Vitamin E and Heart Health
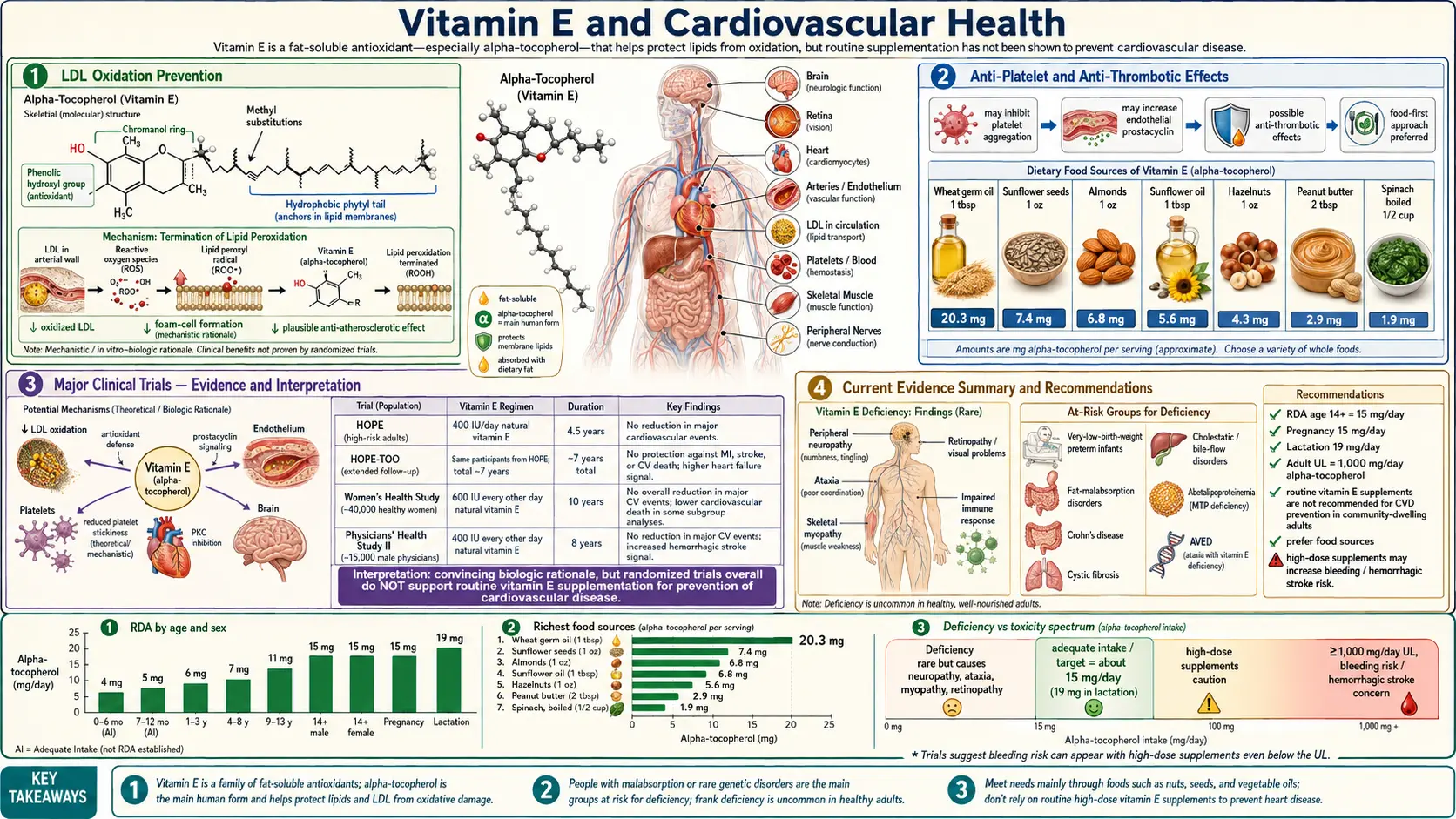
Table of Contents
- Overview
- Vitamin E Forms and Why Alpha-Tocopherol Alone Misled Us
- Mechanism — Lipid Peroxidation and LDL Oxidation
- Gamma-Tocopherol and Reactive Nitrogen Species
- Tocotrienols and Cholesterol
- Major Cardiovascular RCTs in Context
- Modern Evidence — Subgroups That Benefit
- Vitamin E and Atherosclerosis Progression
- Practical Dosing and Form
- Cautions and Drug Interactions
- References
- Connections
- Featured Videos
Overview
For three decades, vitamin E was the antioxidant of the century — the fat-soluble vitamin that would quench free radicals, stop the oxidation of LDL cholesterol, and rescue arteries from atherosclerotic plaque. Observational studies from the early 1990s, most prominently the Nurses' Health Study and the Health Professionals Follow-up Study, reported that men and women in the highest quintile of vitamin E intake had roughly a 30 to 40 percent lower risk of coronary heart disease compared to the lowest quintile. Two decades later, the picture is dramatically more complicated — and dramatically more interesting.
Between 1994 and 2005, a series of large randomized controlled trials — ATBC, CHAOS, GISSI-Prevenzione, HOPE, HOPE-TOO, and the Women's Health Study — tested high-dose synthetic dl-alpha-tocopherol against placebo for cardiovascular endpoints. The results landed somewhere between disappointing and disturbing. HOPE found no benefit. GISSI-Prevenzione was essentially null. ATBC suggested a possible increase in hemorrhagic stroke. By 2005 the Annals of Internal Medicine meta-analysis suggested that doses above 400 IU per day of synthetic alpha-tocopherol might modestly increase all-cause mortality. The professional societies pulled back. Vitamin E went from miracle to malpractice in less than a decade.
The modern, evidence-aware answer is more nuanced than either extreme. The trials did not test vitamin E. They tested one synthetic isomer of one of vitamin E's eight natural forms, given in pharmacologic doses, to mixed populations, mostly without their natural partners (gamma-tocopherol, the four tocotrienols, vitamin C, selenium). The form mattered. The matrix mattered. The population mattered. The dose mattered. When you look at subgroups defined by haptoglobin genotype, at trials of mixed natural tocopherols, at the emerging tocotrienol literature, and at food-derived vitamin E intake, a more sensible picture emerges — one that is neither "antioxidant cure-all" nor "supplement that kills." This page lays out that picture.
Vitamin E Forms and Why Alpha-Tocopherol Alone Misled Us
"Vitamin E" is not one molecule. It is a family of eight structurally related fat-soluble compounds, all biosynthesized only by photosynthetic organisms (plants, algae, some cyanobacteria) and acquired by humans entirely through diet.
- Four tocopherols – alpha-, beta-, gamma-, and delta-tocopherol. These have a saturated 16-carbon phytyl side chain attached to a chromanol head. They differ in the number and position of methyl groups on the chromanol ring.
- Four tocotrienols – alpha-, beta-, gamma-, and delta-tocotrienol. Same head, but with an unsaturated farnesyl tail (three double bonds in the side chain). The tails sit differently in cell membranes and give tocotrienols mechanistic properties that alpha-tocopherol does not have.
- Natural vs synthetic alpha-tocopherol – Natural RRR-alpha-tocopherol (sometimes labeled d-alpha-tocopherol) has a single stereoisomer at three chiral centers. Synthetic all-rac-alpha-tocopherol (labeled dl-alpha-tocopherol) is an equal mix of eight stereoisomers, only one of which is the natural form. The natural form is preferentially retained by the liver's alpha-tocopherol transfer protein (alpha-TTP), giving it roughly twice the bioavailability of the synthetic mixture per unit weight.
- Why most trials used synthetic alpha alone – In the 1990s, synthetic dl-alpha-tocopherol was the cheapest, most stable, and most standardized form available. It gave a clean active-versus-placebo comparison. The cardiovascular RCTs of that era almost universally used 400 IU, 800 IU, or even 2,000 IU of synthetic alpha-tocopherol as a single agent.
- The displacement problem – High-dose supplemental alpha-tocopherol displaces gamma-tocopherol from cell membranes and from circulation. Plasma gamma-tocopherol falls by 30 to 50 percent within weeks of starting a high-dose alpha-tocopherol regimen. Since gamma-tocopherol carries distinct biological activity that alpha-tocopherol lacks (see next section), high-dose alpha-only supplementation may actually subtract a beneficial molecule while adding a less useful one.
- Implication for trial interpretation – The major cardiovascular RCTs did not test "vitamin E." They tested a particular intervention — pharmacologic dl-alpha-tocopherol monotherapy — that is almost the opposite of the food-pattern intake (mixed tocopherols, mostly gamma in the U.S. diet) that the observational studies had been measuring. The null result is consistent with both possibilities: vitamin E does nothing for the heart, or the specific intervention tested was the wrong one. The evidence since 2000 increasingly favors the second interpretation.
Mechanism — Lipid Peroxidation and LDL Oxidation
The proposed cardioprotective mechanism of vitamin E starts inside the LDL particle and ends with the foam cell that builds atherosclerotic plaque.
- Chain-breaking antioxidant – Alpha-tocopherol's chromanol hydroxyl donates a hydrogen atom to a lipid peroxyl radical, neutralizing the radical and stopping the chain reaction of lipid peroxidation. The resulting tocopheroxyl radical is relatively stable and can be regenerated back to alpha-tocopherol by ascorbate (vitamin C), coenzyme Q10, glutathione, and other reductants. This is the classic "alpha-tocopherol is the front-line membrane antioxidant" picture taught in undergraduate biochemistry.
- Location matters – Alpha-tocopherol partitions into the phospholipid bilayer of cell membranes and into the surface monolayer of lipoprotein particles, including LDL. Each LDL particle carries roughly 6 to 12 alpha-tocopherol molecules, sitting at the lipid-water interface where peroxyl radicals attack the polyunsaturated fatty acids of the phospholipid surface.
- The oxidized-LDL hypothesis – Daniel Steinberg and colleagues at UC San Diego proposed in the late 1980s that native LDL is not particularly atherogenic. What drives atherosclerosis is oxidized LDL, which is taken up unregulated by macrophage scavenger receptors (CD36, SR-A), turning macrophages into cholesterol-loaded foam cells — the cellular signature of early atherosclerotic lesions. By this logic, anything that prevents LDL oxidation should slow atherogenesis. Vitamin E, sitting on the LDL surface, looked like the perfect candidate.
- Why the hypothesis was incomplete – Oxidized LDL is real, and it does promote foam-cell formation. But atherosclerosis involves many parallel processes — endothelial dysfunction, smooth muscle proliferation, inflammation, NLRP3 inflammasome activation, neutrophil extracellular traps, oxidized phospholipids signaling through TLR4 — and blocking one path with one antioxidant is unlikely to halt the disease. Alpha-tocopherol also fails to neutralize all oxidants. It is poor at scavenging reactive nitrogen species (peroxynitrite, NO2), which are major contributors to vascular inflammation and which gamma-tocopherol is better positioned to handle.
- Tocopherol-vitamin C recycling – Vitamin E and vitamin C work as a redox pair. Vitamin C in the aqueous phase regenerates oxidized vitamin E at the lipid-water interface. In experimental models, the cardioprotective effect of vitamin E is markedly enhanced when vitamin C is present at adequate levels, and high-dose vitamin E without adequate vitamin C can actually become pro-oxidant by leaving the membrane saturated with tocopheroxyl radicals that have no partner to recycle them. This is one mechanistic explanation for the disappointing results of alpha-tocopherol monotherapy.
Gamma-Tocopherol and Reactive Nitrogen Species
Gamma-tocopherol is the dominant form of vitamin E in the typical U.S. diet, largely because soybean oil, corn oil, and other commonly consumed seed oils are gamma-tocopherol rich. Plasma gamma-tocopherol concentrations in untreated Americans are typically 2 to 4 micromolar, while plasma alpha-tocopherol is around 25 to 35 micromolar. The natural ratio matters — and high-dose alpha-tocopherol supplementation disrupts it.
- Chemistry advantage – Gamma-tocopherol's chromanol ring has an unmethylated 5-position, giving it a structural feature that alpha-tocopherol lacks: the ability to trap reactive nitrogen species. When peroxynitrite (ONOO-) or nitrogen dioxide (NO2) attacks the 5-position, gamma-tocopherol forms 5-nitro-gamma-tocopherol — the same reaction does not occur with alpha-tocopherol because that position is already methylated. The body's plasma 5-nitro-gamma-tocopherol level is therefore a biomarker of in vivo reactive nitrogen species exposure.
- Relevance to atherosclerosis – Reactive nitrogen species are heavily implicated in endothelial dysfunction, vascular inflammation, and plaque instability. Macrophages and neutrophils generate peroxynitrite via the simultaneous production of superoxide and nitric oxide, especially in inflamed vessel walls. By neutralizing these species, gamma-tocopherol may protect against vascular inflammation in a way that alpha-tocopherol cannot.
- Anti-inflammatory effects – Gamma-tocopherol and its major metabolite gamma-CEHC (2,7,8-trimethyl-2-(beta-carboxyethyl)-6-hydroxychroman) suppress cyclooxygenase-2 (COX-2) activity, reducing prostaglandin E2 production in macrophages and epithelial cells. Several preclinical studies show that gamma-tocopherol-rich mixed tocopherol preparations reduce C-reactive protein, IL-6, and TNF-alpha in inflammation models — effects that pure alpha-tocopherol either lacks or shows weakly.
- The displacement issue, restated – Qing Jiang, Maret Traber, Bruce Ames, and colleagues showed in the 2000s that high-dose alpha-tocopherol supplementation depletes plasma and tissue gamma-tocopherol by 30 to 50 percent. If gamma-tocopherol is doing protective work, then trials of alpha-tocopherol monotherapy may have inadvertently removed the very molecule that mattered. This is a leading hypothesis for why mixed natural tocopherols outperform pure alpha-tocopherol in many surrogate-endpoint cardiovascular studies.
- Wagner et al. review – A 2008 review by Wagner, Kamal-Eldin, and Elmadfa in Annals of Nutrition and Metabolism summarized the gamma-tocopherol literature and argued that the food-pattern observational data were closer to a test of "all tocopherols, gamma-rich" while the RCTs were closer to a test of "pure alpha at pharmacologic dose, gamma depleted." The two interventions were essentially different molecules, and there is no logical inconsistency in observing benefit from the first and null from the second.
Tocotrienols and Cholesterol
Tocotrienols are the four-double-bond cousins of tocopherols. They are concentrated in the bran of rice and barley, in palm oil, and most cleanly in annatto seed extract (which is essentially pure delta- and gamma-tocotrienol with no tocopherol contamination). Tocotrienols have a different set of bioactivities than tocopherols — some of them clinically relevant for cardiovascular disease.
- HMG-CoA reductase suppression – A. Asaf Qureshi and colleagues showed in the 1980s and 1990s that delta- and gamma-tocotrienol post-transcriptionally suppress HMG-CoA reductase, the rate-limiting enzyme in cholesterol biosynthesis — the same target as statin drugs, but through a different molecular mechanism. Tocotrienols increase the rate of HMG-CoA reductase degradation and reduce its translation, lowering hepatic cholesterol synthesis. The effect is selective for delta- and gamma-tocotrienol; alpha-tocopherol actually antagonizes this effect, which is why tocopherol-rich tocotrienol preparations (e.g., from palm oil) produce smaller lipid effects than tocopherol-free annatto preparations.
- Annatto-source tocotrienol research – The cleanest tocotrienol RCTs use annatto-source delta- and gamma-tocotrienol (DeltaGold and related preparations), typically dosed at 125 to 300 mg per day. Trials by Barrie Tan, Chandan Sen, and others have reported total cholesterol reductions of 10 to 17 percent and LDL reductions of 10 to 24 percent, alongside reductions in C-reactive protein and improvements in endothelial function. The effect size is modest compared to statins, but the safety profile is excellent and the mechanism is complementary.
- Anti-inflammatory and endothelial effects – Tocotrienols suppress NF-kB activation in endothelial cells, reduce VCAM-1 and ICAM-1 expression (the adhesion molecules that recruit monocytes to the vessel wall), and improve flow-mediated dilation. These are mechanistically relevant for the earliest stages of atherosclerosis, before lipid accumulation begins.
- Why tocotrienols are not in the major cardiovascular RCTs – The 1990s and early-2000s mega-trials predate the modern tocotrienol literature and used tocopherol preparations only. There is no HOPE-scale RCT of tocotrienols and hard cardiovascular endpoints (MI, stroke, cardiovascular death). What exists is a moderate-quality literature of surrogate-endpoint trials (lipids, inflammation, IMT, flow-mediated dilation) suggesting benefit, plus mechanistic plausibility. This is a reasonable basis for considering mixed tocopherol + tocotrienol preparations, but not for claiming that hard-endpoint efficacy has been proven.
- Sen and Khanna alpha-tocotrienol neuroprotection – Chandan Sen and Savita Khanna's work at Ohio State showed that alpha-tocotrienol at nanomolar concentrations protects neurons from glutamate-induced excitotoxicity through a mechanism distinct from alpha-tocopherol's antioxidant action — specifically by suppressing 12-lipoxygenase and c-Src activation. While the primary application is stroke, the same vascular-protective biology is relevant for atherosclerotic disease.
Major Cardiovascular RCTs in Context
The cardiovascular RCTs of the 1990s and early 2000s are the historical reason vitamin E acquired its current "doesn't work and may be harmful" reputation. Understanding what they actually tested — and what they did not test — is essential to interpreting modern evidence.
- ATBC (Alpha-Tocopherol, Beta-Carotene Cancer Prevention Study), 1994 – 29,133 Finnish male smokers, 50 mg per day dl-alpha-tocopherol versus placebo, mean 6.1 years. Designed for lung cancer endpoint; cardiovascular events were secondary. No reduction in coronary mortality. A statistically significant increase in hemorrhagic stroke in the alpha-tocopherol arm (50% relative increase, small absolute number) raised the first major safety signal.
- CHAOS (Cambridge Heart Antioxidant Study), 1996 – 2,002 patients with angiographically proven coronary atherosclerosis, randomized to 400 or 800 IU per day natural alpha-tocopherol or placebo. Median follow-up 510 days. CHAOS reported a striking 47% reduction in nonfatal myocardial infarction in the vitamin E arm (relative risk 0.23). It remains the only major secondary-prevention RCT with a clearly positive primary endpoint. The trial was small, short, and used the natural RRR form rather than synthetic. Subsequent larger trials did not reproduce the magnitude.
- GISSI-Prevenzione, 1999 – 11,324 Italian patients within 3 months of myocardial infarction, randomized 2x2 to 300 mg per day synthetic vitamin E, 1 g per day omega-3 (EPA+DHA), both, or neither. The omega-3 arm reduced cardiovascular mortality; the vitamin E arm did not reach statistical significance for the primary combined endpoint. A factorial analysis suggested a modest reduction in cardiovascular death with vitamin E, but the trial is generally read as null.
- HOPE (Heart Outcomes Prevention Evaluation), 2000 – 9,541 patients with vascular disease or diabetes plus one additional risk factor, randomized to 400 IU per day natural alpha-tocopherol or placebo for 4.5 years. HOPE was the methodologically cleanest, largest, and most-quoted of the trials. The primary outcome (composite of myocardial infarction, stroke, and cardiovascular death) showed no benefit (RR 1.05, 95% CI 0.95-1.16). HOPE-TOO, a 2.5-year extension, similarly showed no benefit and a small increase in heart-failure hospitalizations.
- Women's Health Study, 2005 – 39,876 healthy women aged 45 and older, 600 IU natural alpha-tocopherol every other day versus placebo, 10.1 years. Primary endpoint (composite cardiovascular events) showed no significant reduction. A pre-specified secondary endpoint of cardiovascular death was reduced by 24% (RR 0.76, 95% CI 0.59-0.98), but the overall trial is generally classified as null. Notably, the dose was modest (600 IU every other day, roughly 300 IU per day equivalent) and the population was healthy — the absolute event rate was low.
- Why the null results are not the whole story – Every one of these trials tested synthetic or natural alpha-tocopherol as monotherapy. None tested mixed tocopherols. None tested tocotrienols. None pre-stratified on haptoglobin genotype (the strongest known cardiovascular vitamin E responder phenotype, see next section). Most used populations on aggressive secondary-prevention regimens (aspirin, statins, ACE inhibitors, beta-blockers) where the addition of any single antioxidant against an already-heavily-treated background is unlikely to show effect. The trials answered the question they were designed to answer — "does pharmacologic alpha-tocopherol monotherapy added to standard therapy reduce hard cardiovascular endpoints in mixed populations?" — and the answer was no. They did not answer the broader question of whether dietary vitamin E patterns or carefully chosen subgroups might benefit.
Modern Evidence — Subgroups That Benefit
The most important post-HOPE development in vitamin E cardiovascular research is the recognition that pharmacogenomic and metabolic subgroups respond very differently to alpha-tocopherol supplementation. The clearest signal is from the haptoglobin (Hp) genotype literature led by Andrew Levy at Technion.
- The haptoglobin Hp 2-2 phenotype – Haptoglobin is the plasma protein that binds free hemoglobin (released from lysed red cells) and prevents it from acting as a pro-oxidant. There are three common phenotypes: Hp 1-1, Hp 2-1, and Hp 2-2. The Hp 2-2 protein is structurally inferior at neutralizing free hemoglobin; in diabetes, where chronic hyperglycemia promotes hemoglobin release, Hp 2-2 individuals have markedly elevated oxidative stress in the vasculature.
- ICARE trial (Milman, Blum, Levy, 2008) – The Israel Cardiovascular Events Reduction with Vitamin E trial randomized 1,434 Hp 2-2 diabetic patients to 400 IU per day natural alpha-tocopherol or placebo. The intervention reduced the composite cardiovascular endpoint (myocardial infarction, stroke, cardiovascular death) by 53% (HR 0.47, 95% CI 0.27-0.82) over 18 months. The trial was stopped early for efficacy. This is the strongest single-RCT evidence for cardiovascular benefit of vitamin E in any defined population.
- Mechanistic plausibility – Hp 2-2 diabetics have elevated HDL-associated oxidative stress, with dysfunctional HDL that promotes rather than prevents LDL oxidation. Alpha-tocopherol supplementation reverses HDL dysfunction in this specific population, restoring HDL's antioxidant capacity. The same dose has no benefit (and possibly slight harm) in Hp 1-1 diabetics, where HDL is already functional and additional alpha-tocopherol may disturb the redox balance.
- HOPE secondary analysis – Re-analysis of HOPE participants by Hp phenotype showed that the Hp 2-2 diabetic subgroup, which represented roughly 16% of the diabetic participants, had a 43% reduction in cardiovascular events with alpha-tocopherol — replicating the ICARE signal in an independent dataset. The overall null HOPE result therefore conceals a strongly positive subgroup result diluted by neutral and possibly slightly harmful effects in other subgroups.
- Clinical implication – The current state of evidence supports considering 400 IU per day natural alpha-tocopherol for Hp 2-2 diabetic patients as a low-cost, mechanism-based intervention. Haptoglobin phenotyping is inexpensive and clinically available. This is an example of pharmacogenomic medicine applied to a "failed" supplement — an important reminder that population-level RCTs can mask large, real, replicable effects in genetically or metabolically defined subgroups.
- Other potential responder phenotypes – Beyond Hp 2-2 diabetes, candidate responder subgroups under active study include individuals with elevated baseline oxidative stress markers (oxidized LDL, F2-isoprostanes, myeloperoxidase), individuals with low baseline plasma alpha-tocopherol (under 12 micromolar), and individuals with specific apolipoprotein E genotypes. The evidence base is weaker than for Hp 2-2 but mechanistically reasonable.
Vitamin E and Atherosclerosis Progression
Hard endpoints (MI, stroke, cardiovascular death) are not the only relevant outcomes. Atherosclerosis progression measured by carotid intima-media thickness (IMT), coronary artery calcium scoring, and similar surrogate markers gives a more sensitive readout of vascular biology over the timeframes that supplementation trials can practically run.
- Carotid IMT trials – Several small-to-medium RCTs have used carotid IMT progression as the primary endpoint. The VEAPS (Vitamin E Atherosclerosis Prevention Study) randomized 353 men and women aged 40 and older with LDL above 130 mg/dL to 400 IU per day natural alpha-tocopherol or placebo for 3 years. IMT progression was not significantly different between groups, though some sub-analyses suggested modest benefit in subgroups with elevated baseline oxidative stress.
- ARBITER and related trials – The Arterial Biology for the Investigation of the Treatment Effects of Reducing Cholesterol trials evaluated combinations including vitamin E. Niacin-plus-antioxidant cocktails containing vitamin E showed less HDL increase than niacin alone, suggesting potential interference between supplemental alpha-tocopherol and niacin's HDL-raising mechanism — a counterintuitive finding that helped reshape thinking about antioxidant-statin and antioxidant-niacin interactions.
- EPIC-Norfolk plasma observational data – The European Prospective Investigation into Cancer and Nutrition cohort in Norfolk reported that higher plasma alpha-tocopherol concentrations were associated with lower coronary heart disease mortality in dose-response fashion, even after adjustment for traditional risk factors and dietary patterns. Plasma alpha-tocopherol reflects dietary intake plus stable supplementation; it is a different measurement than the pharmacologic spike produced by acute high-dose intervention.
- Mixed tocopherol surrogate-endpoint trials – Several smaller trials of mixed tocopherol preparations (containing gamma- and delta-tocopherol alongside alpha-) report more favorable surrogate-marker results than equivalent-dose pure alpha-tocopherol trials. Effects include reductions in F2-isoprostanes, oxidized LDL, soluble vascular cell adhesion molecule-1, and improvements in flow-mediated dilation. The trials are too small and short for hard-endpoint inference, but they are consistent with the broader mechanistic argument that mixed tocopherols outperform pure alpha.
- The realistic interpretation – Vitamin E supplementation is unlikely to halt atherosclerosis progression as a single intervention in mixed populations. It may modestly slow progression in subgroups with elevated baseline oxidative stress. It may contribute — as part of a broader pattern that includes vitamin C, selenium, omega-3 fatty acids, magnesium, and a low-refined-carbohydrate diet — to vascular biology that is meaningfully different than no intervention at all. None of this constitutes a "vitamin E is proven to prevent heart disease" claim, but it also does not support the popular "vitamin E is useless or harmful" narrative.
Practical Dosing and Form
The contemporary, evidence-aware approach to vitamin E for cardiovascular health prioritizes food first, then carefully chosen supplement form if supplementation is desired, with attention to cofactors.
- Food sources – The highest practical food sources of vitamin E are sunflower seeds (approximately 35 mg of alpha-tocopherol per 100 g, mostly alpha), almonds (26 mg per 100 g, mostly alpha), hazelnuts (15 mg per 100 g), wheat germ oil (149 mg per 100 g, the densest natural source), and avocado (2.6 mg per 100 g). Common U.S. dietary patterns are gamma-tocopherol heavy due to soybean and corn oils. A small daily handful of mixed nuts and seeds will reliably provide 10 to 20 mg of mixed tocopherols in a natural matrix with fiber, magnesium, and the fats needed for absorption.
- If supplementing, choose mixed tocopherols – The mechanistic argument and the modern surrogate-endpoint trials both favor mixed natural tocopherol preparations (containing alpha-, gamma-, and delta-tocopherol) over pure alpha-tocopherol. Quality preparations are labeled "mixed tocopherols" and specify the gamma-tocopherol content (typically 100 to 200 mg per dose). Avoid synthetic dl-alpha-tocopherol monotherapy.
- If supplementing, consider adding tocotrienols – An annatto-source delta- and gamma-tocotrienol preparation at 125 to 300 mg per day adds the cholesterol-modulating and anti-inflammatory bioactivities that tocopherols do not have. Tocopherol and tocotrienol should not be taken at the same meal, since alpha-tocopherol can interfere with tocotrienol absorption; separate by 6 to 8 hours.
- Dose range – The 200 to 400 IU per day range of mixed tocopherols (equivalent to roughly 134 to 268 mg of natural alpha-tocopherol) is supported by trial data and avoids the doses (above 800 IU per day) where the modest mortality signal in the Miller 2005 meta-analysis emerged. Doses above 400 IU per day of synthetic alpha-tocopherol have no demonstrated cardiovascular benefit and a small adverse signal.
- Take with fat – Vitamin E is fat-soluble and requires dietary fat for absorption. Take supplements with a meal containing at least 5 to 10 g of fat. Fasting administration produces erratic and incomplete absorption.
- Cofactor synergy – Selenium is required for the glutathione peroxidase enzymes that work alongside vitamin E to handle lipid hydroperoxides. Vitamin C in the aqueous phase regenerates oxidized vitamin E at the lipid-water interface. Adequate magnesium supports the overall antioxidant defense network. These nutrients are best considered together rather than as individual supplements.
- Rationale against high-dose synthetic alpha – The accumulated evidence weighs strongly against high-dose (above 400 IU per day) synthetic dl-alpha-tocopherol monotherapy. This is the intervention that the major RCTs tested with null results and the meta-analysis flagged for a small mortality signal. There is no longer a serious mechanistic or empirical case for this specific regimen.
Cautions and Drug Interactions
- Warfarin and other anticoagulants – Vitamin E at doses above approximately 400 IU per day has antiplatelet activity and at higher doses appears to antagonize vitamin K-dependent clotting factor synthesis, potentiating the effect of warfarin. Patients on warfarin should keep vitamin E intake stable (food-pattern intake is generally not problematic; high-dose supplements are) and inform their prescriber of any supplementation. INR may need monitoring after supplementation changes.
- Antiplatelet drugs – The combination of high-dose vitamin E with aspirin, clopidogrel, prasugrel, or ticagrelor can additively increase bleeding risk. This is particularly relevant in elderly patients and in patients with prior gastrointestinal bleeding. The increment is small at 200 to 400 IU per day of mixed tocopherols but real and should be discussed with the prescriber.
- Surgery washout – Most surgical teams ask patients to stop vitamin E supplementation 2 weeks before elective surgery to avoid perioperative bleeding. This is a sensible default. Resume after the surgical team clears resumption of normal supplements.
- Statin interaction – The interaction between vitamin E and statins is complex. High-dose vitamin E in combination with simvastatin and niacin appeared to blunt the HDL-raising effect of niacin in the HATS and ARBITER trials — an unexpected adverse signal that helped sour clinician opinion. Statins themselves slightly reduce plasma alpha-tocopherol; the mechanistic interaction goes both ways. The clinical implication is that patients on statins for established coronary disease should not assume that adding high-dose vitamin E will provide additional benefit, and may want to favor food-pattern intake.
- Vitamin K antagonism at high doses – At doses above approximately 1000 IU per day, alpha-tocopherol can interfere with vitamin K-dependent gamma-carboxylation, slightly increasing prothrombin time. This is a dose-dependent effect with no clinical consequence at standard mixed-tocopherol doses but a real concern at the pharmacologic doses (1200 to 2000 IU per day) that have been used in some clinical settings.
- Hemorrhagic stroke signal – The ATBC trial reported a statistically significant increase in hemorrhagic stroke in the alpha-tocopherol arm (small absolute numbers but real signal). The signal is most concerning in male smokers, in older patients with hypertension, and at doses above 400 IU per day. It is less concerning at food-pattern intake and at modest mixed-tocopherol supplementation. Patients with prior hemorrhagic stroke, uncontrolled hypertension, or cerebral amyloid angiopathy should avoid high-dose vitamin E supplementation.
- Mortality meta-analysis context – The Miller 2005 meta-analysis in Annals of Internal Medicine suggested a small increase in all-cause mortality at doses above 400 IU per day. The meta-analysis was dominated by trials in chronically ill populations on multiple medications, and subsequent analyses have suggested the signal may not generalize to healthier populations or to mixed-tocopherol preparations. Nonetheless, the conservative position is that doses above 400 IU per day of synthetic alpha-tocopherol provide no demonstrated cardiovascular benefit and a small possible harm.
This content is provided for informational purposes only and does not constitute medical advice. Consult a qualified healthcare provider before starting any supplementation regimen, particularly when taking anticoagulant, antiplatelet, or lipid-lowering medication, or when planning surgery.
References
The following are landmark and frequently cited peer-reviewed research papers underpinning the claims on this page. Links resolve to the publisher DOI or to PubMed.
- Yusuf S, Dagenais G, Pogue J, Bosch J, Sleight P (HOPE Investigators). Vitamin E supplementation and cardiovascular events in high-risk patients. New England Journal of Medicine. 2000;342(3):154-160. PMID: 10639540.
- GISSI-Prevenzione Investigators. Dietary supplementation with n-3 polyunsaturated fatty acids and vitamin E after myocardial infarction: results of the GISSI-Prevenzione trial. Lancet. 1999;354(9177):447-455. PMID: 10465168.
- The Alpha-Tocopherol, Beta Carotene Cancer Prevention Study Group. The effect of vitamin E and beta carotene on the incidence of lung cancer and other cancers in male smokers. New England Journal of Medicine. 1994;330(15):1029-1035. PMID: 8127329.
- Stephens NG, Parsons A, Schofield PM, Kelly F, Cheeseman K, Mitchinson MJ. Randomised controlled trial of vitamin E in patients with coronary disease: Cambridge Heart Antioxidant Study (CHAOS). Lancet. 1996;347(9004):781-786. PMID: 8622332.
- Lee IM, Cook NR, Gaziano JM, et al. Vitamin E in the primary prevention of cardiovascular disease and cancer: the Women's Health Study: a randomized controlled trial. JAMA. 2005;294(1):56-65. PMID: 15998891.
- Milman U, Blum S, Shapira C, et al. Vitamin E supplementation reduces cardiovascular events in a subgroup of middle-aged individuals with both type 2 diabetes mellitus and the haptoglobin 2-2 genotype: a prospective double-blinded clinical trial. Arteriosclerosis, Thrombosis, and Vascular Biology. 2008;28(2):341-347. PMID: 18032779.
- Levy AP, Gerstein HC, Miller-Lotan R, et al. The effect of vitamin E supplementation on cardiovascular risk in diabetic individuals with different haptoglobin phenotypes. Diabetes Care. 2004;27(11):2767. PMID: 15505023.
- Wagner KH, Kamal-Eldin A, Elmadfa I. Gamma-tocopherol — an underestimated vitamin? Annals of Nutrition and Metabolism. 2004;48(3):169-188. PMID: 15256801.
- Jiang Q, Christen S, Shigenaga MK, Ames BN. Gamma-tocopherol, the major form of vitamin E in the US diet, deserves more attention. American Journal of Clinical Nutrition. 2001;74(6):714-722. PMID: 11722951.
- Sen CK, Khanna S, Roy S. Tocotrienols: vitamin E beyond tocopherols. Life Sciences. 2006;78(18):2088-2098. PMID: 16458936.
- Qureshi AA, Sami SA, Salser WA, Khan FA. Synergistic effect of tocotrienol-rich fraction (TRF(25)) of rice bran and lovastatin on lipid parameters in hypercholesterolemic humans. Journal of Nutritional Biochemistry. 2001;12(6):318-329. PMID: 11516635.
- Miller ER 3rd, Pastor-Barriuso R, Dalal D, Riemersma RA, Appel LJ, Guallar E. Meta-analysis: high-dosage vitamin E supplementation may increase all-cause mortality. Annals of Internal Medicine. 2005;142(1):37-46. PMID: 15537682.
- Steinberg D, Parthasarathy S, Carew TE, Khoo JC, Witztum JL. Beyond cholesterol. Modifications of low-density lipoprotein that increase its atherogenicity. New England Journal of Medicine. 1989;320(14):915-924. PMID: 2648148.
- Lonn E, Bosch J, Yusuf S, et al (HOPE and HOPE-TOO Trial Investigators). Effects of long-term vitamin E supplementation on cardiovascular events and cancer: a randomized controlled trial. JAMA. 2005;293(11):1338-1347. PMID: 15769967.
External Authoritative Resources
- NIH Office of Dietary Supplements — Vitamin E Fact Sheet for Health Professionals
- Linus Pauling Institute — Vitamin E
- Harvard T.H. Chan School of Public Health — The Nutrition Source: Vitamin E
Connections
- All Vitamins
- Vitamin E
- Vitamin E Benefits
- Tocotrienols
- Vitamin C
- Vitamin K
- Vitamin D3
- Vitamin B12
- Selenium
- Magnesium
- Zinc
- Atherosclerosis
- Coronary Artery Disease
- Hypertension
- Berberine
- Homocysteine