Methylene Blue for Methemoglobinemia — the FDA-Approved Use
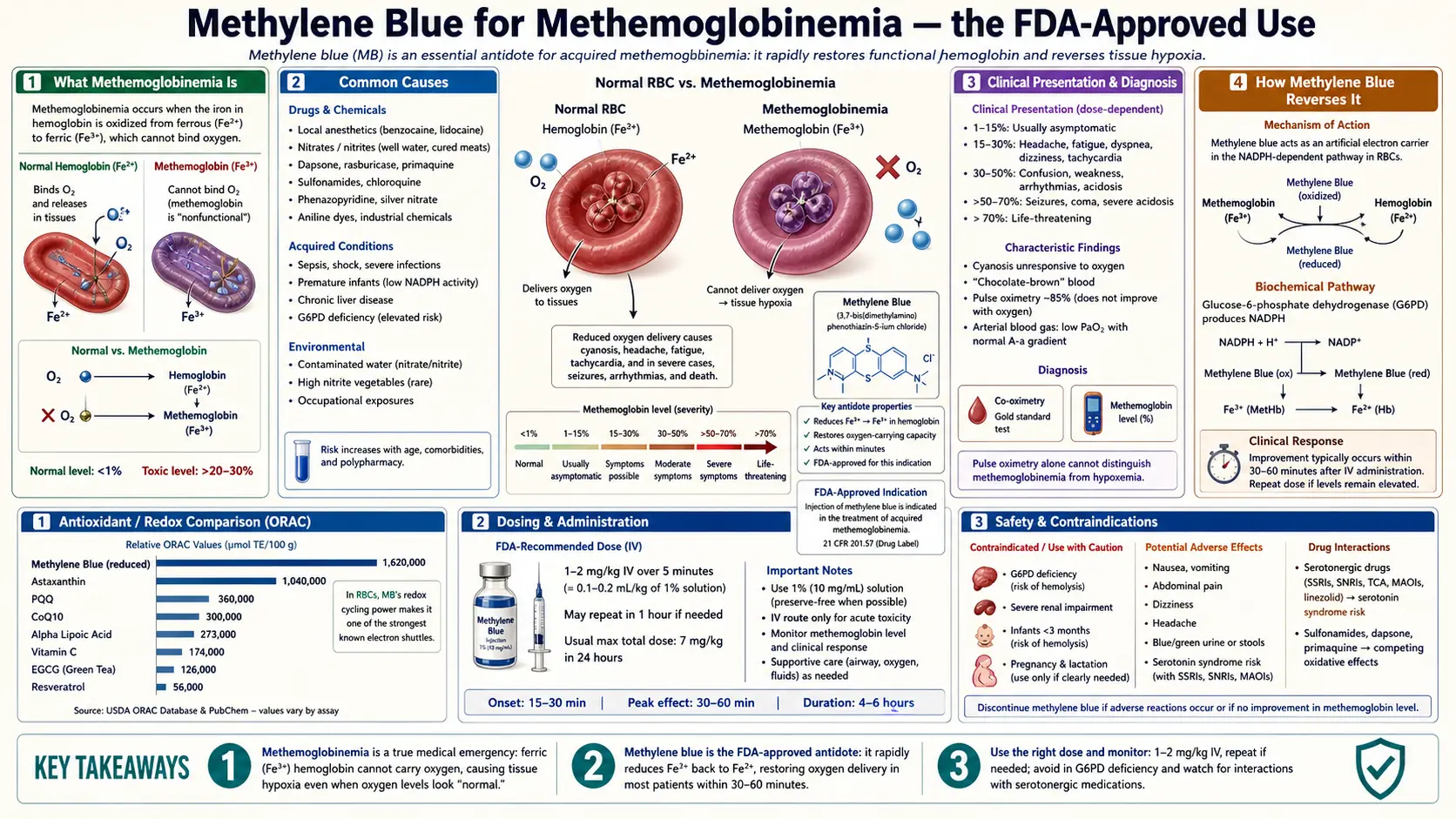
Methemoglobinemia is the FDA-approved indication for methylene blue and the reason it lives on every hospital crash cart. The mechanism is elegant: the iron at the center of hemoglobin must be in the ferrous (Fe²+) state to bind and release oxygen. When environmental oxidants (sodium nitrite, benzocaine, dapsone, aniline dyes, well-water nitrates) push iron into the ferric (Fe³+) state, the resulting methemoglobin can no longer carry oxygen and the patient turns chocolate-brown and cyanotic. Methylene blue, at 1–2 mg/kg IV over 5 minutes, is reduced inside red blood cells to leuco-methylene blue, which then donates electrons to methemoglobin, reducing it back to functional hemoglobin within minutes. Clinical response is dramatic and reliable — it is one of the most satisfying antidotes in toxicology. The two patient populations in whom methylene blue must NOT be used are G6PD-deficient patients (severe hemolysis) and patients on serotonergic medications (serotonin syndrome). This page covers the mechanism, the dosing, the contraindications, and the differential diagnoses to consider.
Table of Contents
- What Methemoglobinemia Is
- Common Causes
- Clinical Presentation & Diagnosis
- How Methylene Blue Reverses It
- Dosing — 1 to 2 mg/kg IV
- Congenital Methemoglobinemia (CYB5R3 Deficiency)
- Sodium Nitrite, Dapsone, and Aniline Poisoning
- Why G6PD Deficiency Is the Critical Contraindication
- Why SSRIs/MAOIs/Triptans Are Critical Contraindications
- The Methylene Blue Paradox — Antidote at Low Dose, Cause at High Dose
- Cautions & Alternative Antidotes
- Key Research Papers
- Connections
- Featured Videos
What Methemoglobinemia Is
Hemoglobin is the iron-containing protein in red blood cells that carries oxygen from the lungs to the tissues. The functional form of hemoglobin has its iron in the ferrous (Fe²+) oxidation state — only Fe²+ can reversibly bind oxygen and release it where needed. Under normal conditions, a small fraction (<1%) of hemoglobin is continuously oxidized to methemoglobin (Fe³+), and the body has two reducing systems — the cytochrome b5 reductase (CYB5R3) system in red blood cells and the NADPH-methemoglobin reductase backup — to convert it back to functional hemoglobin.
When the rate of oxidation exceeds the rate of reduction, methemoglobin accumulates. Methemoglobin cannot carry oxygen. Worse, methemoglobin alters the oxygen-binding curve of the remaining functional hemoglobin in a way that makes it cling to oxygen more tightly, releasing less to tissues. The combined effect produces functional hypoxia at a hemoglobin saturation level that the pulse oximeter does not accurately measure (pulse oximeters read methemoglobin as around 85% saturation regardless of true status — a critical clinical pitfall).
The patient's clinical picture matches the methemoglobin level:
- <15% methemoglobin — mostly asymptomatic; may have subtle gray-blue tinge
- 15–30% — cyanosis (chocolate-brown blood is pathognomonic), headache, fatigue, exercise intolerance
- 30–50% — dyspnea, tachypnea, tachycardia, dizziness, confusion
- 50–70% — severe acidosis, arrhythmias, seizures, coma
- >70% — usually fatal without intervention
Common Causes
Acquired methemoglobinemia is caused by exposure to oxidizing agents. The clinically important ones:
- Local anesthetics — benzocaine (especially throat sprays and topical teething products), prilocaine (a component of EMLA cream), articaine. Benzocaine sprays used during endoscopy or bronchoscopy are a documented hospital cause.
- Dapsone — used for pneumocystis prophylaxis (especially in HIV patients with sulfa allergy), leprosy, dermatitis herpetiformis. Chronic dapsone often produces low-grade chronic methemoglobinemia of 5–15%.
- Nitrites and nitrates — sodium nitrite (industrial chemical, also part of cyanide antidote kits, also a deliberate self-harm agent), amyl nitrite ("poppers"), well-water contamination with agricultural nitrates (the "blue baby syndrome" of infants drinking nitrate-rich rural well water).
- Aniline dyes and chemicals — rare industrial exposures, historically a major cause
- Antimalarials at toxic doses — primaquine, chloroquine
- Phenazopyridine (Pyridium) — the urinary-tract analgesic; methemoglobinemia is a recognized adverse event at therapeutic doses in some individuals
- Nitric oxide and nitrate-based medications — nitroglycerin, isosorbide, inhaled nitric oxide in critical care (usually mild)
- Congenital — CYB5R3 deficiency; rare
- Hereditary hemoglobin M variants — rare structural hemoglobin variants that are intrinsically prone to oxidation
The sodium-nitrite-suicide presentation has become an increasingly recognized emergency-department problem in the US and Europe over the past decade, partly driven by online forums and partly by easy mail-order availability of pure sodium nitrite. Methylene blue is the antidote.
Clinical Presentation & Diagnosis
The classic presentation:
- Cyanosis that does not improve with supplemental oxygen — the methemoglobin still cannot carry oxygen no matter how much O&sub2; is in the lungs
- Pulse oximeter reading stuck around 85% — methemoglobin absorbs light at both wavelengths the pulse oximeter uses, producing a falsely fixed reading regardless of true oxygen saturation. CO-oximetry (multiwavelength co-oximetry from an arterial blood gas) is the diagnostic test.
- Chocolate-brown blood — pathognomonic. Arterial blood drawn into a syringe from a methemoglobinemic patient does not turn bright red on exposure to air the way normal arterial blood does — it stays a dull dark brown.
- Saturation gap — the difference between the pulse oximeter SpO&sub2; (falsely ~85%) and the calculated arterial oxygen saturation from a blood gas (low normal or only mildly reduced) is the clue
- Confirmation — co-oximetry measures methemoglobin fraction directly, reports as a percentage
Differential diagnosis includes other causes of cyanosis with oxygen-resistant SpO&sub2; gap: sulfhemoglobinemia (similar presentation but no response to methylene blue), congenital cyanotic heart disease, and pulmonary AV shunting. The history (recent exposure to an oxidizing agent) and the chocolate-brown blood usually point to methemoglobinemia.
How Methylene Blue Reverses It
The mechanism is one of the cleanest in clinical pharmacology:
- Methylene blue is given IV (typically 1–2 mg/kg in 5–10 mL of saline over 5 minutes).
- Inside red blood cells, the NADPH-methemoglobin reductase enzyme uses NADPH to reduce methylene blue to its leuco (colorless, reduced) form.
- Leuco-methylene blue is a much stronger reducing agent than NADPH itself. It transfers two electrons to ferric methemoglobin (Fe³+), converting it back to ferrous hemoglobin (Fe²+).
- In the process, leuco-methylene blue is oxidized back to methylene blue, which can cycle through the reductase again.
- Net effect: methylene blue acts as a catalytic electron carrier between NADPH and methemoglobin, providing a pathway the body normally lacks at high methemoglobin loads.
The reaction runs quickly. Clinical response is usually visible within 15–30 minutes: cyanosis resolves, pulse oximeter readings return to normal, methemoglobin fraction on repeat co-oximetry falls toward baseline. By 60 minutes, most patients with moderate methemoglobinemia have largely normalized.
The dependence on the NADPH-reductase pathway is why G6PD-deficient patients cannot use methylene blue safely (see below). The G6PD enzyme is what produces NADPH; without it, leuco-methylene blue cannot be regenerated, and the methylene blue itself becomes a paradoxical oxidant.
Dosing — 1 to 2 mg/kg IV
| Setting | Dose | Notes |
|---|---|---|
| Acquired methemoglobinemia, moderate-severe | 1–2 mg/kg IV over 5 minutes | Standard adult dose: 1–2 mg/kg of 1% solution (10 mg/mL). May repeat once after 30–60 minutes if no response. |
| Maximum cumulative dose | ~7 mg/kg | Beyond this, methylene blue itself can cause methemoglobinemia and hemolysis. |
| Mild methemoglobinemia (asymptomatic, <20%) | Often no treatment needed; remove offending agent | Endogenous reductase clears methemoglobin over hours. |
| Ifosfamide-induced encephalopathy | 50 mg IV every 4–6 hours until resolved | Different mechanism (mitochondrial bypass), different dose schedule. |
| Congenital methemoglobinemia (CYB5R3 def) | 100–300 mg/day oral | Chronic maintenance therapy; often combined with riboflavin and ascorbate. |
| Pediatric dose | 1–2 mg/kg IV | Same per-weight dosing as adults; specific neonatal protocols exist. |
The IV is given slowly (over 5 minutes) because rapid administration can cause local irritation and brief blood-pressure swings. The solution stains everything — gloves, sheets, the patient's skin if extravasation occurs. Counseling the patient that urine will turn fluorescent blue-green for 24–48 hours is part of standard post-administration care.
Congenital Methemoglobinemia (CYB5R3 Deficiency)
Congenital methemoglobinemia is rare. The most common form is recessive cytochrome b5 reductase 3 (CYB5R3) deficiency, in which the red-cell enzyme that normally keeps methemoglobin below 1% is missing or non-functional. Patients live with chronic methemoglobin levels of 10–35%.
The clinical picture: lifelong cyanosis (blue-gray skin and lips) present from infancy, otherwise generally well, exercise tolerance moderately reduced. Type I CYB5R3 deficiency affects only red cells; Type II affects all tissues and is associated with progressive neurologic deterioration in early childhood.
The most famous case in popular medicine: the Fugates of Kentucky, the "blue people" of Troublesome Creek, who had a CYB5R3 mutation that became homozygous through generations of cousin marriage in an isolated Appalachian community. Effective treatment with oral methylene blue was demonstrated in this family by hematologist Madison Cawein in the 1960s — methylene blue 100 mg/day cleared their cyanosis within minutes.
Standard treatment of CYB5R3 deficiency today: methylene blue 100–300 mg/day oral, sometimes combined with riboflavin and ascorbate. Avoidance of oxidizing drugs (dapsone, sulfa drugs, certain anesthetics) is also essential.
Sodium Nitrite, Dapsone, and Aniline Poisoning
The three most clinically common acquired methemoglobinemia presentations:
- Sodium nitrite overdose — an increasingly recognized self-harm presentation. Pure sodium nitrite is available by mail-order, and online forums circulate dosing instructions. Patients present with profound cyanosis, often within 30 minutes of ingestion. Methemoglobin levels of 60–90% are common. Treatment: 1–2 mg/kg IV methylene blue, repeat as needed up to ~7 mg/kg cumulative, IV fluids, supportive care. Mortality is high if methylene blue is not given promptly; survival is the rule with prompt treatment.
- Dapsone-induced methemoglobinemia — chronic dapsone produces chronic low-grade methemoglobinemia (5–15%) that most patients tolerate. Acute toxic ingestion or accumulation in renal/hepatic dysfunction can drive levels to 30%+. Treatment: methylene blue 1–2 mg/kg IV, plus cimetidine (which inhibits the CYP450 metabolism of dapsone to its hydroxylamine metabolite, the actual oxidizing species). Dapsone toxicity often requires repeated methylene blue dosing because dapsone's long half-life keeps generating methemoglobin.
- Benzocaine spray methemoglobinemia — classic case is a patient who received benzocaine throat spray for endoscopy and develops cyanosis 30–60 minutes post-procedure. Often presents to recovery room nurses. Methemoglobin levels typically 20–40%. Single 1–2 mg/kg dose usually suffices.
Why G6PD Deficiency Is the Critical Contraindication
Glucose-6-phosphate dehydrogenase (G6PD) is the rate-limiting enzyme of the pentose-phosphate pathway, which generates NADPH. NADPH is required for the methylene blue reduction cycle described above — without NADPH, methylene blue cannot be reduced to its active leuco form.
In a G6PD-deficient red blood cell, giving methylene blue produces two simultaneous problems:
- The methylene blue cannot be effectively reduced, so it does not reverse the methemoglobinemia (it does not work as an antidote).
- The methylene blue itself acts as an oxidant in the absence of adequate reduction, generating reactive oxygen species inside red cells that have no glutathione defense (glutathione regeneration also requires NADPH from G6PD).
The result: severe hemolytic anemia. Red cells lyse, free hemoglobin appears in urine (dark cola-colored urine), bilirubin rises, hematocrit crashes. In severe G6PD-deficient patients exposed to methylene blue, the hemolysis can be life-threatening.
G6PD deficiency affects approximately 400 million people worldwide, with highest prevalence in populations historically exposed to malaria: Mediterranean (Italian, Greek, Sephardic Jewish), Sub-Saharan African, Middle Eastern, and Southeast Asian descent. The African-variant form (most common in African-American patients) is generally milder; the Mediterranean form is more severe.
Practical implication: In emergency settings with severe methemoglobinemia, methylene blue is given empirically because the alternative (no treatment) is often worse. But the clinician must know that if hemolysis develops, the diagnosis of G6PD deficiency is the explanation, and alternative antidotes (ascorbate, exchange transfusion, hyperbaric oxygen) must be deployed.
For chronic or elective use of methylene blue (cognitive, bioenergetic, or long-term CYB5R3 maintenance), G6PD testing before starting is essential.
Why SSRIs/MAOIs/Triptans Are Critical Contraindications
Methylene blue is a potent reversible inhibitor of monoamine oxidase A (MAO-A) at all clinically used doses, including the 1–2 mg/kg IV given for methemoglobinemia. MAO-A is one of the principal enzymes that breaks down serotonin in the brain and elsewhere. Inhibiting it raises synaptic serotonin levels.
When methylene blue is given to a patient already taking a serotonergic medication, the combined effect can produce serotonin syndrome — a potentially fatal toxidrome characterized by:
- Mental status changes — agitation, confusion, hallucinations
- Autonomic instability — tachycardia, hypertension, fever (often >40°C), diaphoresis, mydriasis
- Neuromuscular abnormalities — tremor, myoclonus, hyperreflexia, clonus (especially ankle clonus), rigidity
- In severe cases — seizures, rhabdomyolysis, DIC, multi-organ failure, death
The contraindicated medications (any of these in the patient's recent history triggers caution):
- SSRIs — fluoxetine, sertraline, paroxetine, citalopram, escitalopram, fluvoxamine, vilazodone, vortioxetine
- SNRIs — venlafaxine, desvenlafaxine, duloxetine, milnacipran, levomilnacipran
- Tricyclic antidepressants — amitriptyline, nortriptyline, clomipramine, imipramine, desipramine, doxepin
- MAOIs — selegiline, phenelzine, tranylcypromine, isocarboxazid, rasagiline
- Tramadol, fentanyl, meperidine, methadone
- Dextromethorphan (common in cough/cold preparations like Robitussin DM, NyQuil, Vicks)
- Triptans — sumatriptan, rizatriptan, eletriptan, zolmitriptan, etc. (for migraine)
- Lithium
- MDMA, mescaline, LSD, psilocybin
- St. John's Wort, 5-HTP, L-tryptophan supplements
- Linezolid (the antibiotic; rare but documented)
The FDA issued an explicit Drug Safety Communication in July 2011 warning of fatal serotonin syndrome when methylene blue was given to surgical patients on serotonergic medications. The warning is in the methylene blue package insert.
In the emergency methemoglobinemia setting, the medication history must be obtained quickly. If the patient is on a serotonergic drug, alternative antidotes (ascorbate, hyperbaric oxygen, exchange transfusion) should be considered, or methylene blue given only if methemoglobinemia is life-threatening with intensive monitoring for serotonin syndrome. If discontinuing an SSRI to permit elective methylene blue use, allow a 5-half-life washout (5 weeks for fluoxetine, 1–2 weeks for sertraline/escitalopram) under physician supervision.
The Methylene Blue Paradox — Antidote at Low Dose, Cause at High Dose
One of the more counterintuitive facts in clinical pharmacology: methylene blue is the antidote for methemoglobinemia at the standard dose (1–2 mg/kg) but causes methemoglobinemia and hemolysis at higher doses (above ~7 mg/kg cumulative). The mechanism is the same biphasic dose-response (see hormetic dose curve) that operates in all of methylene blue's pharmacology.
At low doses, methylene blue cycles through the NADPH-reductase pathway productively, accepting electrons and donating them to methemoglobin. At high doses, the NADPH supply cannot keep up with the methylene blue load. Methylene blue itself becomes a direct oxidant, oxidizing hemoglobin to methemoglobin and red-cell glutathione, producing hemolysis.
The clinical implication: the cumulative dose limit (~7 mg/kg over 24 hours) is firm. Reaching that limit without resolution of the methemoglobinemia means switching to alternative antidotes (ascorbate, exchange transfusion, hyperbaric oxygen). Repeating methylene blue beyond the limit accelerates rather than treats the methemoglobinemia.
Cautions & Alternative Antidotes
- G6PD deficiency — methylene blue is relatively contraindicated; severe hemolysis is the risk. Alternative: high-dose IV ascorbate (200–1000 mg/kg/day), exchange transfusion, hyperbaric oxygen.
- Serotonergic medications — serotonin syndrome risk. Same alternative antidotes apply.
- Pregnancy — intra-amniotic methylene blue was associated with intestinal atresia in twin-pregnancy studies. IV methylene blue in pregnant women is used only when the alternative (severe methemoglobinemia) is life-threatening.
- Renal failure — methylene blue is partially renally cleared; dose reduction may be needed in advanced CKD.
- Cumulative dose limit ~7 mg/kg — beyond this, methylene blue worsens methemoglobinemia and risks hemolysis.
- Always confirm the diagnosis with co-oximetry — sulfhemoglobinemia presents similarly but does not respond to methylene blue; congenital cardiac shunts present similarly but require different management.
- Remove the offending agent — continuing benzocaine spray or dapsone or sodium nitrite alongside methylene blue treatment defeats the purpose. Identify and stop the source.
- Alternative antidotes — ascorbate (vitamin C) at high dose has weak methemoglobin-reducing activity; exchange transfusion physically removes methemoglobin; hyperbaric oxygen forces enough dissolved oxygen into plasma to support tissue oxygenation while the body slowly clears methemoglobin. For severe G6PD-deficient methemoglobinemia, exchange transfusion is often the practical choice.
- Pulse oximetry is unreliable — do not trust the SpO&sub2; reading. CO-oximetry from a blood gas is the only accurate measurement.
Key Research Papers
- Wendel WB. The control of methemoglobinemia with methylene blue. Journal of Clinical Investigation. 1939;18(2):179–185.
- Bistas E, Sanghavi DK. Methylene blue. StatPearls Publishing. Updated 2023.
- Beutler E. G6PD deficiency. Blood. 1994;84(11):3613–3636.
- Ramsay RR, Dunford C, Gillman PK. Methylene blue and serotonin toxicity: inhibition of monoamine oxidase A (MAO A) confirms a theoretical prediction. British Journal of Pharmacology. 2007;152(6):946–951.
- Gillman PK. Methylene blue implicated in potentially fatal serotonin toxicity. Anaesthesia. 2006;61(10):1013–1014.
- Skold A, Cosco DL, Klein R. Methemoglobinemia: pathogenesis, diagnosis, and management. Southern Medical Journal. 2011;104(11):757–761.
- Wright RO, Lewander WJ, Woolf AD. Methemoglobinemia: etiology, pharmacology, and clinical management. Annals of Emergency Medicine. 1999;34(5):646–656.
- Cortazzo JA, Lichtman AD. Methemoglobinemia: a review and recommendations for management. Journal of Cardiothoracic and Vascular Anesthesia. 2014;28(4):1043–1047.
- Percy MJ, Lappin TR. Recessive congenital methaemoglobinaemia: cytochrome b(5) reductase deficiency. British Journal of Haematology. 2008;141(3):298–308.
- Ash-Bernal R, Wise R, Wright SM. Acquired methemoglobinemia: a retrospective series of 138 cases at 2 teaching hospitals. Medicine (Baltimore). 2004;83(5):265–273.
- Neuhaeuser C, Weigand N, Schaaf H, et al. Postoperative methemoglobinemia following local infiltration anesthesia with prilocaine in adolescents. European Journal of Anaesthesiology. 2012;29(6):300–303.
- Cawein M, Behlen CH 2nd, Lappat EJ, Cohn JE. Hereditary diaphorase deficiency and methemoglobinemia. Archives of Internal Medicine. 1964;113:578–585.
- Mansouri A, Lurie AA. Concise review: methemoglobinemia. American Journal of Hematology. 1993;42(1):7–12.
PubMed Topic Searches
- PubMed: methylene blue methemoglobinemia
- PubMed: sodium nitrite poisoning
- PubMed: dapsone methemoglobinemia
- PubMed: benzocaine prilocaine methemoglobinemia
- PubMed: G6PD methylene blue hemolysis
- PubMed: MB serotonin syndrome SSRI
- PubMed: congenital methemoglobinemia CYB5R
Connections
- Methylene Blue Overview
- MB Benefits Hub
- MB Mitochondrial Bypass
- MB for Cognition & Brain
- MB Antiviral
- Methemoglobinemia & G6PD (parent deep-dive)
- Drug Interactions & Serotonin Syndrome
- Dosing Guide
- Pharmaceutical vs Industrial
- Toxins
- Anemia
- Depression (SSRI Interactions)
- G6PD Test
- Vitamin C (Alternative Reducing Agent)
- All Antioxidants