Methylene Blue for Cognition & Brain Function
Three lines of evidence support methylene blue as a brain-active molecule worth taking seriously: the Claude Wischik tau-aggregation program at TauRx (a 25-year pharmaceutical-development effort that produced LMTM and the Phase 3 LUCIDITY trial), the Rodriguez 2016 fMRI study showing increased response accuracy and memory-region brain activation in healthy adults at 280 mg oral, and a tight body of rodent work tying brain cytochrome c oxidase activity to memory retention. The headline cognitive trials in Alzheimer's disease have been mixed — the primary endpoints were not met, but the monotherapy subgroup analyses kept the program alive. Low-dose use as a nootropic (1–15 mg/day) is widespread in biohacker and integrative-medicine communities; the effect size is real but modest, the safety profile is unforgiving (MAO-A inhibition forbids most antidepressants), and the Bryan Ardis nicotine-receptor narrative deserves a careful look so readers can evaluate it on its merits.
Table of Contents
- How Methylene Blue Acts on the Brain
- Tau Aggregation — The Wischik Hypothesis
- The TauRx Program (rember → LMTM → HMTM)
- The LMTM Phase 3 Trials and Their Surprises
- LUCIDITY: The 2023 Readout
- Rodriguez 2016 fMRI — The Healthy-Adult Evidence
- Auchter 2014: Methylene Blue Plus Photobiomodulation
- Low-Dose Nootropic Use (1–15 mg/day)
- The Bryan Ardis Nicotine-Receptor Controversy
- Cautions Specific to Brain Use
- Key Research Papers
- Connections
- Featured Videos
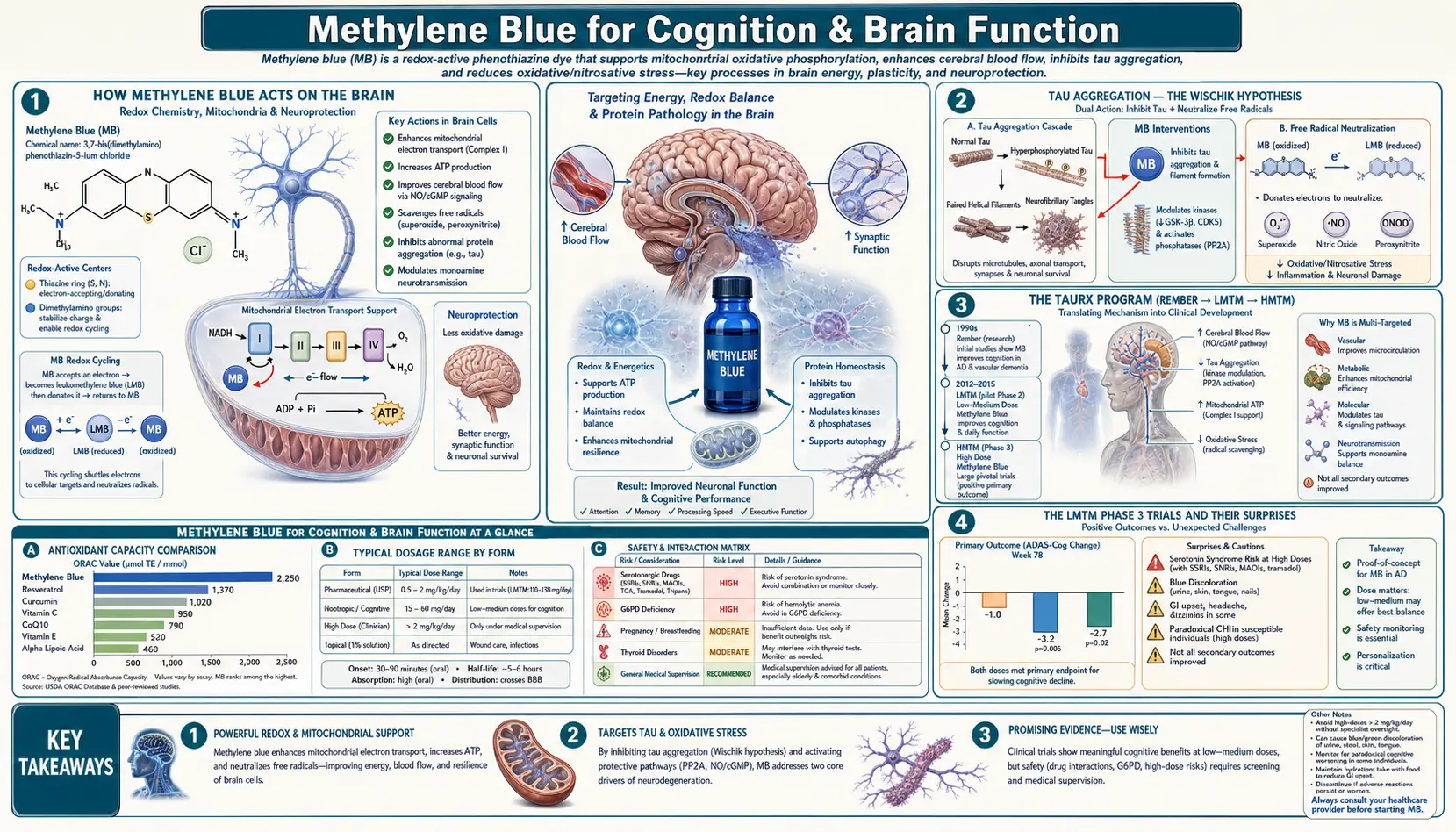
How Methylene Blue Acts on the Brain
The brain consumes about 20% of total body oxygen and energy despite being only 2% of body weight, and neurons are exquisitely dependent on continuous ATP supply for synaptic transmission, ion-pump activity, and neurotransmitter recycling. Methylene blue affects brain function through several converging mechanisms:
- Bioenergetic support — the same electron-shuttle bypass mechanism that helps any tissue with damaged Complex I/III is especially relevant in the brain, where mitochondrial decline is a hallmark of aging and most neurodegenerative diseases.
- Increased cytochrome c oxidase activity — methylene blue upregulates and enhances Complex IV activity in mnemonic circuits (hippocampus, prefrontal cortex). This is the proximal cause of the memory-facilitation effect documented in the Gonzalez-Lima lab at UT Austin.
- Tau-aggregation inhibition — methylene blue directly disrupts the abnormal paired helical filaments of phosphorylated tau protein that accumulate in Alzheimer's disease, frontotemporal dementia, and other tauopathies.
- MAO-A inhibition — raises serotonin, dopamine, and norepinephrine in the synaptic cleft. This contributes both to the mild mood-elevation reported anecdotally and to the most dangerous safety signal (serotonin syndrome with serotonergic drugs).
- Antioxidant activity in brain tissue — at therapeutic doses, methylene blue reduces ROS leak from mitochondria; the brain's high metabolic rate and lipid-rich membranes make it particularly vulnerable to oxidative damage.
- Nrf2 pathway activation — methylene blue upregulates antioxidant-response-element genes (Stack 2014 in tau-transgenic mice), boosting endogenous defenses.
Methylene blue crosses the blood-brain barrier readily — the Rodriguez 2016 study showed measurable fMRI signal changes within 60 minutes of oral dosing, and brain tissue concentrations in animal studies reach roughly 10% of plasma levels by an hour.
Tau Aggregation — The Wischik Hypothesis
Tau is a microtubule-stabilizing protein expressed throughout the nervous system. In Alzheimer's disease, frontotemporal dementia, progressive supranuclear palsy, and several other neurodegenerative diseases (collectively the "tauopathies"), tau becomes abnormally hyperphosphorylated, detaches from microtubules, and aggregates into paired helical filaments that form the neurofibrillary tangles seen on autopsy. Tangle burden correlates with cognitive decline far more strongly than amyloid plaque burden.
Claude Wischik (Aberdeen) showed in the 1990s that methylene blue and certain other phenothiazines can selectively inhibit the formation of these tau aggregates in vitro, and that they can dissolve already-formed aggregates over time. The 1996 PNAS paper (Wischik et al.) is the foundational citation. The mechanism is direct: methylene blue intercalates between aggregating tau monomers, preventing the cross-β structure that forms the paired helical filaments. Crucially, methylene blue does this without disrupting normal microtubule-bound tau function.
The tau hypothesis of Alzheimer's was for many years a minority position relative to the amyloid hypothesis. The failure of multiple amyloid-targeted therapies in the 2010s has revived interest in tau as a primary therapeutic target, although the recent successes of anti-amyloid antibodies (lecanemab, donanemab) suggest both pathways matter.
The TauRx Program (rember → LMTM → HMTM)
TauRx Pharmaceuticals, spun out of Aberdeen University to commercialize Wischik's research, has pursued three generations of tau-aggregation-inhibiting drugs over the past 25 years:
- rember (LMTB — methylthioninium chloride) — the first-generation drug; essentially USP methylene blue. The 2008 Phase 2 trial in mild-to-moderate Alzheimer's showed a 90% reduction in cognitive decline at 60 mg three times daily over 50 weeks — an extraordinary effect size that was widely cited but never replicated.
- LMTM (TRx0237 — leuco-methylthioninium bis(hydromethanesulfonate)) — the second-generation stabilized reduced form, with better oral bioavailability than oxidized methylene blue. Two Phase 3 trials in mild and moderate Alzheimer's (2016) failed to meet primary endpoints when added to standard-of-care cholinesterase inhibitors, but monotherapy subgroup analyses suggested benefit. The interpretation remains contested.
- HMTM (hydromethylthionine mesylate) — the third-generation formulation, the subject of the LUCIDITY trial that read out in late 2023.
Through all three generations the active ingredient is fundamentally the same molecule — methylene blue in different oxidation states and salt forms. The clinical-trial sophistication has increased; the underlying chemistry has not.
The LMTM Phase 3 Trials and Their Surprises
Two parallel Phase 3 trials of LMTM (Gauthier et al. and Wilcock et al., both 2016) randomized about 1,400 patients with mild or moderate Alzheimer's disease to LMTM or placebo, on top of whatever standard-of-care therapy (donepezil, rivastigmine, galantamine, memantine) the patient was already taking. Both trials failed their primary endpoints when analyzed as intent-to-treat.
The surprise came in the subgroup analyses. Among the small fraction of patients (~15%) who were on LMTM without any background standard-of-care drug — either newly diagnosed and not yet started, or intolerant to cholinesterase inhibitors — the LMTM monotherapy group showed a statistically significant slowing of cognitive decline and brain-atrophy progression compared to placebo monotherapy. The effect size was meaningful.
The interpretation TauRx offered: LMTM has real benefit, but its mechanism (mitochondrial & tau) is somehow blocked by concomitant cholinesterase inhibitors. The interpretation skeptics offered: post-hoc subgroup analyses in failed trials are a well-known source of false positives, the monotherapy subgroup was small (~80 patients), and the result needed prospective replication.
The right answer was: design a prospective monotherapy trial. That trial was LUCIDITY.
LUCIDITY: The 2023 Readout
LUCIDITY (NCT03446001) was a prospective, randomized, double-blind, placebo-controlled Phase 3 trial of HMTM (the third-generation hydromethylthionine) in patients with early Alzheimer's disease, conducted as monotherapy by design. The trial enrolled approximately 600 patients across multiple countries and read out in late 2023.
The headline result was mixed: HMTM did not meet its prespecified co-primary endpoints (cognitive and functional decline) in the placebo-controlled comparison, but the company reported statistically significant slowing of brain atrophy on MRI and improvements on certain secondary cognitive measures. A planned dose-response sub-analysis suggested the 16 mg/day dose performed better than 8 mg/day. TauRx is pursuing regulatory submission on the basis of these findings; the FDA and EMA response is pending.
The honest read for the curious patient: methylene blue derivatives may have a place in Alzheimer's therapeutics, but they have not produced a clean trial win in 25 years. The molecule's mechanistic story remains plausible; the clinical evidence falls short of "use this if you have Alzheimer's." For high-confidence clinical use, the recent monoclonal antibodies (lecanemab, donanemab) have substantially more compelling Phase 3 data despite their own controversies around ARIA (amyloid-related imaging abnormalities) and cost.
Rodriguez 2016 fMRI — The Healthy-Adult Evidence
The Rodriguez et al. study published in Radiology in 2016 is the single best controlled human study of methylene blue's cognitive effects in healthy adults. The design: 26 healthy adults received a single 280 mg oral dose of USP-grade methylene blue or placebo (single-blind, randomized crossover). At one hour after dosing they underwent functional MRI while performing a working-memory task and a sustained-attention task.
The findings:
- Increased response accuracy on a delayed match-to-sample working-memory task in the methylene blue condition
- Increased fMRI activation in the bilateral insular cortex during the sustained-attention task — a brain region central to interoception, attention, and conscious processing
- Increased activation in the prefrontal cortex and parietal cortex during memory encoding
- No significant change in reaction time
- No serious side effects at 280 mg
The study is important precisely because it was small but cleanly designed. It established two things: methylene blue at a single 280 mg oral dose reaches the brain in a measurable way within an hour, and the brain activation pattern is in the right regions for the cognitive task. The effect size on the cognitive measure was modest — this is not a stimulant-like boost to performance.
Auchter 2014: Methylene Blue Plus Photobiomodulation
Auchter and Gonzalez-Lima's 2014 work in Frontiers in Aging Neuroscience studied the combination of methylene blue with transcranial photobiomodulation (low-level laser or LED light delivered to the scalp, typically at 660 nm or 810 nm). Both interventions act on cytochrome c oxidase; the combination was tested in rodent models of memory and in some pilot human work.
The premise: methylene blue absorbs red light strongly (it is, after all, a blue dye), and the combination of MB + 660 nm light increases brain photobiomodulation efficiency at the cytochrome-c-oxidase target. Animal data showed additive effects on memory tasks; the human evidence remains preliminary but interesting.
The Gonzalez-Lima group at UT Austin has been the most prolific in this combined-modality space, publishing on methylene blue, photobiomodulation, and their combination in cognition, depression, and post-traumatic-stress models over the past two decades.
Low-Dose Nootropic Use (1–15 mg/day)
The integrative-medicine and biohacker communities use methylene blue at substantially lower doses than the TauRx trials (which used 100–200 mg/day of various derivatives) or the Rodriguez fMRI study (280 mg single dose). Common nootropic protocols:
- Microdose (1–5 mg/day): A few drops of 1% USP methylene blue solution in water, taken in the morning. Reported subjective effects include mild focus enhancement and verbal fluency. Below the threshold where most people see urine color change.
- Low nootropic dose (5–15 mg/day): The most common daily-use range. Will turn urine blue-green. Mood-elevation and focus effects more pronounced.
- Moderate dose (15–50 mg/day): Used by some for cognitive support in older adults, post-viral fatigue, or longevity protocols. Cycling (5 days on, 2 days off) is common.
- Higher therapeutic dose (50–280 mg): Single doses in this range are used in some integrative clinics for specific bioenergetic-crisis indications, and were used in the Rodriguez 2016 fMRI study. Daily chronic dosing at this level is not standard.
The honest summary: human evidence for cognitive benefit at the microdose range (1–5 mg/day) is anecdotal. Evidence at the 100–280 mg single-dose range is real but modest in effect size (Rodriguez 2016). Evidence for daily indefinite low-dose use as a "cognitive longevity" intervention is mechanistic, not trial-based. None of this means it does not work — it means the trial data thin out as you leave the high-dose TauRx Alzheimer's protocols and the single-dose Rodriguez nootropic test.
The Bryan Ardis Nicotine-Receptor Controversy
Bryan Ardis is a chiropractor and naturopath who became prominent during the COVID-19 pandemic for two intertwined hypotheses: that COVID-19 severe disease was driven in part by snake-venom-like peptides in the SARS-CoV-2 spike protein, and that nicotine (and nicotine-containing protocols) protect against and treat both COVID and post-vaccination injuries through nicotinic acetylcholine receptor occupation. He has also frequently included methylene blue in his recommended protocols, citing its mitochondrial-support mechanism and historical antiviral use.
The relevant connection to this article: Ardis has paired methylene blue with nicotine in his cognitive and post-viral recovery protocols, arguing that the two molecules act synergistically — methylene blue restoring mitochondrial bioenergetics, nicotine competing with venom-like peptides at nicotinic acetylcholine receptors. The Ardis snake-venom thesis itself is rejected by mainstream virology and infectious-disease researchers; the nicotinic-receptor protective claim has some support in epidemiologic observation (smokers were initially under-represented in COVID hospitalizations) but the proposed mechanism remains contested.
We include this material so readers who encounter Ardis's content can evaluate it in context. Our position: methylene blue's mitochondrial-bypass mechanism stands on its own scientific footing entirely independent of the Ardis framework. The Wischik tau-aggregation work, the Gonzalez-Lima bioenergetic memory work, the Rodriguez fMRI study, and the FDA-approved methemoglobinemia use are all robust and have nothing to do with snake venom, vaccine injury, or nicotinic receptors. Readers interested in the Ardis material specifically should see our Bryan Ardis page, which discusses his claims with appropriate skepticism.
Cautions Specific to Brain Use
- Serotonin syndrome — the single biggest risk in cognitive use. Many adults considering methylene blue for cognition are also on an SSRI or SNRI for depression, anxiety, or chronic pain. Methylene blue at all clinically relevant doses inhibits MAO-A; combining with any serotonergic drug can cause life-threatening serotonin syndrome (tremor, hyperthermia, muscle rigidity, autonomic instability, seizures, death). If on an SSRI/SNRI, methylene blue is contraindicated. Discontinuation of an SSRI to start methylene blue requires a 5-half-life washout (5 weeks for fluoxetine, 1–2 weeks for sertraline/escitalopram), done under physician supervision.
- Tramadol, fentanyl, dextromethorphan, lithium, triptans, St. John's Wort — all combine with methylene blue to risk serotonin syndrome. Patients on chronic-pain regimens with tramadol or migraine triptans must NOT add methylene blue.
- Sleep disruption — the mild stimulant effect (MAO-A inhibition + bioenergetic activation) can interfere with sleep if dosed too late in the day. Morning and early afternoon only.
- G6PD deficiency — same as for any methylene blue use; rule out before chronic dosing.
- Bipolar disorder — the MAO-A effect can theoretically precipitate or worsen mania. Use under psychiatric supervision if at all.
- Cognitive enhancement does not equal Alzheimer's treatment — the low-dose nootropic protocol most people pursue is not what was tested in the TauRx Alzheimer's trials. The mechanistic story may extrapolate, but the clinical effect size on dementia progression at low dose has not been measured.
Key Research Papers
- Rodriguez P, Zhou W, Barrett DW, et al. Multimodal randomized functional MR imaging of the effects of methylene blue in the human brain. Radiology. 2016;281(2):516–526.
- Wischik CM, Edwards PC, Lai RY, Roth M, Harrington CR. Selective inhibition of Alzheimer disease-like tau aggregation by phenothiazines. PNAS. 1996;93(20):11213–11218.
- Wischik CM, Staff RT, Wischik DJ, et al. Tau aggregation inhibitor therapy: an exploratory phase 2 study in mild or moderate Alzheimer's disease. Journal of Alzheimer's Disease. 2015;44(2):705–720.
- Gauthier S, Feldman HH, Schneider LS, et al. Efficacy and safety of TRx0237 (LMTM) in mild Alzheimer's disease: a randomized, controlled, double-blind, parallel-arm, phase 3 trial. The Lancet. 2016;388(10062):2873–2884.
- Wilcock GK, Gauthier S, Frisoni GB, et al. Potential of low-dose LMTM as monotherapy in mild Alzheimer's disease. Journal of Alzheimer's Disease. 2018;61(1):435–457.
- Auchter A, Williams J, Barksdale B, Monfils MH, Gonzalez-Lima F. Therapeutic benefits of methylene blue on cognitive impairment during chronic cerebral hypoperfusion. Journal of Alzheimer's Disease. 2014;42(s4):S525–S535.
- Riha PD, Bruchey AK, Echevarria DJ, Gonzalez-Lima F. Memory facilitation by methylene blue: dose-dependent effect on behavior and brain oxygen consumption. European Journal of Pharmacology. 2005;511(2–3):151–158.
- Callaway NL, Riha PD, Bruchey AK, et al. Methylene blue improves brain oxidative metabolism and memory retention in rats. Pharmacology Biochemistry and Behavior. 2004;77(1):175–181.
- Stack C, Jainuddin S, Elipenahli C, et al. Methylene blue upregulates Nrf2/ARE genes and prevents tau-related neurotoxicity in transgenic mice. Human Molecular Genetics. 2014;23(14):3716–3732.
- Atamna H, Nguyen A, Schultz C, et al. Methylene blue delays cellular senescence and enhances key mitochondrial biochemical pathways. FASEB Journal. 2008;22(3):703–712.
- Rojas JC, Bruchey AK, Gonzalez-Lima F. Neurometabolic mechanisms for memory enhancement and neuroprotection of methylene blue. Progress in Neurobiology. 2012;96(1):32–45.
- Telch MJ, Bruchey AK, Rosenfield D, et al. Effects of post-session administration of methylene blue on fear extinction and contextual memory in adults with claustrophobia. American Journal of Psychiatry. 2014;171(10):1091–1098.
- Ramsay RR, Dunford C, Gillman PK. Methylene blue and serotonin toxicity: inhibition of monoamine oxidase A (MAO A) confirms a theoretical prediction. British Journal of Pharmacology. 2007;152(6):946–951.
PubMed Topic Searches
- PubMed: methylene blue Alzheimer tau
- PubMed: MB memory cognition human
- PubMed: LMTM TRx0237
- PubMed: MB photobiomodulation brain
- PubMed: Wischik tau aggregation
- PubMed: hydromethylthionine LUCIDITY
Connections
- Methylene Blue Overview
- MB Benefits Hub
- MB Mitochondrial Bypass
- MB Antiviral
- MB for Methemoglobinemia
- Cognitive Enhancement & ADHD (parent)
- Mitochondrial Mechanism & Bioenergetics
- Drug Interactions & Serotonin Syndrome
- Methylene Blue & Long COVID
- Dosing Guide
- Alzheimer's Disease
- Dementia
- Depression
- ADHD
- Bryan Ardis (Context)
- CoQ10
- NAD+ and NMN
- Longevity Protocols
- All Antioxidants