: durvalumab tremelimumab hepatocellular carcinoma
- PubMed search: coffee hepatocellular carcinoma risk
- PubMed search: LI-RADS hepatocellular carcinoma diagnosis
Connections
- Cancer Overview
- Metastatic Cancers
- Cirrhosis
- Liver Disease
- Non-Alcoholic Fatty Liver Disease
- Hepatitis
- Hepatitis B
- Hepatitis C
- Hemochromatosis
- Diabetes
- Obesity
- Addiction
- Jaundice
- Coffee
- Coffee and Cancer Prevention
- Milk Thistle
- Hepatocellular Carcinoma — the dominant subtype, accounting for about 90% of primary liver cancers; covered in depth on its own page.