Methylene Blue: Antiviral, Antimicrobial & Antiparasitic
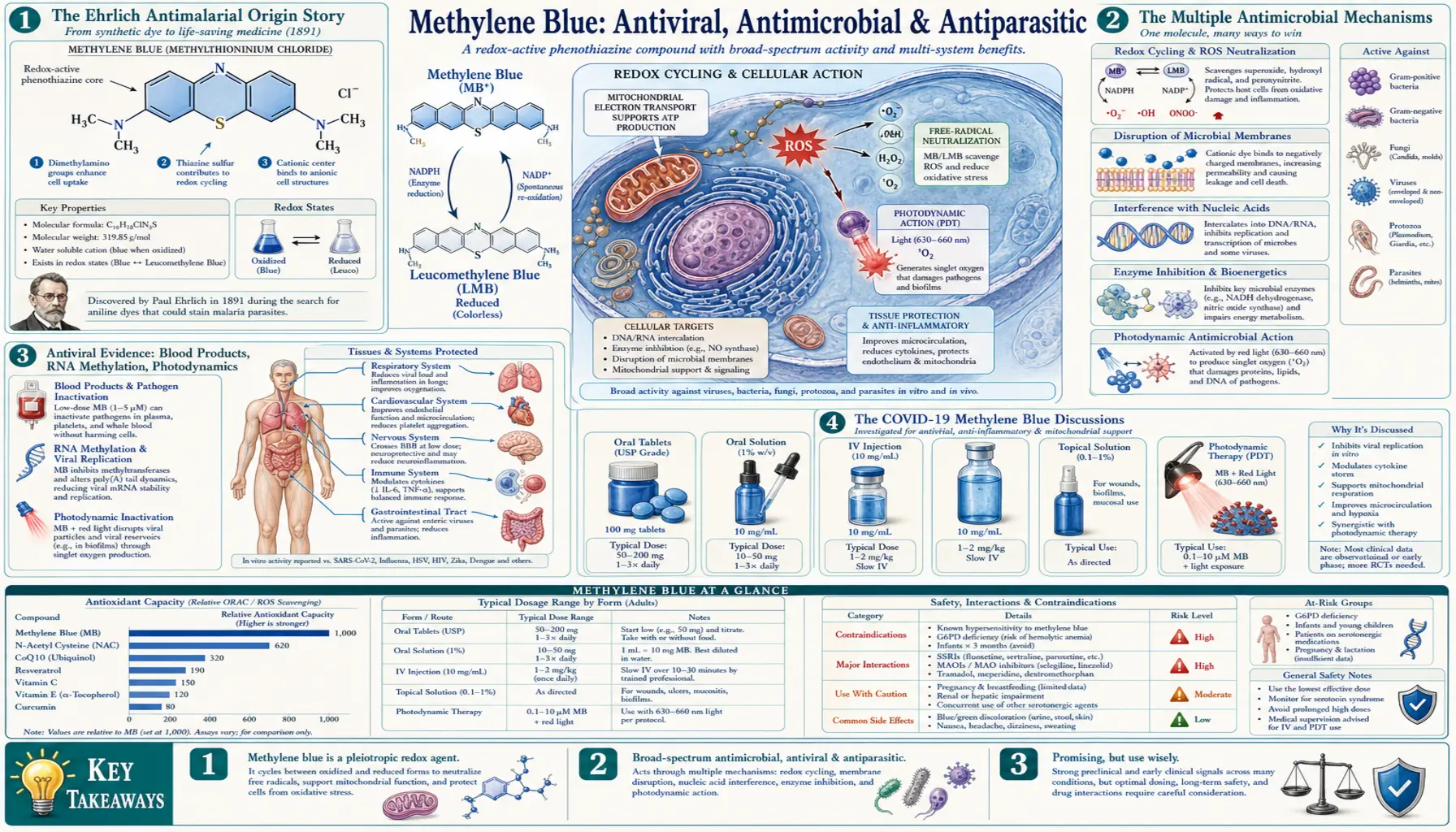
Methylene blue's antimicrobial career predates its bioenergetic and cognitive applications by almost a century. Paul Ehrlich used it as an antimalarial in 1891 — the first synthetic drug ever deployed against an infectious disease, half a century before chloroquine. The mechanism is multi-pronged: photodynamic generation of singlet oxygen on illumination (now an FDA-approved approach for periodontal disease and superficial skin infections), direct methylation and oxidative damage to viral RNA, oxidative damage to bacterial cell walls and biofilms, and selective killing of Plasmodium parasites. The COVID-19 hypothesis discussions of the early 2020s drew on legitimate in vitro data showing methylene blue inactivates SARS-CoV-2 under blood-bank photodynamic conditions, but the clinical case for oral systemic methylene blue against respiratory viruses remains unproven. The Bryan Ardis snake-venom thesis — in which methylene blue features prominently — deserves a clear-eyed look, marked as fringe and unproven.
Table of Contents
- The Ehrlich Antimalarial Origin Story
- The Multiple Antimicrobial Mechanisms
- Antiviral Evidence: Blood Products, RNA Methylation, Photodynamics
- The COVID-19 Methylene Blue Discussions
- Bacterial and Fungal Applications
- Periodontal & Oral Photodynamic Therapy
- Superficial Skin and Wound PDT
- Antiparasitic Use Today
- The Bryan Ardis Snake-Venom Thesis (Marked as Fringe)
- Cautions Specific to Antimicrobial Use
- Key Research Papers
- Connections
- Featured Videos
The Ehrlich Antimalarial Origin Story
Methylene blue was synthesized as a textile dye by Heinrich Caro at BASF in 1876. Paul Ehrlich — who would go on to win the 1908 Nobel Prize and to coin the phrase "magic bullet" — was at the time fascinated by the selective staining behavior of synthetic dyes in animal tissue. He noticed that methylene blue selectively stained Plasmodium parasites in blood smears, and reasoned that if it bound selectively, it might also kill selectively.
In 1891, Ehrlich and Paul Guttmann treated two malaria patients in a Berlin hospital with oral methylene blue. Both recovered. This is widely considered the first deliberate use of a synthetic chemical to treat an infectious disease in humans — the founding event of modern chemotherapy. Methylene blue continued as an antimalarial in tropical medicine for decades, but it had two practical drawbacks: it stained skin, sclera, and urine vivid blue, and it was eventually displaced by chloroquine (developed in the 1930s) which had a cleaner side-effect profile.
The modern coda: chloroquine resistance has driven renewed interest in methylene blue as an antimalarial. Trials in West Africa in the 2000s and 2010s showed that methylene blue combined with artemisinin-class drugs achieves high cure rates against drug-resistant Plasmodium falciparum, with the additional benefit of blocking gametocyte transmission (the stage that infects mosquitoes). Methylene blue is back in the WHO conversation as a tool against artemisinin-resistant malaria in Southeast Asia.
The Multiple Antimicrobial Mechanisms
Methylene blue does not have one antimicrobial mechanism — it has several, and which mechanism dominates depends on the target organism, the dose, and whether light exposure is involved.
- Photodynamic singlet-oxygen generation — methylene blue strongly absorbs red light around 660 nm. When illuminated, the excited methylene blue transfers energy to molecular oxygen, producing singlet oxygen (¹O&sub2;) — an extremely reactive species that damages lipid membranes, nucleic acids, and proteins indiscriminately. This is the basis of antimicrobial photodynamic therapy (aPDT), used for periodontal disease, oral infections, certain skin infections, and decontamination of blood products.
- RNA methylation — methylene blue can intercalate into RNA and DNA between adjacent base pairs, and at certain sites it transfers a methyl group to nucleic-acid bases. In RNA viruses, this disrupts replication. The mechanism is most relevant in the context of photoreactive RNA cross-linking.
- Direct oxidative damage — even without light, methylene blue cycling between oxidized and reduced forms can generate ROS in microbial environments, damaging cell walls (bacterial) and viral capsids.
- Mitochondrial selective targeting in parasites — Plasmodium mitochondria differ from mammalian mitochondria in important ways; methylene blue concentrates in the parasite's mitochondrion and disrupts heme polymerization in the food vacuole, generating toxic heme intermediates.
- Inhibition of bacterial enzymes — methylene blue inhibits certain bacterial respiratory enzymes more potently than mammalian counterparts, contributing to selective antibacterial activity.
Antiviral Evidence: Blood Products, RNA Methylation, Photodynamics
The strongest antiviral evidence for methylene blue is in the photodynamic inactivation of enveloped viruses in blood products. Methylene blue plus visible light is approved in several European countries (since the early 1990s) for the inactivation of HIV, hepatitis B, hepatitis C, and other enveloped viruses in plasma units used for transfusion. The mechanism is photodynamic: methylene blue diffuses into the lipid envelope and into the viral RNA, and visible-light exposure produces singlet oxygen that destroys envelope and genome. Treated plasma retains coagulation factor activity well enough to be transfusion-acceptable.
This blood-product application is the cleanest piece of antiviral evidence for methylene blue. It is mechanistically clear, well-validated by decades of European blood-bank use, and dose-response defined. It establishes that methylene blue can kill viruses under the right conditions.
The harder question is whether oral or systemic methylene blue produces clinically meaningful antiviral effect in vivo, in human patients, without the photodynamic conditions. The answer here is: maybe, with caveats. Small case series suggest benefit in certain viral conditions, but the photodynamic step that makes methylene blue clearly virucidal in test tubes does not happen efficiently inside the body except in tissues directly exposed to light (skin, accessible mucosa). Systemic antiviral activity, if real, is likely smaller than the bench-top photodynamic data suggest.
The COVID-19 Methylene Blue Discussions
During the COVID-19 pandemic, several research groups and clinicians proposed that methylene blue might be useful against SARS-CoV-2 for the following reasons:
- SARS-CoV-2 is an enveloped RNA virus — the kind that methylene blue photodynamically inactivates in blood products.
- Methylene blue inhibits SARS-CoV-2 spike-protein binding to ACE2 receptors in some in vitro assays.
- Methemoglobinemia was reported as a complication of severe COVID-19 in some patients; methylene blue is the antidote for methemoglobinemia.
- The mitochondrial dysfunction seen in long COVID is mechanistically addressable by methylene blue's bioenergetic-bypass effect — see Methylene Blue and Long COVID.
A few small studies and case series during 2020–2022 tested methylene blue combined with vitamin C and N-acetylcysteine (the "MCN" protocol) in ICU COVID patients, reporting improvements in oxygenation. The studies were not large randomized trials, and the results have not been independently replicated at scale. None of the major regulatory agencies has approved methylene blue for COVID-19 prevention or treatment.
Our position: the mechanistic case for methylene blue in post-viral mitochondrial dysfunction (long COVID) is more credible than the case for methylene blue as an acute antiviral. For the acute-infection setting, antiviral drugs with strong randomized-trial evidence (nirmatrelvir/ritonavir for high-risk patients) are first-line. For post-viral fatigue with documented mitochondrial dysfunction, methylene blue is one of several mechanistically reasonable adjuncts to explore under clinical supervision.
Bacterial and Fungal Applications
Methylene blue plus light is a robust photodynamic antimicrobial against a broad spectrum of bacteria and fungi. Documented activity:
- MRSA and other gram-positive bacteria — topical methylene blue + 660 nm light reliably kills MRSA in vitro and in superficial skin/wound clinical use
- Pseudomonas aeruginosa and other gram-negative bacteria — less susceptible than gram-positive but still photodynamically killable
- Bacterial biofilms — methylene blue penetrates biofilms reasonably well; photodynamic therapy can disrupt biofilms that resist antibiotics
- Candida albicans and other fungal species — photodynamic therapy effective in oral candidiasis (denture-stomatitis) and superficial cutaneous fungal infections
- Dermatophytes (tinea, ringworm) — topical photodynamic therapy is one option for treatment-resistant cases
Importantly, the antimicrobial activity is photodynamic in essentially all of these settings. Oral systemic methylene blue does not produce significant antibacterial activity in routine doses — the systemic concentrations needed for non-photodynamic antibacterial effect are well above the safe dosing window.
Periodontal & Oral Photodynamic Therapy
Antimicrobial photodynamic therapy with methylene blue is now a standard adjunct to scaling and root planing in periodontology. The protocol: a 0.005–0.01% methylene blue solution is applied to the periodontal pocket for several minutes (allowing diffusion into the biofilm), then a 660 nm red light is delivered into the pocket for 60–120 seconds per site. Singlet oxygen generation inside the biofilm kills the bacterial population without the systemic exposure of oral antibiotics.
Multiple randomized trials and meta-analyses support modest but consistent improvements in periodontal-pocket depth and clinical attachment level when aPDT is added to mechanical debridement. The systemic safety profile is excellent because exposure is local.
The same principle is applied in endodontics (root canal disinfection) and in the management of peri-implantitis (infection around dental implants). For patients exploring this option, look for periodontists or dentists with formal training in laser-assisted periodontal therapy or PDT.
Superficial Skin and Wound PDT
For dermatologic use, methylene blue + red light has been studied in:
- Chronic non-healing wounds — diabetic foot ulcers, pressure ulcers, venous stasis ulcers with multidrug-resistant bacterial colonization
- Acne vulgaris — some efficacy in inflammatory acne, particularly when combined with blue/red LED treatment
- Cutaneous infections by drug-resistant organisms — MRSA skin infections, certain mycobacterial infections
- Basal cell carcinoma — photodynamic therapy is one approved treatment modality, although methylene blue is less commonly used than 5-aminolevulinic acid (ALA) in this indication
The wound-care application is one of the most practically useful modern uses of methylene blue: topical 0.1–1% solution applied to the wound bed, then red-light exposure for 5–15 minutes per session. The treatment is operator-dependent and is not yet widely available outside specialty wound-care centers.
Antiparasitic Use Today
Beyond malaria, methylene blue has been studied for several parasitic infections:
- African trypanosomiasis (sleeping sickness) — methylene blue was one of the original Ehrlich-era anti-trypanosomal compounds
- Babesiosis — case reports in severe babesia infections in immunocompromised patients
- Giardia and other intestinal protozoa — limited efficacy data; not a first-line agent
- Antimalarial combination therapy — methylene blue + artemether or artesunate is the most actively investigated modern antiparasitic use, particularly in artemisinin-resistant P. falciparum
For practical patient use in 2026: methylene blue is not a first-line agent for any common parasitic infection in non-tropical countries. In settings of artemisinin-resistant malaria it has a legitimate place in combination protocols.
The Bryan Ardis Snake-Venom Thesis (Marked as Fringe)
Bryan Ardis is a chiropractor who in early 2022 published a documentary called "Watch the Water" that advanced the hypothesis that the COVID-19 pandemic was driven by snake-venom-like peptides — specifically peptides similar to those found in king cobra and other elapid venoms — rather than (or in addition to) the SARS-CoV-2 virus. Ardis argued these peptides reached the population through contaminated municipal water supplies and through the spike protein produced by mRNA vaccines, and that this explained both the respiratory failure and the neurological symptoms of severe COVID and post-vaccination injury.
The thesis has been comprehensively rejected by mainstream virology, infectious-disease, and toxinology research. The SARS-CoV-2 genome and spike-protein structure have been sequenced and characterized in extraordinary detail; there is no evidence of snake-venom-like peptide sequences in any meaningful sense. The municipal water-contamination claim is not supported by any documented contamination event. The vaccine-spike-equals-venom claim is incompatible with the well-characterized structure of the spike protein.
The reason we include this discussion: methylene blue features prominently in the Ardis protocols, often paired with nicotine, vitamin C, and other interventions. Patients encountering Ardis content online may form the impression that methylene blue's antiviral or detoxifying properties are part of an Ardis-style framework. This is not the case. Methylene blue's mitochondrial-bypass, photodynamic-antimicrobial, and methemoglobinemia-antidote properties are scientifically robust and entirely independent of the snake-venom hypothesis. Readers should evaluate the Ardis material on its own merits but not let it color their evaluation of legitimate methylene blue science.
Readers specifically interested in Ardis's claims should see our Bryan Ardis page and the Snake Venom Hypothesis page, both of which discuss the claims with appropriate skepticism and link to mainstream scientific responses.
Cautions Specific to Antimicrobial Use
- Photodynamic therapy is operator-dependent — dose of dye, duration of pre-light incubation, light wavelength, light fluence (J/cm²), and time of light delivery all matter. DIY home photodynamic therapy is not advisable; seek a trained operator.
- Photosensitivity for 24–48 hours post-systemic-dose — systemic methylene blue makes skin and eyes mildly photosensitive. Avoid direct intense sunlight for one or two days after high oral doses.
- Serotonin syndrome — same caveats as for any methylene blue use — do not combine with SSRIs, SNRIs, tricyclics, MAOIs, tramadol, fentanyl, dextromethorphan, lithium, triptans, MDMA, or St. John's Wort. The MAO-A inhibition is dose-independent in clinically relevant ranges.
- G6PD deficiency — screen before use, particularly in patients of Mediterranean, African, or Southeast Asian descent.
- Not a substitute for antibiotic therapy in serious infection — for established bacteremia, sepsis, pneumonia, or other serious bacterial infections, evidence-based antibiotic therapy is first-line. Photodynamic methylene blue is an adjunct for topical/localized infection, not a replacement for systemic antibiotics.
- Not a substitute for antiviral therapy in serious viral infection — for COVID-19 in high-risk patients, nirmatrelvir/ritonavir or other evidence-based antivirals are first-line. Methylene blue is at best an adjunct.
- Pregnancy — contraindicated.
Key Research Papers
- Wainwright M, Crossley KB. Methylene blue — a therapeutic dye for all seasons? Journal of Chemotherapy. 2002;14(5):431–443.
- Schirmer RH, Coulibaly B, Stich A, et al. Methylene blue as an antimalarial agent. Redox Report. 2003;8(5):272–275.
- Coulibaly B, Pritsch M, Bountogo M, et al. Efficacy and safety of triple combination therapy with artesunate-amodiaquine-methylene blue for falciparum malaria in children: a randomized controlled trial in Burkina Faso. Journal of Infectious Diseases. 2015;211(5):689–697.
- Lozano M, Cid J. The clinical implications of pathogen reduction in transfusion medicine. Transfusion Medicine and Hemotherapy. 2011;38(6):359–367.
- Wainwright M, Phoenix DA, Marland J, et al. A study of photobactericidal activity in the phenothiazinium series. FEMS Immunology and Medical Microbiology. 1997;19(1):75–80.
- Cieplik F, Deng D, Crielaard W, et al. Antimicrobial photodynamic therapy — what we know and what we don't. Critical Reviews in Microbiology. 2018;44(5):571–589.
- Wagner SJ, Skripchenko A, Robinette D, et al. Factors affecting virus photoinactivation by a series of phenothiazine dyes. Photochemistry and Photobiology. 1998;67(3):343–349.
- Gendrot M, Andreani J, Duflot I, et al. Methylene blue inhibits replication of SARS-CoV-2 in vitro. International Journal of Antimicrobial Agents. 2020;56(6):106202.
- Bojadzic D, Alcazar O, Buchwald P. Methylene blue inhibits the SARS-CoV-2 spike-ACE2 protein-protein interaction — a mechanism that can contribute to its antiviral activity against COVID-19. Frontiers in Pharmacology. 2021;11:600372.
- Floyd RA, Schneider JE Jr, Dittmer DP. Methylene blue photoinactivation of RNA viruses. Antiviral Research. 2004;61(3):141–151.
- Schirmer H, Müller IB, Becker K. The role of methylene blue in modern medicine. Drug Research. 2003;58(1):1–10.
- Akilov OE, Kosaka S, O'Riordan K, Hasan T. Photodynamic therapy for cutaneous leishmaniasis: the effectiveness of topical phenothiaziniums in parasite eradication and Th1 immune response stimulation. Photochemistry and Photobiology Sciences. 2007;6(10):1067–1075.
PubMed Topic Searches
- PubMed: methylene blue antimalarial
- PubMed: MB photodynamic antimicrobial
- PubMed: MB SARS-CoV-2
- PubMed: MB plasma virus inactivation
- PubMed: MB periodontal endodontic
- PubMed: MB MRSA biofilm wound
- PubMed: Ehrlich methylene blue history
Connections
- Methylene Blue Overview
- MB Benefits Hub
- MB Mitochondrial Bypass
- MB for Cognition & Brain
- MB for Methemoglobinemia
- Photodynamic Therapy (parent deep-dive)
- History: Ehrlich & Phenothiazines
- Methylene Blue & Long COVID
- Drug Interactions & Serotonin Syndrome
- Pharmaceutical Grade vs Industrial
- Malaria
- Bryan Ardis (Context)
- Bryan Ardis — Snake Venom Hypothesis
- All Antioxidants