Tryptophan and Niacin Synthesis
The serotonin and melatonin story typically gets the popular-nutrition attention, but the metabolic majority of dietary tryptophan — roughly 95% — does not go to serotonin at all. It goes down the kynurenine pathway, a long sequence of enzymatic reactions that ultimately yields niacin (vitamin B3) and the universal redox cofactor nicotinamide adenine dinucleotide (NAD+). The conversion is famously inefficient, requiring approximately 60 mg of tryptophan to produce 1 mg of niacin equivalents (NE), which is the modern dietary unit that captures this dual sourcing. The kynurenine pathway also produces several biologically active intermediates — the neuroprotective kynurenic acid branch and the neurotoxic quinolinic acid branch — that have become major topics in psychiatric and neurodegenerative disease research. The pellagra story is one of the most consequential nutrition history lessons of the twentieth century: corn-based diets in the American South triggered an epidemic of skin, gut, and mental disease because corn is uniquely low in BOTH bioavailable niacin AND in tryptophan that the body could convert to niacin. Hartnup disease is the genetic form of the same metabolic vulnerability. This page walks through the chemistry, the historical pellagra epidemic and its eventual conquest, the Hartnup disease story, and the modern significance of the kynurenine pathway.
Table of Contents
- The Kynurenine Pathway in Detail
- The 60:1 Conversion Ratio and Niacin Equivalents
- NAD+ Biosynthesis from Tryptophan
- The Pellagra Epidemic — Corn, the American South, and the 4 D's
- Joseph Goldberger and the End of Pellagra
- Why Corn Is the Pellagra Trigger
- Nixtamalization — Mesoamerican Wisdom
- Hartnup Disease — The Genetic Form
- The Kynurenic vs Quinolinic Branches
- Modern Clinical Significance
- Cautions and Cofactor Notes
- Key Research Papers
- Connections
- Featured Videos
The Kynurenine Pathway in Detail
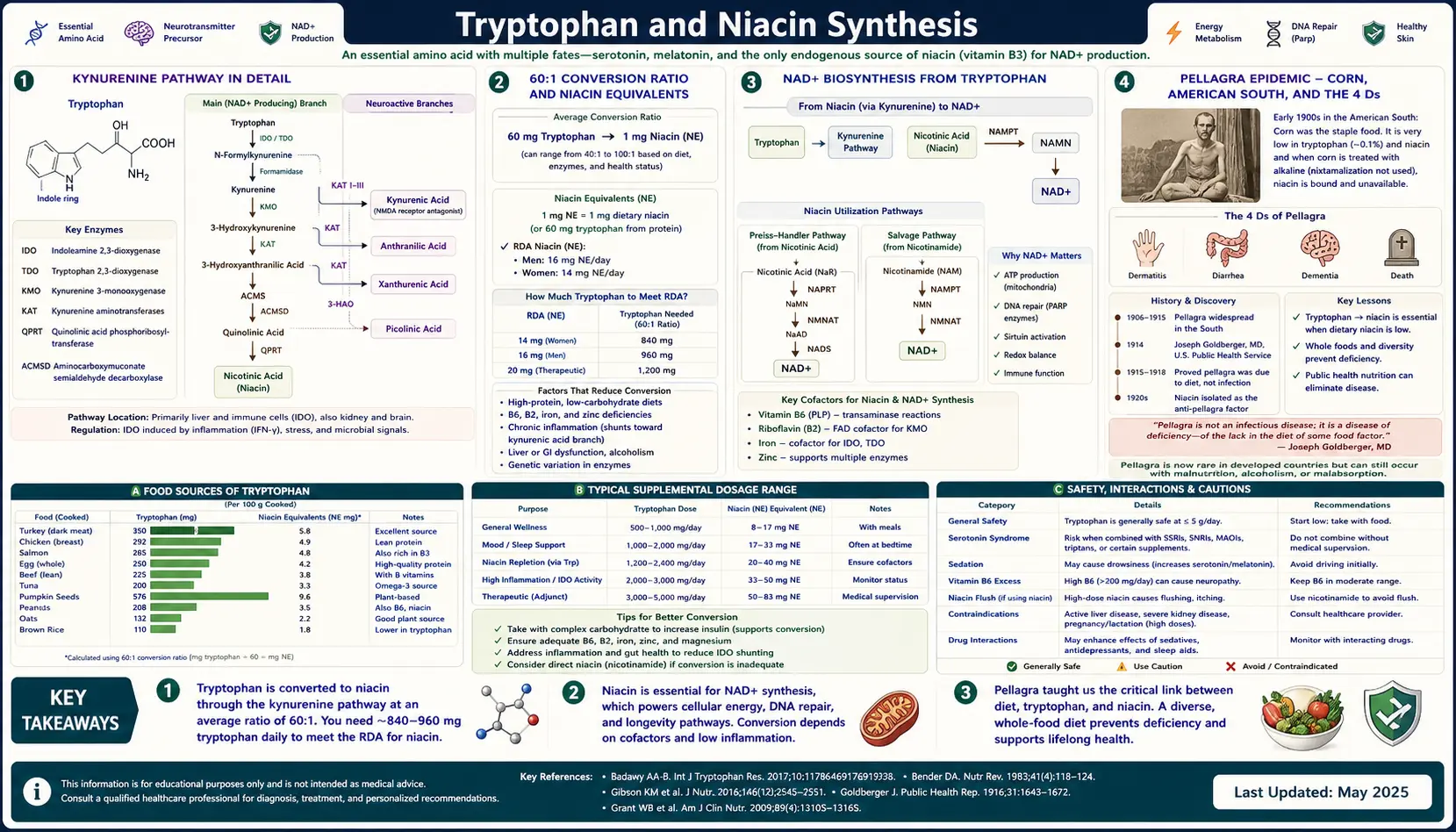
The kynurenine pathway is one of the longest enzymatic sequences in human biochemistry. It catabolizes the indole ring of tryptophan in roughly eight discrete enzymatic steps to ultimately yield quinolinic acid, which is then committed into NAD+ biosynthesis. The major steps are:
- L-tryptophan is oxidized at the C2-C3 bond of the indole ring by either indoleamine 2,3-dioxygenase (IDO) (in most peripheral tissues, the immune system, the brain) or tryptophan 2,3-dioxygenase (TDO) (predominantly in the liver). Both yield N-formylkynurenine. This is the rate-limiting step of the whole pathway.
- N-formylkynurenine is rapidly deformylated to L-kynurenine.
- L-kynurenine sits at a critical metabolic fork:
- One branch goes through kynurenine aminotransferase (KAT) to yield kynurenic acid. Kynurenic acid is a NMDA receptor antagonist and is broadly neuroprotective.
- The other branch — the quantitatively dominant one — goes through kynurenine 3-monooxygenase (KMO) to yield 3-hydroxykynurenine. From there:
- 3-hydroxykynurenine is processed by kynureninase (a vitamin B6-dependent enzyme) to yield 3-hydroxyanthranilic acid.
- 3-hydroxyanthranilic acid is processed by 3-hydroxyanthranilate 3,4-dioxygenase to yield 2-amino-3-carboxymuconic-6-semialdehyde (ACMS).
- ACMS spontaneously cyclizes to quinolinic acid (no enzyme required for this step).
- Quinolinic acid is processed by quinolinate phosphoribosyltransferase (QPRT) to yield nicotinic acid mononucleotide (NaMN), which enters the canonical NAD+ biosynthetic pathway and eventually becomes NAD+.
The IDO/TDO step is regulated by inflammation (IDO is strongly induced by interferon-gamma) and by cortisol (TDO is induced by glucocorticoids). This is the molecular hinge between inflammation, stress, and the rest of the tryptophan biology — in inflammation and chronic stress, more dietary tryptophan is shunted down the kynurenine pathway, less is available for serotonin synthesis, and more potentially neurotoxic intermediates accumulate.
The 60:1 Conversion Ratio and Niacin Equivalents
In typical human metabolism, approximately 60 mg of dietary tryptophan yields about 1 mg of niacin equivalents (NE). This ratio is the basis for the modern dietary unit. The Recommended Dietary Allowance (RDA) for niacin in adults is expressed as Niacin Equivalents and is 16 mg NE/day for men and 14 mg NE/day for women. The total of (preformed niacin in milligrams) plus (dietary tryptophan in milligrams divided by 60) must meet this RDA to prevent pellagra.
The 60:1 ratio is not fixed. It is influenced by:
- Cofactor status — the pathway depends on vitamin B6 (kynureninase), vitamin B2 (kynurenine 3-monooxygenase contains an FAD prosthetic group), and iron (multiple steps). Deficiency of any of these reduces the conversion efficiency.
- Pregnancy — pregnancy increases the efficiency to roughly 30:1, providing more NE per gram of dietary tryptophan. This appears to be a hormonal effect on hepatic TDO expression.
- Hormonal contraception — estrogen-containing oral contraceptives modestly increase the conversion efficiency, similar to pregnancy.
- Protein-deficient diets — in severe protein malnutrition, more of the limited tryptophan supply may be diverted to serotonin and melatonin pathways rather than to NE production. This is part of why severe protein-energy malnutrition (kwashiorkor) presents with mental status changes as well as the visible wasting.
- Liver disease — advanced cirrhosis reduces hepatic TDO activity and the conversion efficiency.
The practical implication for healthy adults with adequate mixed diets is that endogenous tryptophan-to-niacin conversion typically supplies roughly half of the daily niacin requirement, with preformed niacin (from meat, poultry, fish, whole grains, peanuts, fortified cereals) supplying the other half. Either source alone is sufficient if intake is generous; the failure mode — pellagra — requires that both be deficient, which is the historical and modern epidemiology of the disease.
NAD+ Biosynthesis from Tryptophan
Quinolinic acid is the ultimate kynurenine-pathway endpoint that gets committed into NAD+ biosynthesis. The committing enzyme is quinolinate phosphoribosyltransferase (QPRT), which transfers a phosphoribosyl group from PRPP onto quinolinate to yield nicotinic acid mononucleotide (NaMN). From NaMN, the canonical NAD+ pathway proceeds:
- NaMN is adenylylated by NMNAT (nicotinamide mononucleotide adenylyltransferase) to yield nicotinic acid adenine dinucleotide (NAAD).
- NAAD is amidated by NAD synthetase to yield NAD+.
NAD+ is the universal redox cofactor of cellular metabolism. It accepts electrons from glycolysis, the TCA cycle, beta-oxidation, and other oxidative reactions to become NADH, which then donates those electrons to the electron transport chain to drive ATP synthesis. The NAD+/NADH ratio is one of the most fundamental homeostatic variables in cellular biology.
Beyond its redox role, NAD+ is consumed (not just shuffled) by three classes of enzymes:
- Sirtuins (SIRT1-7) — NAD+-dependent deacetylases involved in metabolic regulation, mitochondrial biogenesis, DNA repair, and longevity signaling. The sirtuin family is the cellular sensor that translates NAD+ availability into transcriptional and post-translational regulation.
- Poly(ADP-ribose) polymerases (PARPs) — consume NAD+ in DNA damage repair, particularly single-strand break repair. Heavy DNA damage (oxidative stress, ionizing radiation) can deplete cellular NAD+ through PARP overactivation.
- CD38 and other NADases — consume NAD+ in calcium signaling and immune function. CD38 expression rises with age and is one proposed contributor to age-related NAD+ decline.
This three-way consumption is why steady-state NAD+ depends on continuous biosynthesis. Tryptophan-derived de novo NAD+ biosynthesis is one of three input pathways (preformed niacin via the Preiss-Handler pathway is the second; nicotinamide salvage via NAMPT is the third). The de novo pathway becomes quantitatively important when preformed niacin intake is low — the pellagra setting.
The contemporary interest in nicotinamide riboside (NR) and nicotinamide mononucleotide (NMN) as anti-aging supplements is rooted in this same biology — they are alternative substrates for NAD+ biosynthesis that bypass parts of the de novo pathway. See our Vitamin B3 (Niacin) page for more on the contemporary niacin / NAD+ supplement landscape.
The Pellagra Epidemic — Corn, the American South, and the 4 D's
Pellagra is the niacin-deficiency disease. The clinical presentation is classically summarized as the "4 D's": Dermatitis (a characteristic sunlight-exposed photosensitive rash on the face, neck, and forearms called Casal's necklace), Diarrhea, Dementia (progressing through irritability, anxiety, confusion, and ultimately frank psychosis or stupor), and — if untreated — Death. The disease was endemic in maize-eating populations of southern Europe and the Mediterranean for centuries before it exploded in the American South in the late 19th and early 20th centuries.
The American epidemic was concentrated in poor sharecropper and mill-worker communities whose diet was dominated by what was then called the "3M diet" — meat (specifically fatback or salt pork), molasses, and meal (cornmeal). Fresh vegetables, dairy, eggs, and lean meat were scarce. The result was a population subsisting on calories that were severely inadequate for niacin and tryptophan content. By the 1910s, pellagra was killing tens of thousands of Americans per year. The South Carolina State Hospital alone reported 1,500 pellagra deaths in 1915.
The disease was initially blamed on infection (the working hypothesis at the time was that maize contained or hosted some kind of microbial toxin or zymotic agent), and entire careers were spent trying to identify the supposed pathogen. The truth turned out to be a nutritional deficiency that nobody had yet imagined, and demonstrating that took a public health campaign of extraordinary patience and political courage.
Joseph Goldberger and the End of Pellagra
Joseph Goldberger was a US Public Health Service epidemiologist assigned in 1914 to investigate the Southern pellagra epidemic. He was a Hungarian-born Jewish physician working in a profoundly racist political environment in the deep South, where pellagra was widely understood by local elites as evidence of the moral and racial inferiority of poor whites and Black Americans rather than as a structural consequence of their diet and poverty.
Goldberger's field epidemiology was incisive. He noticed that the staff in orphanages, mental hospitals, and prisons where pellagra was epidemic almost never developed the disease themselves — even when they shared the same building, water supply, and broad living conditions as the patients. The crucial difference was diet: staff ate fresh meat, eggs, milk, and vegetables, while inmates ate the corn-and-molasses ration. This was not consistent with any infectious hypothesis.
Goldberger then ran a series of experiments that would not pass any modern ethics review but which definitively proved the dietary hypothesis:
- He selected Mississippi state-prison inmates (offered pardons in exchange) and put them on the 3M cornmeal diet for several months. Multiple prisoners developed unmistakable pellagra. None of the controls eating mixed diets did.
- He performed self-experiments and "filth parties" with his wife and colleagues, deliberately inoculating themselves and each other with scabs, blood, urine, feces, and other body fluids from active pellagra patients. None of them got pellagra. This single dramatic gesture finally killed the infectious-agent hypothesis.
- He treated orphanage outbreaks by adding milk, eggs, and lean meat to the diet, and the pellagra resolved — even though no other intervention had been made.
Goldberger correctly inferred that a deficiency factor in the typical Southern diet was responsible. He called it the "P-P factor" (pellagra-preventive factor). He died in 1929 (of cancer, not pellagra) before the specific nutrient was identified. Conrad Elvehjem at the University of Wisconsin identified the P-P factor as niacin (nicotinic acid) in 1937 by curing black-tongue (the dog version of pellagra) with niacin extracts. Within a decade, the US fortified wheat flour and cornmeal with niacin, and pellagra essentially vanished from the American disease landscape.
Pellagra remains a problem today in refugee populations subsisting on maize aid, in some traditional cuisines that lean heavily on un-treated corn, and in alcoholic populations whose nutritional intake is severely compromised (alcohol increases niacin requirements through multiple mechanisms). It is also a recognized presentation of carcinoid syndrome (tryptophan diversion to serotonin), of inflammatory bowel disease (malabsorption), and of certain rare genetic conditions including Hartnup disease.
Why Corn Is the Pellagra Trigger
The mystery that perplexed nineteenth-century investigators was why corn specifically was associated with pellagra when other grains were not. Wheat, rice, oats, and barley all support populations that do not develop pellagra. Corn does. Why?
The answer is a combination of two corn-specific facts:
- Corn is unusually low in tryptophan among the cereal grains. The principal corn protein is zein, which has essentially no tryptophan and very little lysine. A corn-dominated diet provides little tryptophan to be converted to niacin equivalents. By contrast, wheat protein (gliadin + glutenin) has modest but adequate tryptophan content.
- The niacin that is present in corn is bound in an insoluble complex called niacytin. Human digestion cannot efficiently liberate niacin from niacytin under acidic conditions. The niacin that the food composition tables credit to corn is essentially nutritionally invisible without specific processing.
The combination is uniquely bad. A diet dominated by untreated corn has neither enough preformed bioavailable niacin nor enough tryptophan to make up the difference via the kynurenine pathway. Niacin deficiency develops within weeks to months on such a diet.
Nixtamalization — Mesoamerican Wisdom
Pellagra was never endemic among the Mesoamerican civilizations (Olmec, Maya, Aztec) where corn originated and where corn dominated the diet for thousands of years. The reason is a traditional pre-cooking processing technique called nixtamalization (from the Nahuatl nextli, "ashes," + tamalli, "dough").
In nixtamalization, dried corn kernels are simmered and steeped in an alkaline solution — traditionally limewater (calcium hydroxide), wood ash slurry, or seashell ash. The alkaline treatment does several biochemically important things:
- It hydrolyzes niacytin and releases bound niacin, making the niacin bioavailable. Nixtamalized corn provides several-fold more absorbable niacin than untreated corn.
- It softens and partially gelatinizes the corn endosperm and loosens the pericarp, making the kernel easier to grind into masa dough.
- It improves the amino acid profile somewhat (modest reductions in the otherwise-significant excess of leucine over tryptophan, which is implicated in some of the pellagra pathophysiology).
- It produces a characteristic flavor and color that defines traditional Mesoamerican cuisine — the corn tortilla, the tamale, the masa-based hominy preparations.
European settlers in the Americas adopted corn as a staple crop but generally did not adopt nixtamalization — they ground corn directly into untreated cornmeal in the European style. The pellagra epidemic that followed (first in Italy in the 1700s where corn from the New World had become a peasant staple, then in the American South) is a striking example of a cultural-knowledge gap producing a population-scale nutritional disease.
The modern American food supply addresses corn's niacin problem through fortification of cornmeal, corn flour, and grits with synthetic niacin. Traditional Mexican cuisine and its derivatives address the same problem through nixtamalization. Either solution prevents pellagra. The original Southern 3M diet had neither.
Hartnup Disease — The Genetic Form
Hartnup disease is an autosomal recessive disorder of neutral amino acid transport caused by mutations in the SLC6A19 gene, which encodes the apical brush-border B(0)AT1 transporter in the intestinal epithelium and the proximal renal tubule. The transporter normally absorbs the neutral amino acids (alanine, serine, threonine, valine, leucine, isoleucine, phenylalanine, tyrosine, tryptophan, glutamine, asparagine, histidine, cysteine, citrulline) from the intestinal lumen and reclaims them from the glomerular filtrate. Loss of function impairs both intestinal absorption and renal reabsorption of these amino acids.
Patients with Hartnup disease excrete large quantities of neutral amino acids in the urine (the diagnostic finding on amino-acid chromatography) and have reduced intestinal absorption. Tryptophan is among the most clinically consequential casualties — the marginal absorption combined with bacterial conversion of unabsorbed tryptophan into indolic metabolites in the colon produces a functional tryptophan deficiency despite normal dietary intake.
The clinical presentation overlaps significantly with pellagra: a photosensitive Casal's-necklace rash on sun-exposed skin, cerebellar ataxia and neurological symptoms (intermittent confusion, double vision, headache), and emotional lability. Symptoms classically wax and wane in episodes triggered by stress, intercurrent illness, sunlight, or poor diet. Many patients are asymptomatic between episodes; some are diagnosed only incidentally on newborn screening or family workup.
Treatment is gratifyingly simple: oral niacin (nicotinamide) supplementation at typical pediatric doses (50–200 mg/day) usually resolves the rash, the ataxia, and the mood symptoms. A high-protein diet that provides excess tryptophan helps offset the absorption defect. Sun protection (clothing, sunscreen) prevents the dermatitis from being triggered by UV exposure.
Hartnup disease is the cleanest illustration of how the tryptophan-niacin axis works in human metabolism. The genetic absorption defect produces the same downstream disease (pellagra) as the dietary tryptophan/niacin double-deficiency in the historic Southern epidemic.
The Kynurenic vs Quinolinic Branches
The most clinically important contemporary aspect of the kynurenine pathway is the branchpoint at L-kynurenine, which can be processed in either of two directions with strikingly different biological consequences:
- Kynurenic acid (produced by kynurenine aminotransferase, KAT) is a glutamate NMDA receptor antagonist and a 7-nicotinic-acetylcholine-receptor antagonist. It is broadly neuroprotective and is the "good" branch. Astrocytes are the principal producers of kynurenic acid in the brain.
- Quinolinic acid (produced through the kynurenine-3-monooxygenase route) is a glutamate NMDA receptor agonist and at elevated concentrations a frank excitotoxin. It is also a free-radical generator. Activated microglia and macrophages are the principal producers of quinolinic acid in the inflamed brain.
The ratio of kynurenic to quinolinic acid in the brain is therefore a kind of biochemical scoreboard of neuroprotection-versus-neurotoxicity within the kynurenine pathway. Inflammation tilts the balance toward quinolinic acid — the microglial KMO enzyme is upregulated, more kynurenine is funneled toward the quinolinic branch, and the kynurenic / quinolinic ratio falls. This biology is now a major focus of psychiatric and neurological research:
- Major depressive disorder — meta-analyses show modestly reduced kynurenic-to-quinolinic ratios in depressed patients compared to controls.
- Suicidal ideation — Erhardt and colleagues reported elevated CSF quinolinic acid in patients with suicide attempts, with normalization over recovery time.
- Schizophrenia — paradoxically elevated kynurenic acid in some patients (a possible contributor to the NMDA-hypofunction model of psychosis).
- Alzheimer's disease — quinolinic acid is elevated in cortical regions affected by amyloid pathology, contributing to the excitotoxic component of neurodegeneration.
- Huntington's disease — selective quinolinic-acid toxicity to striatal medium spiny neurons is one of the cellular models of the disease.
The pharmacological implication is that KMO inhibitors (blocking the conversion of kynurenine to 3-hydroxykynurenine and shunting flux to kynurenic acid instead) are an active drug-discovery target for both psychiatric and neurodegenerative disease. Several KMO inhibitors are in early clinical development.
The deep-dive on the cognitive-function side of this biology is in the companion page: Tryptophan and Cognitive Function.
Modern Clinical Significance
- Adequate niacin status in mixed-diet adults — the typical American diet provides 25–50 mg of niacin equivalents per day, well above the 14–16 mg/day RDA. Frank pellagra is rare in the US except in alcoholics, in patients with carcinoid syndrome, and in advanced IBD.
- Niacin requirements in inflammation — chronic inflammation (rheumatoid arthritis, inflammatory bowel disease, hepatitis C) diverts tryptophan to kynurenine and may increase niacin requirements modestly. This is rarely clinically significant but is part of the rationale for B-complex supplementation in chronic inflammatory conditions.
- Carcinoid syndrome and pellagra — serotonin-secreting carcinoid tumors divert up to 50% of dietary tryptophan into serotonin/5-HIAA production. The de novo niacin synthesis falls, and patients can develop pellagra-like symptoms. Niacin supplementation is routinely added to carcinoid management.
- Alcoholic pellagra encephalopathy — described by Jolliffe in the 1940s. Chronic alcoholism produces niacin deficiency through poor diet, impaired absorption, and accelerated catabolism. Presents with confusion, oculogyric symptoms, and gait disturbance. Treated with parenteral niacin (often included in "banana bag" thiamine-folate-niacin replacement protocols).
- Niacin (high-dose) for dyslipidemia — pharmacologic high-dose niacin (1–3 g/day) lowers LDL cholesterol and triglycerides and raises HDL. This use is independent of any tryptophan-niacin biology and is now less commonly prescribed than the statin class, but it remains an option in specific clinical scenarios. See Vitamin B3 (Niacin) for details.
- NAD+ precursor supplementation — nicotinamide riboside (NR) and nicotinamide mononucleotide (NMN) are increasingly used as anti-aging supplements based on the hypothesis that cellular NAD+ declines with age and that boosting NAD+ improves mitochondrial function and sirtuin activity. The clinical evidence is still emerging.
Cautions and Cofactor Notes
- The pathway is vitamin B6 dependent. Kynureninase (the kynurenine-to-anthranilate step) requires pyridoxal-5-phosphate. B6 deficiency produces functional niacin deficiency even with adequate dietary tryptophan, and elevated urinary xanthurenic acid is the classic biomarker (xanthurenic acid accumulates upstream of the B6-dependent step). Anyone supplementing tryptophan for any reason should ensure adequate B6 intake.
- The pathway is vitamin B2 (riboflavin) dependent. Kynurenine 3-monooxygenase (KMO) contains a flavin prosthetic group. Severe riboflavin deficiency impairs the pathway.
- The pathway is iron dependent. IDO and TDO are both heme-containing dioxygenases.
- High-dose pharmacologic niacin causes flushing (prostaglandin-D2-mediated cutaneous vasodilation). This is unrelated to tryptophan biology but is the dose-limiting side effect of niacin used for dyslipidemia. Extended-release formulations and aspirin pretreatment reduce flushing.
- High-dose pharmacologic niacin can cause hepatotoxicity, especially the sustained-release formulations. Liver function should be monitored on chronic high-dose niacin therapy.
- Tryptophan supplementation alone will not treat pellagra if niacin requirements are acutely high (active alcoholism, carcinoid, advanced malabsorption). Direct niacin (nicotinamide or niacin) replacement is more efficient and faster.
Key Research Papers
- Goldberger J (1914). The etiology of pellagra: the significance of certain epidemiological observations with respect thereto. Public Health Reports. — PubMed
- Elvehjem CA et al. (1937). Relation of nicotinic acid and nicotinic acid amide to canine black tongue. Journal of the American Chemical Society. — PubMed
- Krehl WA et al. (1945). Growth-retarding effect of corn in nicotinic acid-low rations and its counteraction by tryptophan. Science 101:489–490. — PubMed
- Horwitt MK et al. (1956). Tryptophan-niacin relationships in man. Journal of Nutrition. — PubMed
- Bender DA, Olufunwa R (1988). Utilization of tryptophan, nicotinamide and nicotinic acid as precursors for nicotinamide nucleotide synthesis in isolated rat liver cells. British Journal of Nutrition. — PubMed
- Levy HL (2001). Hartnup disorder. In: The Metabolic and Molecular Bases of Inherited Disease. — PubMed
- Kleta R et al. (2004). Mutations in SLC6A19, encoding B0AT1, cause Hartnup disorder. Nature Genetics 36:999–1002. — PubMed
- Schwarcz R, Bruno JP, Muchowski PJ, Wu HQ (2012). Kynurenines in the mammalian brain: when physiology meets pathology. Nature Reviews Neuroscience 13:465–477. — PubMed
- Stone TW, Darlington LG (2002). Endogenous kynurenines as targets for drug discovery and development. Nature Reviews Drug Discovery 1:609–620. — PubMed
- Carpenter KJ (1981). Pellagra. Hutchinson Ross historical series. — PubMed
- Carcinoid syndrome and tryptophan-niacin depletion case series — PubMed
- Wall RA, Mertz ET (1945). Studies on the vitamin content of tortillas. Journal of Nutrition. — PubMed
PubMed Topic Searches
- PubMed: Tryptophan to niacin equivalent conversion
- PubMed: Pellagra history and niacin deficiency
- PubMed: Hartnup disease
- PubMed: Kynurenine pathway in brain
- PubMed: Nixtamalization and corn niacin
Connections
- Tryptophan Overview
- Tryptophan Benefits Hub
- Tryptophan for Sleep
- Tryptophan for Mood
- Tryptophan and Cognition
- Vitamin B3 (Niacin)
- Vitamin B6 (Kynureninase Cofactor)
- All Vitamins
- All Amino Acids
- Inflammatory Bowel Disease
- Depression
- Food Index
- All Minerals
- Iron (Dioxygenase Cofactor)
- Brain Fog