Methylene Blue: From 19th-Century Dye to Mitochondrial Nootropic
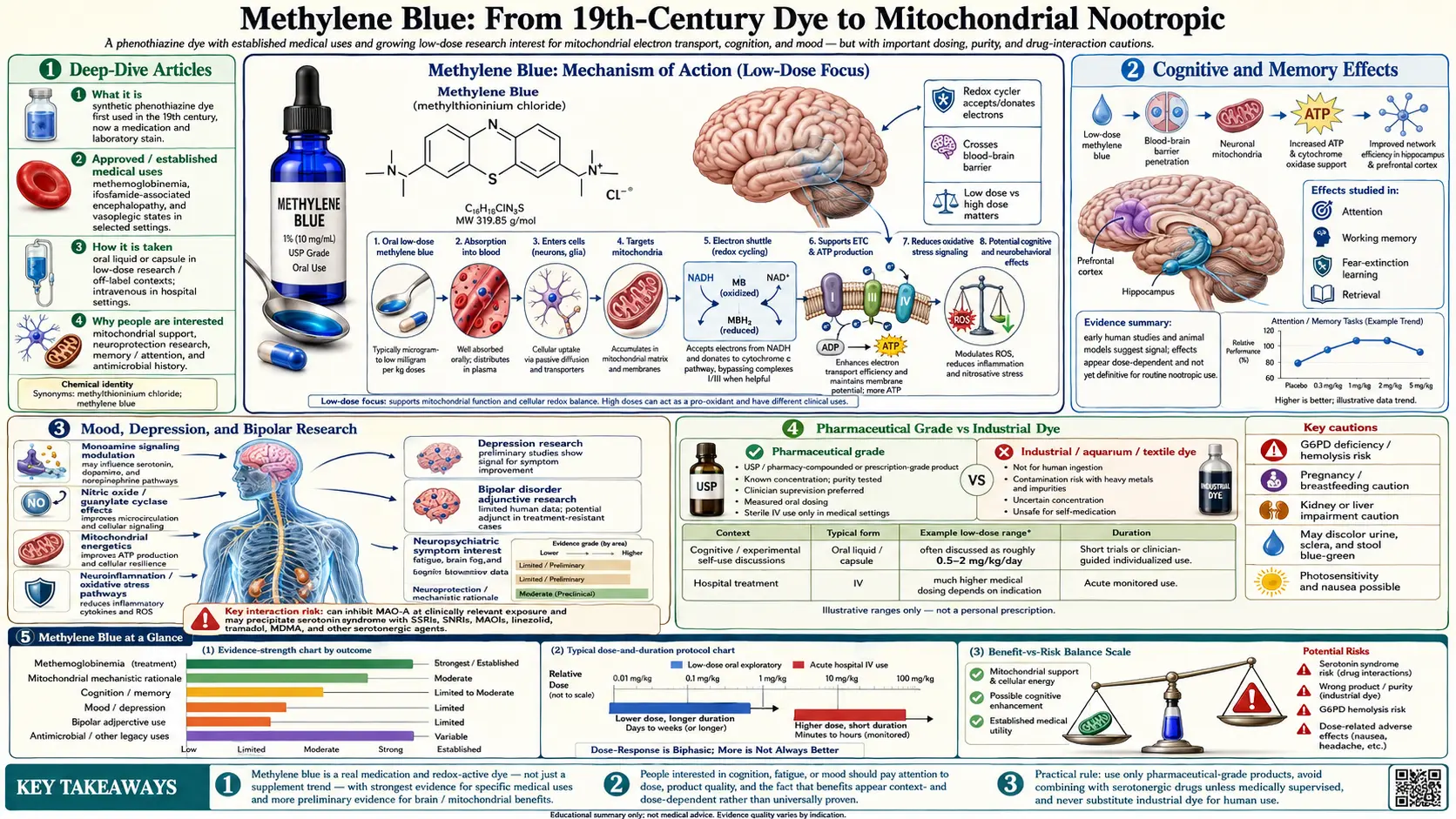
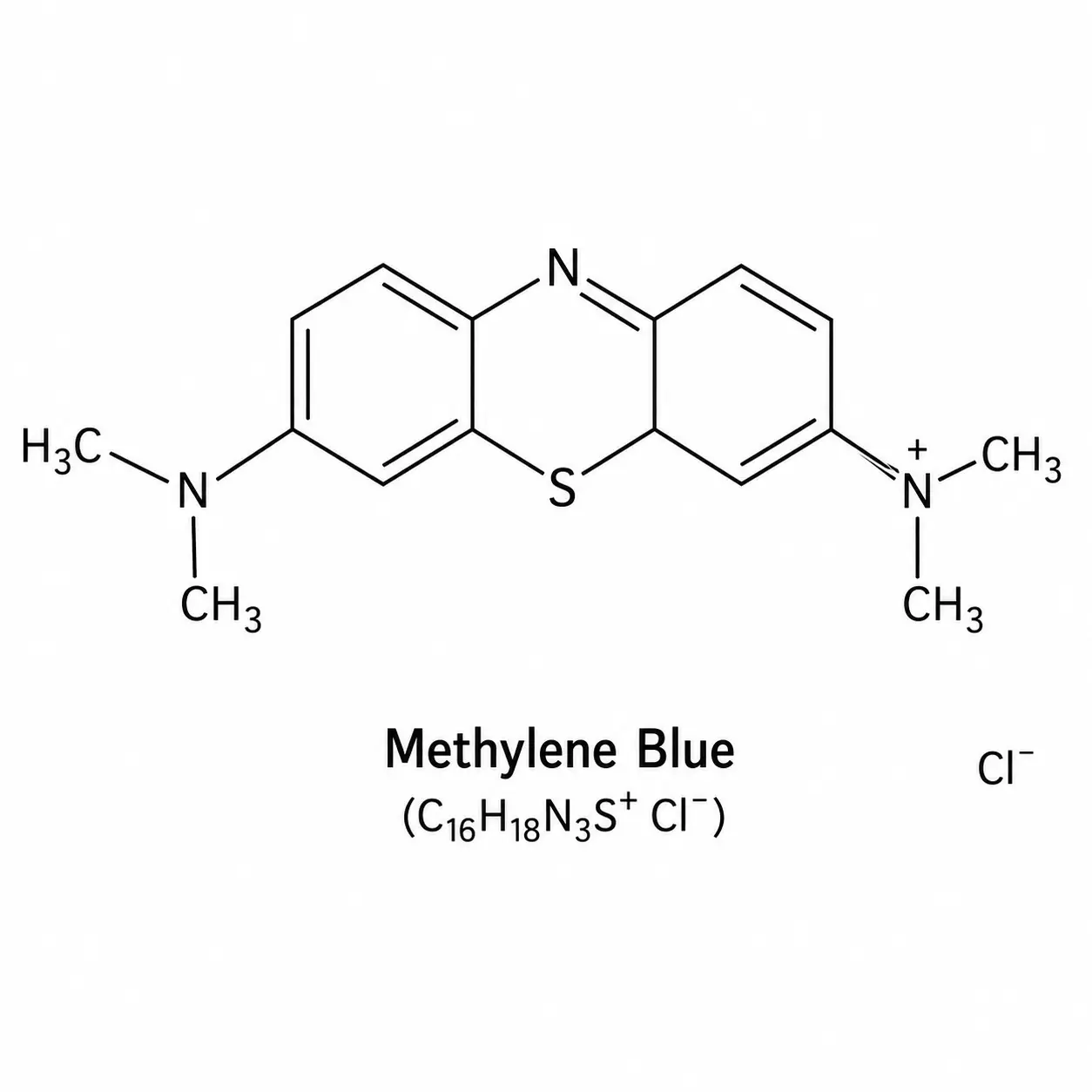
Methylene blue (methylthioninium chloride) is one of the oldest synthetic drugs in continuous medical use — first synthesized in 1876 as a textile dye, it became the prototype for every subsequent phenothiazine-class psychiatric medication and remains today a standard treatment for methemoglobinemia and certain cyanide poisonings. Over the past two decades, a quiet but substantial body of research has explored methylene blue at much lower doses for its effects on mitochondrial function, memory, mood, and neurodegenerative disease. These uses are off-label and the pharmaceutical-grade formulation differs significantly in purity from the industrial-grade dye that shares the same name; this distinction is not trivial.
This article covers the mechanisms, evidence, safety profile, and practical considerations for methylene blue as a cognitive and metabolic tool. It is educational and not a substitute for individualized medical advice.
Deep-Dive Articles
Methylene blue is unusual: a 19th-century textile dye that became the world's first synthetic drug, the prototype for every modern phenothiazine, an emergency antidote, and now an off-label cognitive and longevity tool. The nine articles below break it apart by topic so you can find the piece you actually need — the bioenergetics, the dosing, the off-label uses, the very real safety pitfalls, the medication interactions, and the difference between USP-grade pharmaceutical methylene blue and the industrial dye sold from chemistry suppliers.
Mitochondrial Mechanism & Bioenergetics
How methylene blue accepts electrons from NADH and bypasses Complexes I and III in the electron transport chain, restoring ATP and lowering ROS in dysfunctional mitochondria. The hormetic bell curve, the role of cytochrome c, and why low doses help while high doses harm.
Dosing Guide (mg/kg, Oral, Sublingual, IV)
Nootropic doses (0.5–4 mg/kg), neuroprotective doses, FDA-approved dosing for methemoglobinemia, oral vs sublingual vs IV pharmacokinetics, peak times, the vitamin C interaction, and why the bell-shaped dose-response makes "more" the wrong instinct.
Cognitive Enhancement & ADHD
The Rodriguez 2016 functional MRI study, working memory and sustained attention data, the off-label ADHD interest, brain fog applications, dose-response curves for cognition, and the realistic expectation gap between mouse studies and human effects.
Methylene Blue & Long COVID
Why post-viral fatigue and long COVID share a mitochondrial-dysfunction signature, the small case-series and mechanistic basis for methylene blue protocols, current clinical-trial activity, dosing patterns clinicians have published, and the unresolved questions.
Drug Interactions & Serotonin Syndrome
The single most important safety topic. SSRIs, SNRIs, MAOIs, tramadol, fentanyl, dextromethorphan, lithium, triptans, even St. John's Wort. The MAO-A inhibition mechanism, the FDA black-box warning, the washout periods, and what serotonin syndrome actually looks like.
Methemoglobinemia & G6PD Deficiency
The paradox: methylene blue is the antidote for methemoglobinemia at therapeutic doses but causes it at higher doses. Why G6PD-deficient patients can have severe hemolysis. Pre-screening recommendations and what to do if you don't know your G6PD status.
Photodynamic Therapy & Cancer Research
Methylene blue + red light = singlet oxygen. Approved photodynamic uses (Barrett's esophagus, basal cell carcinoma, antimicrobial PDT for periodontal disease), the ongoing oncology research, and why this is the most legitimate cancer-adjacent use of methylene blue.
Pharmaceutical Grade vs Industrial Dye
The contaminant problem nobody warns you about. USP grade vs ChemDye / lab-grade. Heavy-metal residues, organic byproducts. The brands clinicians use, the third-party testing question, blue tongue and urine, and the 2024 FDA enforcement actions on grey-market sellers.
History: Ehrlich, Malaria, & the Phenothiazine Revolution
From a German textile dye in 1876 to Paul Ehrlich's "magic bullet" malaria experiments, to chlorpromazine and the entire modern psychiatric drug class that descended from this single molecule. The clearest example in pharmacology of how one chemical reshaped medicine.
Table of Contents
- Deep-Dive Articles
- History and Approved Uses
- Historical Medical Use (1926)
- Mechanism — The Electron-Transport Bypass
- Cognitive and Memory Effects
- Alzheimer’s and Neurodegenerative Research
- Mood, Depression, and Bipolar Research
- Practical Dosing and Formulation
- Risks and Drug Interactions
- Pharmaceutical Grade vs Industrial Dye
- Connections
- Featured Videos
History and Approved Uses
Methylene blue is widely described as the first fully synthetic drug used in medicine: first prepared as a textile dye by Heinrich Caro in 1876, it crossed into the clinic when Paul Ehrlich and Paul Guttmann tested it against malaria in 1891. FDA-approved uses today include acute methemoglobinemia, ifosfamide-induced encephalopathy, and use as a surgical dye. — the fuller story is told in the dedicated History & Discovery article.
Historical Medical Use (1926 U.S. Dispensatory)
By the time the United States Dispensatory (21st edition, 1926) was the standard American drug reference, methylene blue had already had a fifty-year career — remarkable for a compound that began life in 1876 as a synthetic textile dye. It is genuinely one of the first fully synthetic medicines, and its tricyclic phenothiazine core is a distinct chemical structure, not one of the simpler azo dyes that color most fabrics and foods. That structural backbone is the same one later built into chlorpromazine and the whole family of antipsychotic drugs, which is why methylene blue is often called the grandparent of modern psychiatric medicine.
The medical claims of that era, presented here strictly as history, were broad. Physicians experimented with methylene blue to try to shrink tumors, and used it for meningitis, bladder (urinary tract) infections, and gonorrhea — all in a pre-antibiotic world where a cheap dye that stained and was thought to be mildly antiseptic was one of the few tools available. A century later, methylene blue is again in the spotlight, this time for mitochondrial and neurological support, the focus of much of this page.
Each of those 1926 claims has to be read against what modern evidence actually shows. It is not a cancer cure — there is no clinical evidence that ingesting or injecting methylene blue treats or shrinks tumors, and presenting it as a cancer therapy is dangerous. (The one legitimate oncology-adjacent role is photodynamic therapy, where methylene blue is activated by red light to generate singlet oxygen in a tightly controlled clinical setting; see the Photodynamic Therapy & Cancer Research article.) Likewise, methylene blue is not a treatment for meningitis, bladder infections, or gonorrhea today — those are bacterial infections that require proper antibiotics, and self-treating them with a dye risks letting a serious infection progress. Its proven, accepted modern uses are narrow: it is the standard antidote for acquired methemoglobinemia, a treatment for ifosfamide-induced encephalopathy, a surgical and diagnostic tissue stain, and a rescue therapy for vasoplegic syndrome (dangerously low vascular tone, often after cardiac surgery). The low-dose mitochondrial and neurocognitive uses driving the current resurgence are scientifically interesting and biologically plausible, but they remain investigational — promising research, not settled medicine.
One safety point the popular "revival" coverage tends to skip deserves repeating up front (it is detailed in the Risks and Drug Interactions section below). Methylene blue is a potent monoamine oxidase inhibitor (MAOI), so combining it with SSRIs, SNRIs, or other serotonergic drugs can trigger life-threatening serotonin syndrome. It can cause dangerous hemolysis in people with G6PD deficiency. At high doses it paradoxically causes the very methemoglobinemia it treats at low doses. And only pharmaceutical-grade (USP) methylene blue is fit for human use — the aquarium, textile, and industrial-grade dye sold under the same name can carry heavy-metal and chemical contaminants and must never be ingested.
Mechanism — The Electron-Transport Bypass
In the mitochondrial electron transport chain, methylene blue acts as an alternative electron carrier, accepting electrons from NADH and shuttling them directly to cytochrome c, thereby bypassing partially dysfunctional Complexes I and III. In cells with compromised mitochondrial function — seen in aging, neurodegeneration, and stroke — this can restore ATP production and reduce the reactive oxygen species (ROS) that leak from a sluggish chain. At higher doses, methylene blue becomes a pro-oxidant, illustrating the bell-shaped hormetic dose curve that dominates its pharmacology: low doses help, high doses harm.
Methylene blue also inhibits monoamine oxidase A (MAO-A) at clinically relevant concentrations. This accounts for both its mood effects and its most dangerous interaction (with serotonergic drugs, discussed below). It inhibits nitric oxide synthase and guanylate cyclase, which is why it is used in vasoplegic shock to restore vascular tone. It has been shown to reduce aggregation of the tau protein implicated in Alzheimer’s disease.
Cognitive and Memory Effects
A placebo-controlled functional-MRI study by Rodriguez et al. (2016) showed a single low dose (280 mg oral) of methylene blue increased response accuracy on a sustained-attention task and enhanced activation in memory-related brain regions. Animal studies consistently show improved learning and memory, effects tied to enhanced cytochrome oxidase activity in mnemonic circuits. Self-reported nootropic effects include improved focus, mild mood elevation, and enhanced verbal fluency — all at doses far below therapeutic ranges for methemoglobinemia.
Alzheimer’s and Neurodegenerative Research
Methylene blue and its derivative LMTX (leuco-methylthioninium) have been studied in Alzheimer’s disease based on their ability to inhibit tau aggregation. Phase-3 trials have produced mixed results: the drug failed to meet primary endpoints but showed potentially meaningful effects in monotherapy subgroups. Research continues in frontotemporal dementia and Parkinson’s disease, where mitochondrial dysfunction is central.
Mood, Depression, and Bipolar Research
Small trials of methylene blue in bipolar depression have suggested a possible augmentation effect when added to a mood stabilizer. Its MAO-A inhibition and mitochondrial effects are both plausible mechanisms. Because of the serotonin-syndrome risk, use in depression is not compatible with most standard antidepressants.
Practical Dosing and Formulation
Nootropic and anti-aging protocols commonly use 0.5 mg to 4 mg per kilogram body weight per day, or fixed doses of 10–50 mg. Higher doses (>5 mg/kg) cross into pro-oxidant territory and can paradoxically worsen mitochondrial stress. Methylene blue is bitter and stains everything it touches — including tongue, teeth, and urine (fluorescent blue-green urine is a benign expected side effect). Solutions are typically taken orally diluted in water; sublingual delivery improves absorption but amplifies staining of mucous membranes.
Risks and Drug Interactions
- Serotonin syndrome. Methylene blue is a potent MAO-A inhibitor. Combining it with SSRIs, SNRIs, tricyclics, tramadol, MDMA, or other serotonergic agents can produce life-threatening serotonin syndrome. The FDA issued an explicit warning in 2011.
- G6PD deficiency. Methylene blue can precipitate hemolytic anemia in people with glucose-6-phosphate dehydrogenase deficiency.
- Pregnancy. Contraindicated.
- Pro-oxidant range. High doses reverse the benefit.
- Blue discoloration. Of skin, urine, sweat, and tears — benign but surprising.
Pharmaceutical Grade vs Industrial Dye
This distinction is life-or-death. Industrial-grade methylene blue used for aquariums, textile dyeing, and laboratory staining frequently contains heavy-metal contaminants (arsenic, mercury, lead) and impurities that are irrelevant for staining fabric but unacceptable for human ingestion. Only USP-grade or pharmacopoeia-grade methylene blue, prepared by a compounding pharmacy or an FDA-registered manufacturer, is appropriate for medicinal use. The price difference is not large; the quality difference is.
Key Research Papers
Foundational and recent peer-reviewed publications on methylene blue, covering mitochondrial bioenergetics, cognitive enhancement, neurodegenerative disease, methemoglobinemia, and the MAO-A/serotonin-syndrome safety axis. Each citation links to the full text via DOI.
- Atamna H, Nguyen A, Schultz C, et al. Methylene Blue Delays Cellular Senescence and Enhances Key Mitochondrial Biochemical Pathways. FASEB Journal. 2008;22(3):703–712.
- Rojas JC, Bruchey AK, Gonzalez-Lima F. Neurometabolic Mechanisms for Memory Enhancement and Neuroprotection of Methylene Blue. Progress in Neurobiology. 2012;96(1):32–45.
- Wainwright M, Crossley KB. Methylene Blue—A Therapeutic Dye for All Seasons? Journal of Chemotherapy. 2002;14(5):431–443.
- Oz M, Lorke DE, Petroianu GA. Methylene Blue and Alzheimer's Disease. Biochemical Pharmacology. 2009;78(8):927–932. (Reviews methylene blue's history as one of the first synthetic drugs and its century of changing medical uses.)
- Schirmer RH, Adler H, Pickhardt M, Mandelkow E. "Lest We Forget You—Methylene Blue…". Neurobiology of Aging. 2011;32(12):2325.e7–2325.e16.
- Bistas E, Sanghavi DK. Methylene Blue. StatPearls Publishing. Updated 2023.
- Wischik CM, Staff RT, Wischik DJ, et al. Tau Aggregation Inhibitor Therapy: An Exploratory Phase 2 Study in Mild or Moderate Alzheimer's Disease. Journal of Alzheimer's Disease. 2015;44(2):705–720.
- Rodriguez P, Zhou W, Barrett DW, et al. Multimodal Randomized Functional MR Imaging of the Effects of Methylene Blue in the Human Brain. Radiology. 2016;281(2):516–526.
- Ramsay RR, Dunford C, Gillman PK. Methylene Blue and Serotonin Toxicity: Inhibition of Monoamine Oxidase A (MAO A) Confirms a Theoretical Prediction. British Journal of Pharmacology. 2007;152(6):946–951.
- Wendel WB. The Control of Methemoglobinemia with Methylene Blue. Journal of Clinical Investigation. 1939;18(2):179–185.
- Beutler E. G6PD Deficiency. Blood. 1994;84(11):3613–3636.
- Tucker D, Lu Y, Zhang Q. From Mitochondrial Function to Neuroprotection—An Emerging Role for Methylene Blue. Molecular Neurobiology. 2018;55(6):5137–5153.
- Riha PD, Bruchey AK, Echevarria DJ, Gonzalez-Lima F. Memory Facilitation by Methylene Blue: Dose-Dependent Effect on Behavior and Brain Oxygen Consumption. European Journal of Pharmacology. 2005;511(2–3):151–158.
- Callaway NL, Riha PD, Bruchey AK, Munshi Z, Gonzalez-Lima F. Methylene Blue Improves Brain Oxidative Metabolism and Memory Retention in Rats. Pharmacology Biochemistry and Behavior. 2004;77(1):175–181.
- Poteet E, Winters A, Yan LJ, et al. Neuroprotective Actions of Methylene Blue and Its Derivatives. PLoS ONE. 2012;7(10):e48279.
- Furian AF, Fighera MR, Oliveira MS, et al. Methylene Blue Prevents Methylmalonate-Induced Seizures and Oxidative Damage in Rat Striatum. Neurochemistry International. 2007;50(1):164–171.
- Gillman PK. Methylene Blue Implicated in Potentially Fatal Serotonin Toxicity. Anaesthesia. 2006;61(10):1013–1014.
Live PubMed Searches
Live PubMed queries that update as new papers are indexed.
- PubMed: methylene blue mitochondrial function
- PubMed: methylene blue cytochrome c oxidase
- PubMed: methylene blue Alzheimer's tau
- PubMed: methylene blue methemoglobinemia
- PubMed: methylene blue cerebral blood flow
- PubMed: methylene blue memory cognition
- PubMed: methylene blue antimicrobial
- PubMed: methylene blue ifosfamide encephalopathy
- PubMed: methylene blue serotonin syndrome
- PubMed: methylene blue photodynamic therapy
- PubMed: methylene blue G6PD deficiency
- PubMed: methylene blue vasoplegic shock
Connections
- Pharmaceutical Grade vs Industrial Dye
- Methylene Blue Dosing Guide
- Drug Interactions and Serotonin Syndrome
- History: Ehrlich and Phenothiazines
- Methylene Blue and Long COVID
- Methemoglobinemia and G6PD Deficiency
- Cognitive Enhancement and ADHD
- Mitochondrial Mechanism and Bioenergetics
- Photodynamic Therapy and Cancer Research
- Depression
- Dementia
- Alzheimer's Disease
- ADHD
- NAD+ and NMN
- Longevity Protocols
- Creatine
- Kidney Disease
- Malaria