Ventricular Tachycardia
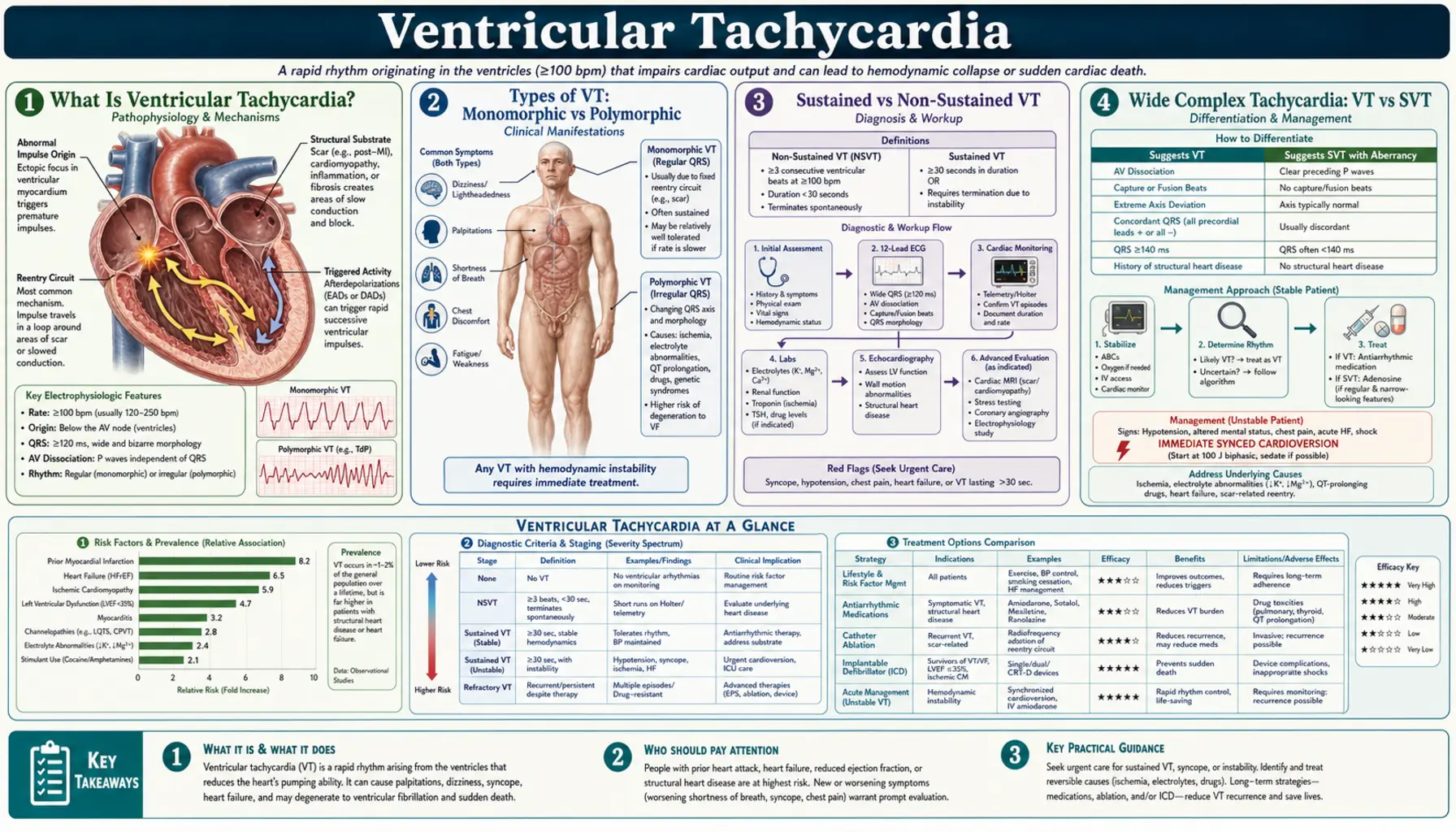
Table of Contents
- What Is Ventricular Tachycardia?
- Types of VT: Monomorphic vs Polymorphic
- Sustained vs Non-Sustained VT
- Wide Complex Tachycardia: VT vs SVT
- Causes and Underlying Conditions
- Acute Management: Stable and Unstable VT
- Long-Term Treatment: ICD and Catheter Ablation
- ICD for Primary and Secondary Prevention
- Special Syndromes: Long-QT, Brugada, and CPVT
- Research Papers
- Connections
- Featured Videos
What Is Ventricular Tachycardia?
Ventricular tachycardia (VT) is a fast heart rhythm (≥3 consecutive beats at rate ≥100–120 bpm) that originates in the ventricles rather than the normal pacemaker system. Because the electrical signal starts in the muscular walls of the ventricles and spreads abnormally, each beat looks wide and distorted on the ECG — the QRS complex is typically >120 milliseconds — and the heart pumps less efficiently.
VT ranges from brief, asymptomatic runs that most people never know about, to life-threatening sustained rhythms that can cause cardiac arrest within minutes. Understanding VT requires knowing its two critical dimensions: morphology (what does each beat look like?) and duration (how long does the episode last?). These two axes together determine risk and treatment.
Types of VT: Monomorphic vs Polymorphic
The shape of the QRS complex on the ECG is the first and most important diagnostic split:
Monomorphic VT
Every beat has the same QRS shape — each one looks identical to the last. This uniformity means a single, stable re-entry circuit is firing repeatedly from the same anatomical location. The most common setting is scar tissue from a prior heart attack (myocardial infarction). Scar does not conduct electricity; healthy tissue bordering the scar creates a slow conduction corridor (isthmus) that allows the electrical impulse to circle continuously. This is called scar-related re-entry.
Monomorphic VT also occurs in non-ischemic cardiomyopathies (dilated, hypertrophic, arrhythmogenic right ventricular cardiomyopathy/ARVC), sarcoidosis, and Chagas disease — wherever myocardial fibrosis creates anatomical substrate for re-entry.
Polymorphic VT
The QRS morphology changes beat to beat — each one looks different. This means the activation sequence is constantly shifting, which signals a more unstable and dangerous process. Common causes include:
- Acute ischemia — ongoing myocardial infarction is the most common cause of polymorphic VT in adults; ischemia disrupts ion channel function throughout the ventricle in a heterogeneous pattern.
- Long-QT syndrome (LQTS) — prolonged repolarization creates a substrate for a specific form of polymorphic VT called torsades de pointes (TdP), in which the QRS axis twists around the isoelectric line. Causes include congenital ion channel mutations (LQT1, LQT2, LQT3) and many drugs (antiarrhythmics, antibiotics, antipsychotics, antiemetics).
- Catecholaminergic polymorphic VT (CPVT) — a rare inherited disorder (RYR2 or CASQ2 mutations) in which exercise or emotional stress triggers adrenergic-mediated polymorphic VT. The resting ECG and echo are normal; the diagnosis requires exercise testing.
- Brugada syndrome — an inherited sodium channel abnormality (SCN5A) that typically causes VF or polymorphic VT at rest or during fever, with a characteristic coved ST-elevation in leads V1–V2 on ECG.
- Hypokalemia and hypomagnesemia — electrolyte deficiencies prolong the QT interval and predispose to TdP.
Sustained vs Non-Sustained VT
Duration determines urgency:
- Non-sustained VT (NSVT) — defined as ≥3 consecutive ventricular beats at ≥100 bpm that terminate spontaneously in less than 30 seconds without causing hemodynamic collapse. NSVT is common and often detected incidentally on Holter monitors. In patients without structural heart disease, isolated NSVT is generally benign. In patients with reduced ejection fraction or significant cardiomyopathy, NSVT is a marker of increased sudden cardiac death risk and warrants further evaluation (often electrophysiology study).
- Sustained VT — lasts 30 seconds or longer, or terminates sooner only because of hemodynamic deterioration requiring intervention. Sustained VT demands immediate assessment and treatment. Even if the patient appears stable, sustained VT can degenerate into ventricular fibrillation (VF) without warning.
A practical clinical concept is hemodynamic stability: a patient in VT who is alert, maintaining blood pressure, and has preserved peripheral perfusion is "stable VT" and can be treated with medications first. A patient in VT who is unconscious, hypotensive, or showing signs of cardiogenic shock is "unstable" and requires immediate electrical cardioversion — drug therapy would waste critical time.
Wide Complex Tachycardia: VT vs SVT
A wide QRS tachycardia (QRS >120 ms at rate >100 bpm) has two main possibilities: ventricular tachycardia, or supraventricular tachycardia (SVT) with aberrant conduction (e.g., SVT conducting down a bundle branch block or accessory pathway). Getting this distinction right is critical — some SVT treatments (adenosine, verapamil) can cause cardiovascular collapse in VT.
The Brugada Criteria (1991)
Jose Brugada and colleagues described a four-step algorithm for wide complex tachycardia. A "yes" answer at any step diagnoses VT:
- Is there an absence of RS complexes in all precordial leads (V1–V6)?
- Is the R-to-S interval >100 ms in any precordial lead?
- Is there atrioventricular dissociation (P waves and QRS complexes firing independently)?
- Are there morphological criteria for VT in V1 and V6? (e.g., in LBBB-pattern tachycardia: Q wave in V6; in RBBB-pattern: monophasic R or Rr' in V1 + QS or rS in V6)
The Brugada criteria have ~98% sensitivity for VT when all four are systematically applied.
The Vereckei Algorithm (2008)
The Vereckei aVR algorithm uses only lead aVR — particularly useful when precordial leads are noisy. A "yes" at any step diagnoses VT:
- Is there an initial R wave in aVR?
- Is the initial r or q wave >40 ms in aVR?
- Is there a notch on the descending limb of a predominantly negative (QS or QR) complex in aVR?
- Is vi/vt ≤1? (ratio of initial to terminal deflection velocity)
A useful clinical rule: "If in doubt, treat as VT." VT is far more common than SVT-aberrancy in patients with structural heart disease; treating VT as SVT can be fatal, while the reverse mistake is rarely catastrophic.
Signs strongly suggesting VT rather than SVT: AV dissociation (independent P waves — "capture beats" and "fusion beats"), concordance (all precordial QRS complexes pointing the same direction), extreme axis deviation, and a QRS morphology that does not match any typical bundle branch block pattern.
Causes and Underlying Conditions
VT rarely arises in a normal heart. The substrate is nearly always some form of structural or electrical disease:
- Ischemic cardiomyopathy — prior MI with scar tissue is the most common substrate for monomorphic VT in the developed world. Risk is highest in the first year post-MI, especially with EF <40%.
- Non-ischemic dilated cardiomyopathy — fibrosis from genetic, viral, alcoholic, or idiopathic causes creates re-entry substrate.
- Hypertrophic cardiomyopathy (HCM) — disorganized myofibril arrangement and bridging fibrosis; a leading cause of sudden death in young athletes.
- Arrhythmogenic right ventricular cardiomyopathy (ARVC) — fatty and fibrous infiltration of the right ventricle (desmosome mutations); exercise-triggered VT is the presentation; "epsilon wave" on ECG is a clue.
- Acute myocardial infarction — the primary cause of polymorphic VT and VF in the acute setting; revascularization is the most important treatment.
- Electrolyte disorders — hypokalemia (<3.0 mEq/L), hypomagnesemia, and hypocalcemia all prolong repolarization and lower the threshold for VT.
- Drug-induced QT prolongation — a long list of common medications causes acquired long-QT syndrome: sotalol, dofetilide, amiodarone (paradoxically rarely causes TdP), azithromycin, haloperidol, ondansetron, methadone.
- Idiopathic VT — a minority of VTs have no structural substrate. The most common forms are right ventricular outflow tract (RVOT) VT (adenosine-sensitive, typically benign) and fascicular VT (verapamil-sensitive).
Acute Management: Stable and Unstable VT
The first decision in acute VT management is whether the patient is hemodynamically stable or unstable.
Unstable VT: DC Cardioversion
If the patient has altered consciousness, systolic BP <80 mmHg, signs of pulmonary edema, or active chest pain from the arrhythmia: immediate synchronized DC cardioversion. Do not delay with drug therapy. Deliver 100–200 joules biphasic. If VT is pulseless (i.e., VF or pulseless VT), unsynchronized defibrillation is required — this is a cardiac arrest requiring CPR and ACLS protocols.
Stable Monomorphic VT: Antiarrhythmic Drugs
For hemodynamically stable, sustained monomorphic VT, two first-line intravenous antiarrhythmics are used in the United States:
- Amiodarone IV — loading dose 150 mg over 10 minutes, followed by 1 mg/min infusion for 6 hours. The most commonly used agent; effective across many VT types; does not significantly lower blood pressure at standard doses. Note: IV amiodarone rarely terminates VT acutely — it stabilizes the rhythm and prevents recurrence. Chronic oral amiodarone causes significant toxicity (thyroid, lung, liver, peripheral neuropathy) but is unmatched for efficacy.
- Procainamide IV — loading 20–50 mg/min (max 17 mg/kg) then maintenance infusion. May actually terminate VT more reliably than amiodarone in the acute setting. Preferred by some electrophysiologists; requires QRS and QTc monitoring. A 2014 Cochrane analysis found procainamide superior to amiodarone for acute VT conversion to sinus rhythm.
Lidocaine IV is a third option, less commonly used than previously for VT because it is less effective, but still useful in acute ischemic VT where its sodium-channel block is well-suited to the ischemic mechanism.
Polymorphic VT and Torsades de Pointes
Polymorphic VT treatment depends on the underlying cause:
- Acute ischemia — emergent revascularization (PCI or thrombolysis) is the definitive treatment; amiodarone IV as a bridge.
- Torsades de pointes (acquired long-QT) — IV magnesium sulfate 2 g over 5 minutes is first-line. Correct hypokalemia to K⁺ >4.5 mEq/L. Discontinue all QT-prolonging drugs. Temporary pacing at 90–110 bpm (overdrive pacing) shortens the QT by increasing heart rate and suppresses TdP.
- Congenital long-QT — IV beta-blockers (propranolol or esmolol); avoid isoproterenol in LQT3.
- CPVT storm — IV propranolol; if refractory, flecainide can reduce RYR2-mediated calcium leak.
Long-Term Treatment: ICD and Catheter Ablation
Acute termination of VT does not address the underlying substrate. Long-term management prevents future episodes and sudden death.
Catheter Ablation for Recurrent Scar-Related VT
In patients with recurrent monomorphic VT from scar-related re-entry, catheter ablation maps the re-entry circuit and delivers radiofrequency energy to eliminate the critical isthmus within the scar. Modern three-dimensional electroanatomic mapping (Carto, EnSite) allows precise identification of scar borders, low-voltage zones, and late potentials.
The VTACH trial (2010) and SMASH-VT trial (2007) showed that ablation performed after a first VT episode reduced VT recurrence by ~50% compared to ICD therapy alone. The VANISH trial (2016) found that ablation was superior to escalated antiarrhythmic drug therapy in reducing the composite of death, VT storm, or ICD shock in patients already failing amiodarone. Ablation does not replace an ICD but substantially reduces ICD shock burden and improves quality of life.
Antiarrhythmic Drugs for VT Suppression
- Amiodarone — most effective oral agent for suppressing recurrent VT; often combined with ICD to reduce shock frequency.
- Sotalol — beta-blocker plus class III potassium channel block; effective for VT but proarrhythmic (TdP risk ~3–5%); requires renal dosing.
- Beta-blockers — first-line for CPVT and useful adjunct in ischemic VT; not adequate as sole therapy for recurrent sustained VT.
- Mexiletine — oral sodium channel blocker; used as adjunct to amiodarone in refractory VT, particularly in LQT3.
ICD for Primary and Secondary Prevention
The implantable cardioverter-defibrillator (ICD) is the most effective therapy for preventing sudden cardiac death from VT/VF.
Secondary Prevention (after VT/VF arrest)
Patients who survive a cardiac arrest or sustained VT without a reversible cause have a high risk of recurrence. The AVID, CIDS, and CASH trials (late 1990s) established ICD superiority over antiarrhythmic drugs (mainly amiodarone) for secondary prevention, with a 20–31% relative reduction in total mortality.
Primary Prevention — MADIT-II
The MADIT-II trial (NEJM 2002, N=1,232) enrolled patients with prior MI and EF ≤30% with no history of sustained VT. Prophylactic ICD implantation reduced all-cause mortality by 31% (HR 0.69, p=0.016) compared with conventional medical therapy over 20 months. This trial established the principle that patients do not need to have had VT to benefit from an ICD.
Primary Prevention — SCD-HeFT
The SCD-HeFT trial (NEJM 2005, N=2,521) enrolled patients with EF ≤35% from both ischemic and non-ischemic cardiomyopathy, all in NYHA Class II–III. ICD therapy reduced all-cause mortality by 23% (HR 0.77, p=0.007) vs placebo over a median of 45.5 months. Amiodarone showed no mortality benefit vs placebo. SCD-HeFT extended ICD benefit to non-ischemic cardiomyopathy and confirmed the EF ≤35% threshold used in current guidelines.
Current ICD Indications (simplified)
- EF ≤35% despite optimal medical therapy for ≥3 months, NYHA Class II or III, and expected survival >1 year (Class I recommendation)
- Survivors of VF or hemodynamically unstable VT without reversible cause
- Syncope of suspected VT etiology in structural heart disease
- Brugada syndrome with prior cardiac arrest or spontaneous sustained VT
- CPVT with prior cardiac arrest or syncope
Special Syndromes: Long-QT, Brugada, and CPVT
Congenital Long-QT Syndrome (LQTS)
Congenital LQTS is caused by mutations in cardiac ion channels that delay ventricular repolarization. QTc >460 ms in women and >440 ms in men raises suspicion; QTc >500 ms is high risk. The three commonest subtypes are LQT1 (KCNQ1, triggered by exercise/swimming), LQT2 (KCNH2, triggered by sudden sounds/startle), and LQT3 (SCN5A, triggered at rest/sleep). Treatment: beta-blockers for LQT1 and LQT2; mexiletine ± beta-blockers for LQT3; left cardiac sympathetic denervation for drug-refractory cases.
Brugada Syndrome
Brugada syndrome is caused by loss-of-function mutations in SCN5A (in ~20% of cases; others unknown) producing a characteristic Type 1 Brugada ECG pattern (coved ST elevation ≥2 mm in V1–V2). Risk stratification is imperfect; patients with prior cardiac arrest or spontaneous Type 1 pattern are highest risk. ICD is the only proven therapy for high-risk Brugada; quinidine may reduce VF burden. Fever can unmask the pattern and trigger arrhythmias — patients must treat fever aggressively.
Catecholaminergic Polymorphic VT (CPVT)
CPVT is caused by mutations (RYR2, CASQ2) that lead to pathological calcium release from the sarcoplasmic reticulum during adrenergic stimulation. Exercise provokes bidirectional or polymorphic VT in an otherwise normal heart. First-line therapy: nadolol (preferred over metoprolol for its non-selective beta-blockade). Flecainide reduces calcium leak directly and is added if beta-blockers alone are insufficient. Exercise restriction is mandatory; ICD is used in high-risk patients but inappropriate shocks can trigger catecholamine surges that worsen VT — programming must be careful.
Research Papers
The following citations are from published peer-reviewed literature on ventricular tachycardia. PubMed links open the specific article.
- Search PubMed (MADIT-II: ICD primary prevention post-MI EF ≤30%)
- Bardy GH et al., 2005 — PMID: 15659722 (SCD-HeFT: ICD vs amiodarone EF ≤35%)
- Search PubMed (VANISH: ablation vs escalated antiarrhythmic drugs for VT)
- Search PubMed (VTACH trial: ablation reduces VT recurrence)
- Search PubMed (SMASH-VT: prophylactic ablation after MI)
- Search PubMed (Brugada criteria for wide complex tachycardia)
- Search PubMed (Vereckei aVR algorithm for VT diagnosis)
- Search PubMed (ICD vs antiarrhythmics for secondary prevention)
- Search PubMed (Congenital long-QT syndrome classification and outcomes)
- Search PubMed (CPVT: flecainide reduces exercise-induced arrhythmias)
- Search PubMed (Systematic review: procainamide vs amiodarone acute VT)
- Search PubMed (AHA/ACC ventricular arrhythmia guideline)
Connections
- Cardiology
- Arrhythmia
- Atrial Fibrillation
- Heart Failure
- Coronary Artery Disease
- Cardiomyopathy
- Cardiovascular Disease
- HFpEF
- Cardiac Tamponade
- Myocardial Infarction
- Valvular Heart Disease
- Magnesium
- Potassium