Methylene Blue for Mitochondrial Bypass & Bioenergetics
Methylene blue is unique among small molecules in clinical use because it can act as an artificial electron acceptor inside the mitochondrial inner membrane — accepting electrons from NADH and Complex I and donating them directly to cytochrome c, effectively routing around partially damaged Complex III. The clinically relevant window is narrow: 0.5–4 mg/kg/day produces electron-shuttle benefit, while doses above roughly 5 mg/kg flip methylene blue into pro-oxidant behavior. The hormetic U-shape is unforgiving, the contrast with CoQ10 (which feeds the ETC rather than bypassing it) matters in clinical decision-making, and the drug-interaction profile — serotonin syndrome, G6PD hemolysis — is more dangerous than for any conventional antioxidant.
Table of Contents
- Why "Bypass" Is the Right Word
- The Electron Transport Chain in 90 Seconds
- How Methylene Blue Inserts Into the Chain
- The NADH Shuttle Problem MB Helps Solve
- The U-Shaped Hormetic Dose Curve
- Methylene Blue vs CoQ10: Different Tools
- Mitochondrial-Dysfunction States Where MB Has Been Studied
- Practical Dosing for the Bypass Effect
- Cautions Specific to Bioenergetic Use
- Key Research Papers
- Connections
- Featured Videos
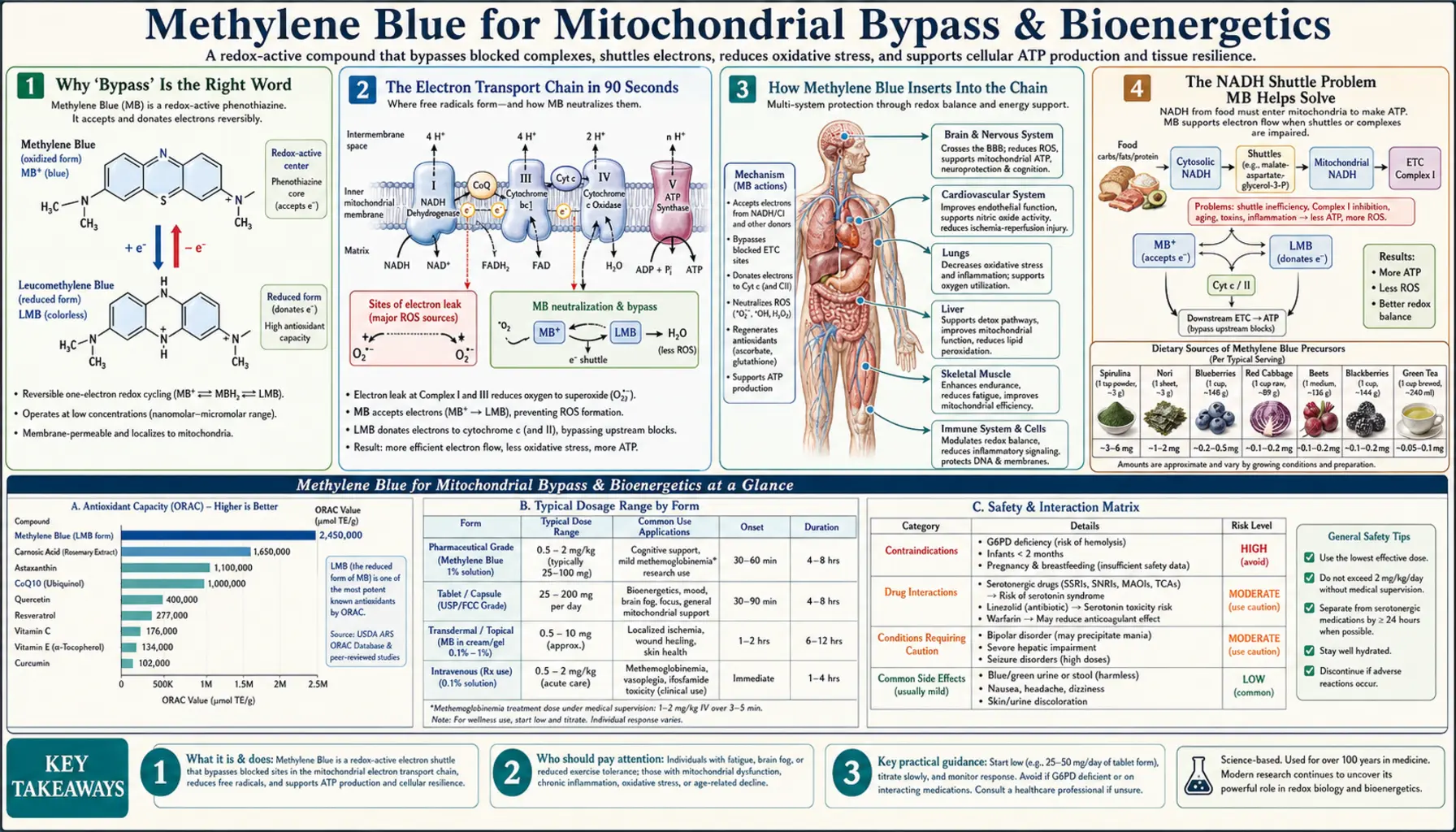
Why "Bypass" Is the Right Word
Most antioxidants do one of two things to the mitochondrial chain: they scavenge reactive oxygen species that have already leaked out (vitamin E, vitamin C, glutathione), or they donate electrons into the existing chain at a specific point (CoQ10 sits between Complex I/II and Complex III as a built-in electron carrier). Methylene blue does neither. It performs an entirely different trick — it acts as a parallel electron pathway, picking up electrons before they reach a damaged complex and depositing them downstream past the bottleneck.
This is most often phrased as "bypassing Complex I and III." The phrasing is correct but slightly misleading — methylene blue does not literally route around the entire complex. It accepts electrons from NADH (the same substrate Complex I uses) in its oxidized form, becoming leuco-methylene blue, and then deposits those electrons directly onto cytochrome c (the same electron carrier Complex III hands off to). Functionally the chain still runs — ATP synthase still pumps protons, oxygen is still the terminal acceptor — but the electrons can take a parallel express lane when the local stretch of road is broken.
In a healthy mitochondrion this parallel pathway is unnecessary. In a damaged or aged mitochondrion — with oxidized Complex I, mtDNA mutations affecting Complex III, post-viral damage, or traumatic-brain-injury bioenergetic crisis — the parallel pathway becomes the difference between ATP and apoptosis.
The Electron Transport Chain in 90 Seconds
To understand what methylene blue does, you need a brief refresher on what it is doing it to. The mitochondrial inner membrane hosts four protein complexes that form an electron-conducting wire:
- Complex I (NADH dehydrogenase) — accepts electrons from NADH (the universal currency of carbohydrate, fat, and protein oxidation), shuttles them onto coenzyme Q (ubiquinone), and pumps four protons across the inner membrane in the process.
- Complex II (succinate dehydrogenase) — accepts electrons from FADH&sub2; (made during the citric-acid cycle from succinate), also passes them to coenzyme Q. Does not pump protons.
- Coenzyme Q (CoQ10) — the small lipid electron carrier that shuttles between Complex I/II and Complex III.
- Complex III (cytochrome bc&sub1;) — accepts electrons from reduced CoQ10 and hands them to cytochrome c, pumping more protons.
- Cytochrome c — another small electron carrier; sits in the intermembrane space between Complex III and Complex IV.
- Complex IV (cytochrome c oxidase) — accepts electrons from cytochrome c and uses them to reduce molecular oxygen (O&sub2;) to water, again pumping protons.
- ATP synthase (sometimes called Complex V) — uses the proton gradient built by Complexes I, III, and IV to spin a rotor that synthesizes ATP from ADP + Pi.
The crucial point: damage to Complex I or Complex III is common in aging, in mtDNA mutations, in ischemia-reperfusion injury, in chronic post-viral states, and in neurodegeneration. Complex IV and ATP synthase are usually intact in those conditions. Methylene blue's parallel electron pathway is exactly between the damaged upstream stretch (Complex I → CoQ10 → Complex III) and the intact downstream stretch (cytochrome c → Complex IV → ATP synthase).
How Methylene Blue Inserts Into the Chain
Methylene blue exists in two reversible forms separated by two electrons and a proton: the oxidized form (the deep blue color) and the leuco form (colorless, reduced). In cells, methylene blue is rapidly reduced inside mitochondria by NADH dehydrogenase or directly by NADH at sites accessible from the matrix. Once reduced to leuco-methylene blue, the molecule diffuses across the inner membrane (it is small and lipophilic enough) and can then be re-oxidized by donating its two electrons to cytochrome c. Cytochrome c hands them to Complex IV, oxygen is reduced to water, and protons continue to flow through ATP synthase.
The cycle:
- NADH + MB(oxidized) → NAD+ + leuco-MB (in the matrix, near or via Complex I)
- Leuco-MB diffuses across the inner mitochondrial membrane to the intermembrane-space side
- Leuco-MB + 2 cytochrome c (Fe³+) → MB(oxidized) + 2 cytochrome c (Fe²+)
- Cytochrome c (Fe²+) feeds Complex IV; oxygen is reduced to water; ATP synthase spins.
- MB(oxidized) returns to the matrix side and accepts the next pair of electrons from NADH.
The shuttle runs as long as methylene blue is present in the catalytic concentration range and the downstream chain (cytochrome c → Complex IV → O&sub2;) is intact. The proton gradient built by Complex IV alone is enough to sustain meaningful ATP synthesis even when Complex I and III are partially crippled.
The NADH Shuttle Problem MB Helps Solve
NADH cannot cross the mitochondrial inner membrane directly. Cells therefore use shuttles — the malate-aspartate shuttle (in most tissues) and the glycerol-3-phosphate shuttle (in muscle and brain) — to move cytosolic reducing equivalents into the matrix where Complex I can use them. When mitochondria are damaged or NADH/NAD+ ratios are skewed (a hallmark of metabolic disease, post-viral fatigue, and aging), the shuttle backs up. Cytosolic NADH accumulates, fermentation increases, lactate rises.
Methylene blue partly relieves this bottleneck. Because it cycles between oxidized and reduced forms on both sides of the inner membrane, it acts as an additional cross-membrane electron transporter — not a true shuttle in the formal biochemistry sense, but functionally equivalent. The result in animal models and isolated mitochondria: lower NADH/NAD+ ratio in the cytosol, less lactate, more ATP per molecule of glucose or fatty acid burned.
This is part of why methylene blue is investigated as a potential intervention for long COVID and chronic fatigue, where mitochondrial dysfunction is a recurring finding. The evidence for clinical benefit remains preliminary.
The U-Shaped Hormetic Dose Curve
The single most important fact about methylene blue in bioenergetic use is that the dose-response is biphasic. At low doses (roughly 0.5–4 mg/kg in humans, equivalent to 35–280 mg for a 70 kg adult), methylene blue acts as an electron acceptor, supports ATP production, and reduces reactive oxygen species (because well-coupled mitochondria leak less superoxide). At high doses (above roughly 5–7 mg/kg), methylene blue starts to behave as a pro-oxidant: it auto-oxidizes, generates superoxide directly, can oxidize hemoglobin to methemoglobin, and overall worsens the very mitochondrial state it was meant to support.
The curve is sketched in animal cognition studies, in vitro mitochondrial respiration studies, and indirectly in the methemoglobinemia dose-response (which is paradoxical: methylene blue is the antidote at therapeutic doses, the cause at supra-therapeutic doses — see Methemoglobinemia).
The practical implication: when the user asks "if some is good, isn't more better?" the answer with methylene blue is an emphatic no. Doubling the dose can flip the entire pharmacology from beneficial to harmful. This is unusual; most water-soluble vitamins and most antioxidants tolerate large overshoots without flipping sign. Methylene blue does not.
Methylene Blue vs CoQ10: Different Tools
Both methylene blue and CoQ10 (ubiquinone) support mitochondrial bioenergetics, and both are sometimes promoted under the umbrella term "mitochondrial antioxidant." They are not interchangeable.
| Aspect | Methylene Blue | CoQ10 (Ubiquinone / Ubiquinol) |
|---|---|---|
| Role in ETC | Parallel bypass — routes around damaged complexes | Native carrier — feeds electrons through the existing complexes |
| Best when | Complex I or III is damaged (aging, mtDNA mutations, post-viral) | CoQ10 levels are depleted (statin therapy, aging, mitochondrial disease) |
| Dose range | 0.5–4 mg/kg/day (narrow window, biphasic) | 100–400 mg/day (wide window, no biphasic flip) |
| Side-effect profile | Serotonin syndrome, G6PD hemolysis, blue urine, MAO-A inhibition | Mild GI upset; few interactions |
| Drug interactions | Many serious (SSRIs, SNRIs, tramadol, dextromethorphan, lithium, triptans) | Mild warfarin interaction (CoQ10 reduces INR) |
| Photodynamic activity | Strong — absorbs 660 nm light, generates singlet oxygen | None |
| Cost | $30–80/month (USP-grade) | $15–60/month |
The clean way to think about it: CoQ10 helps when the chain is intact but undersupplied; methylene blue helps when the chain itself is damaged. Many integrative protocols use both, with CoQ10 as a daily background and methylene blue cycled in for specific bioenergetic-crisis indications.
Mitochondrial-Dysfunction States Where MB Has Been Studied
- Cerebral ischemia & stroke — rodent models consistently show smaller infarct volumes when methylene blue is given during the reperfusion phase. Human trials are scarce.
- Traumatic brain injury (TBI) — animal data are promising; bioenergetic crisis in the first 24 hours post-injury is partly addressable by parallel electron transport.
- Ifosfamide-induced encephalopathy — one of the FDA-recognized clinical uses; methylene blue restores neurologic function within hours in many cases. The mechanism is the same bypass effect — ifosfamide's chloroacetaldehyde metabolite inhibits Complex I.
- Mitochondrial myopathies — case reports and small series in primary mitochondrial disease (MELAS, Leigh syndrome). Evidence remains anecdotal.
- Post-viral fatigue and long COVID — the post-viral mitochondrial dysfunction signature (low NAD+/NADH, reduced Complex I activity) maps onto MB's mechanism. Clinical trials in progress; published data are preliminary.
- Aging-associated mitochondrial decline — the Atamna 2008 FASEB paper showed delayed cellular senescence in fibroblasts; longevity-medicine clinicians extrapolate from this, although human longevity data do not exist.
- Chronic fatigue syndrome / ME-CFS — case reports of benefit; no randomized trials.
- Glioma and brain tumor bioenergetics — experimental, photodynamic-adjacent (see Photodynamic Therapy).
Practical Dosing for the Bypass Effect
- Conservative starting dose: 0.5 mg/kg/day, taken orally diluted in water (about 35 mg for a 70 kg adult). Many clinicians begin at 10 mg fixed dose to establish tolerance and rule out the rare allergic reaction.
- Bioenergetic-support range: 1–2 mg/kg/day (about 70–140 mg for a 70 kg adult), divided into morning and early-afternoon doses to mimic natural ATP demand.
- Upper end (still therapeutic): 3–4 mg/kg/day (about 210–280 mg for a 70 kg adult). The Rodriguez 2016 fMRI study used a single 280 mg dose. Cognitive and bioenergetic effects plateau in this range; doses higher than 4 mg/kg/day should not be used outside clinical-trial protocols.
- Pharmaceutical grade only: USP-grade methylene blue from a compounding pharmacy or an FDA-registered manufacturer. Industrial-grade or aquarium-grade methylene blue contains heavy-metal contaminants (arsenic, mercury, lead) that disqualify it from oral use. See the parent article's Pharmaceutical Grade vs Industrial Dye page.
- Timing: Mornings and early afternoons. Methylene blue is mildly stimulating in some individuals due to MAO-A inhibition and increased brain bioenergetics; evening dosing can disrupt sleep.
- Vitamin C interaction: Ascorbate (vitamin C) reduces methylene blue to its leuco form in solution. Some clinicians co-administer vitamin C; others avoid it. The clinical data do not clearly favor either approach.
- Cycling: Many longevity-medicine protocols cycle methylene blue (5 days on, 2 days off, or 4 weeks on, 1 week off) rather than daily indefinite use. The data for cycling are mechanistic rather than trial-based.
Cautions Specific to Bioenergetic Use
- Serotonin syndrome — the single most important risk. Methylene blue is a potent reversible MAO-A inhibitor at all clinically relevant doses. Do NOT combine with SSRIs (sertraline, fluoxetine, escitalopram, citalopram, paroxetine), SNRIs (duloxetine, venlafaxine), tricyclics (amitriptyline, nortriptyline), MAOIs (selegiline, phenelzine), tramadol, fentanyl, dextromethorphan, lithium, triptans (sumatriptan etc.), MDMA, or St. John's Wort. The FDA issued an explicit warning in 2011. If discontinuing an SSRI to start methylene blue, allow at least 5 half-lives (~5 weeks for fluoxetine, ~1 week for sertraline/escitalopram) — under physician supervision.
- G6PD deficiency — methylene blue can precipitate severe hemolytic anemia in individuals with G6PD deficiency. The same redox cycling that gives MB its bioenergetic benefit also strips G6PD-deficient red blood cells of reducing equivalents they cannot regenerate. Test G6PD status before chronic use, particularly in patients of Mediterranean, African, or Southeast Asian descent. See Methemoglobinemia & G6PD Deficiency.
- Pregnancy — contraindicated. Intra-amniotic methylene blue was historically used in twin-pregnancy diagnostic studies and was associated with intestinal atresia in the fetus.
- Pro-oxidant range — doses above 5 mg/kg flip methylene blue from electron-accepting to electron-donating in the wrong direction, generating superoxide and potentially worsening the very dysfunction being treated. Stay in the 0.5–4 mg/kg/day window.
- Blue discoloration — expected and benign. Urine turns fluorescent blue-green; tongue and stool may also be tinted. Will stain teeth and porcelain. Rinse the mouth after sublingual dosing.
- Drug interactions beyond serotonin syndrome — methylene blue inhibits CYP1A2 and CYP2D6 to some extent. Monitor when combining with substrates of those enzymes (theophylline, caffeine, many psychiatric medications).
Key Research Papers
- Atamna H, Nguyen A, Schultz C, et al. Methylene blue delays cellular senescence and enhances key mitochondrial biochemical pathways. FASEB Journal. 2008;22(3):703–712.
- Rojas JC, Bruchey AK, Gonzalez-Lima F. Neurometabolic mechanisms for memory enhancement and neuroprotection of methylene blue. Progress in Neurobiology. 2012;96(1):32–45.
- Poteet E, Winters A, Yan LJ, et al. Neuroprotective actions of methylene blue and its derivatives. PLoS ONE. 2012;7(10):e48279.
- Tucker D, Lu Y, Zhang Q. From mitochondrial function to neuroprotection — an emerging role for methylene blue. Molecular Neurobiology. 2018;55(6):5137–5153.
- Callaway NL, Riha PD, Bruchey AK, et al. Methylene blue improves brain oxidative metabolism and memory retention in rats. Pharmacology Biochemistry and Behavior. 2004;77(1):175–181.
- Wen Y, Li W, Poteet EC, et al. Alternative mitochondrial electron transfer as a novel strategy for neuroprotection. Journal of Biological Chemistry. 2011;286(18):16504–16515.
- Bruchey AK, Gonzalez-Lima F. Behavioral, physiological and biochemical hormetic responses to the autoxidizable dye methylene blue. American Journal of Pharmacology and Toxicology. 2008;3(1):72–79.
- Rodriguez P, Zhou W, Barrett DW, et al. Multimodal randomized functional MR imaging of the effects of methylene blue in the human brain. Radiology. 2016;281(2):516–526.
- Riha PD, Bruchey AK, Echevarria DJ, Gonzalez-Lima F. Memory facilitation by methylene blue: dose-dependent effect on behavior and brain oxygen consumption. European Journal of Pharmacology. 2005;511(2–3):151–158.
- Stack C, Jainuddin S, Elipenahli C, et al. Methylene blue upregulates Nrf2/ARE genes and prevents tau-related neurotoxicity in transgenic mice. Human Molecular Genetics. 2014;23(14):3716–3732.
- Schirmer RH, Adler H, Pickhardt M, Mandelkow E. "Lest We Forget You — Methylene Blue…". Neurobiology of Aging. 2011;32(12):2325.e7–2325.e16.
- Wischik CM, Edwards PC, Lai RY, Roth M, Harrington CR. Selective inhibition of Alzheimer disease-like tau aggregation by phenothiazines. PNAS. 1996;93(20):11213–11218.
PubMed Topic Searches
- PubMed: methylene blue mitochondrial function
- PubMed: MB cytochrome c oxidase
- PubMed: MB electron transport chain bypass
- PubMed: MB hormesis dose response
- PubMed: MB traumatic brain injury
- PubMed: MB stroke cerebral ischemia
Connections
- Methylene Blue Overview
- MB Benefits Hub
- MB for Cognition & Brain
- MB Antiviral
- MB for Methemoglobinemia
- Mitochondrial Mechanism (parent deep-dive)
- Dosing Guide
- Drug Interactions & Serotonin Syndrome
- Methylene Blue & Long COVID
- Pharmaceutical Grade vs Industrial
- CoQ10
- NAD+ and NMN
- Glutathione
- Alpha Lipoic Acid for Mitochondria
- Longevity Protocols
- Stroke
- Traumatic Brain Injury
- All Antioxidants