NAD+ Precursors Compared: Niacin vs Niacinamide vs NR vs NMN
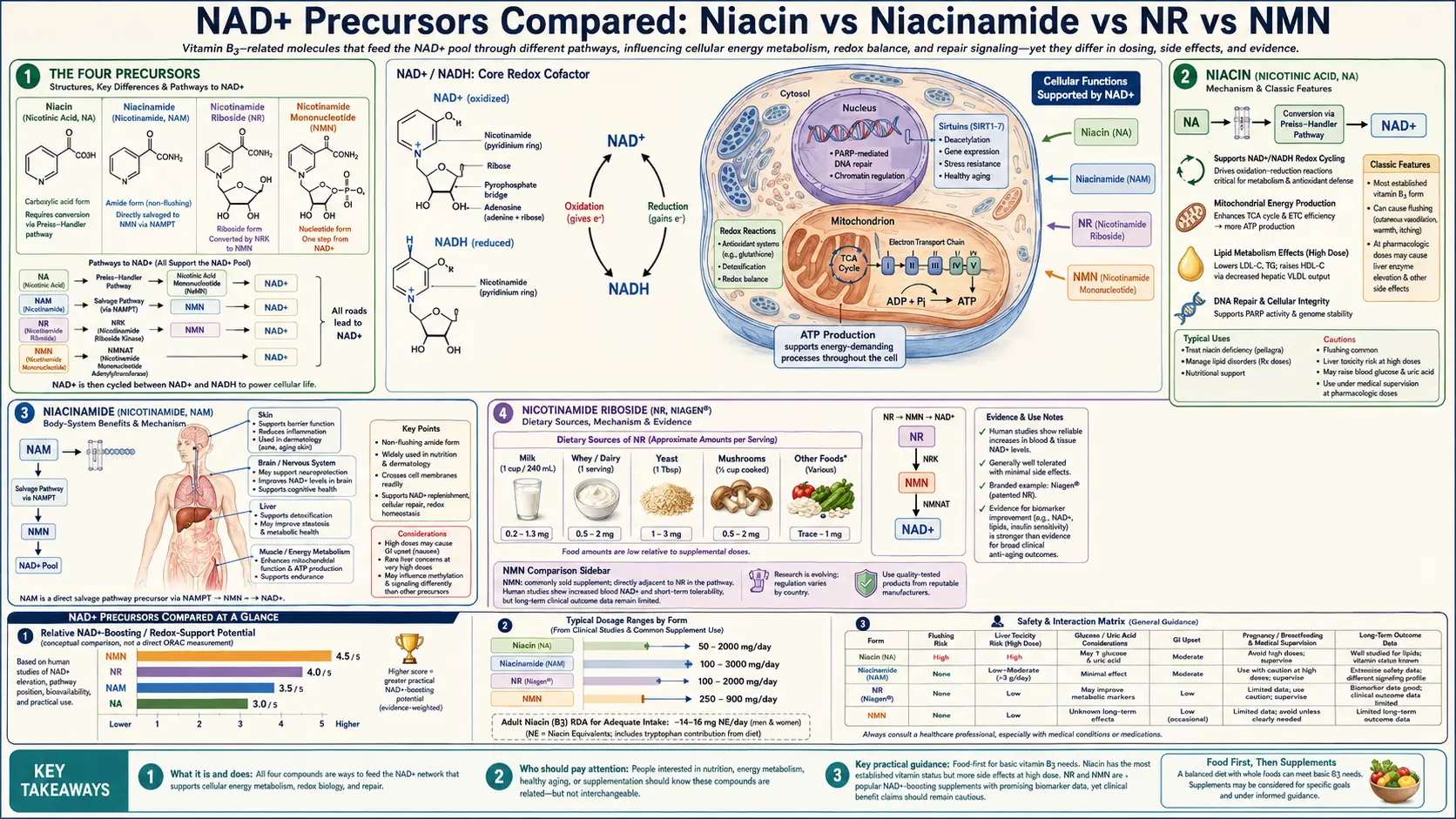
Four molecules can serve as NAD+ precursors in human supplementation: nicotinic acid (niacin, NA), nicotinamide (niacinamide, NAM), nicotinamide riboside (NR), and nicotinamide mononucleotide (NMN). They are all forms of vitamin B3 in the broadest sense, but they differ substantially in absorption, tissue distribution, methylation cost, side-effect profile, regulatory history, price-per-mg, and the strength of their clinical evidence. This deep-dive walks through each molecule, the Brenner-vs-Sinclair NR-vs-NMN debate, the FDA reclassification of NMN in 2022 and the September 2025 reversal, why niacin produces vasodilator flushing while NR and NMN do not, the methylation-cofactor depletion concern, cost-effectiveness comparison, and a practical decision framework for choosing between them.
Table of Contents
- The Four Precursors
- Niacin (Nicotinic Acid, NA)
- Niacinamide (Nicotinamide, NAM)
- Nicotinamide Riboside (NR, Niagen)
- Nicotinamide Mononucleotide (NMN)
- Side-by-Side Comparison Table
- The Niacin Flush — Why It Happens and Why NR/NMN Are Flush-Free
- The Methylation Cofactor Debate (Brenner Critique)
- The Sinclair NMN Advocacy
- The FDA NMN Reclassification (2022) and Reversal (2025)
- Cost-Effectiveness
- A Practical Decision Framework
- Cautions
- Key Research Papers
- Connections
- Featured Videos
The Four Precursors
All four NAD+ precursors share the same downstream destination: incorporation into the cellular NAD+ pool, where they support the electron transport chain, sirtuin activity, PARP DNA repair, and CD38 signaling. They differ in the steps required to get there.
Schematic of the salvage pathway from each precursor to NAD+:
- Niacin (NA) — enters the Preiss-Handler pathway: NA + PRPP → nicotinic acid mononucleotide (NaMN) via NAPRT; NaMN + ATP → nicotinic acid adenine dinucleotide (NaAD) via NMNAT; NaAD + glutamine → NAD+ via NAD synthase
- Niacinamide (NAM) — enters the salvage pathway: NAM + PRPP → NMN via NAMPT (the rate-limiting enzyme); NMN + ATP → NAD+ via NMNAT
- Nicotinamide riboside (NR) — phosphorylated by NR kinase (NRK1, NRK2): NR + ATP → NMN; NMN + ATP → NAD+ via NMNAT
- Nicotinamide mononucleotide (NMN) — converted directly: NMN + ATP → NAD+ via NMNAT (most direct route)
This is why NMN is sometimes called "one step from NAD+": NMN bypasses the NAMPT and NRK steps and feeds directly into the final NMNAT-catalyzed conversion. Whether this directness actually matters in practice depends on whether NMN can enter cells intact, which is the contested question (see Brenner critique below).
Niacin (Nicotinic Acid, NA)
Niacin is the oldest and best-characterized of the four. It was identified as the cure for pellagra in 1937 (Joseph Goldberger's public-health detective work led to the discovery), and it has been a recognized vitamin (vitamin B3) ever since. The pharmaceutical-grade prescription form has been in clinical use for over 60 years, primarily for dyslipidemia.
Clinical effects
- Lowers LDL cholesterol by 10–25% at 1–3 g/day
- Raises HDL cholesterol by 15–35% (the most effective HDL-raising agent known)
- Lowers triglycerides by 20–50%
- Lowers Lp(a) by 20–30% (one of the few interventions that meaningfully lowers Lp(a))
- Treats pellagra (the niacin-deficiency syndrome of dermatitis, diarrhea, dementia, death)
- Raises NAD+ (via the Preiss-Handler pathway)
Drawbacks
- The niacin flush — intense cutaneous vasodilation, burning, and pruritus lasting 30–60 minutes, mediated by GPR109A receptor activation on dermal Langerhans cells and prostaglandin D2 release. Becomes more tolerable with chronic use; can be mitigated by 325 mg aspirin 30 minutes before dosing.
- Hepatotoxicity — rare at standard doses but a real risk with sustained-release formulations and at >3 g/day
- Hyperglycemia — can worsen glucose control in diabetics
- Hyperuricemia — can precipitate gout attacks
- The cardiovascular outcome trials of niacin (AIM-HIGH, HPS2-THRIVE) failed to show benefit when added to statins, despite the favorable lipid changes — calling into question its clinical role in cardiovascular prevention
For NAD+ raising specifically, niacin works but the flushing makes it less practical than NR or NMN. See our Vitamin B3 (Niacin) page and Niacin & Cholesterol for the lipid-focused discussion, and Pellagra for the deficiency syndrome.
Niacinamide (Nicotinamide, NAM)
Niacinamide (the amide form of nicotinic acid) is the form found in most multivitamins and B-complex supplements at the official RDA-level dose of 14–16 mg/day. It also has a long history as a high-dose supplement for specific clinical purposes:
- Type 1 diabetes prevention (historical) — the ENDIT trial of high-dose nicotinamide failed to prevent type 1 diabetes in at-risk children, ending this line of research
- Skin cancer prevention — the ONTRAC trial in New England Journal of Medicine showed that 500 mg nicotinamide twice daily reduced new non-melanoma skin cancers by 23% in high-risk patients
- Topical skin care — widely used in cosmetics at 5% concentration for barrier function and pigmentation
- Raises NAD+ via the salvage pathway through NAMPT (the rate-limiting enzyme)
Advantages
- Cheapest of the four precursors (cents per gram)
- No flushing (no GPR109A activation)
- Generally well tolerated up to 1.5–3 g/day
Drawbacks
- A 2026 head-to-head clinical trial found that NAM did not raise circulating NAD+ as effectively as NR or NMN at equivalent doses, suggesting NAM is the less efficient NAD+ raiser
- NAM at high doses can inhibit sirtuins as a product-inhibitor — it is both a precursor for NAD+ synthesis and a product of NAD+-consuming reactions, so excess NAM may feedback-inhibit SIRT1. This is a theoretical concern more than a documented clinical issue
- Hepatotoxicity at sustained doses >3 g/day
For NAD+-raising purposes specifically, NAM is the least-recommended of the four precursors due to its lower efficiency and theoretical sirtuin inhibition at high doses.
Nicotinamide Riboside (NR, Niagen)
Nicotinamide riboside was characterized as a NAD+ precursor by Charles Brenner's lab in 2004. It is the nucleoside form of NAM — nicotinamide attached to a ribose sugar but without the phosphate group. NR was patented and brought to market as Niagen by ChromaDex starting around 2013, making it the first commercial NAD+ precursor with a strong intellectual property position.
Advantages
- Most clinically studied NAD+ precursor in humans — over 30 published human RCTs as of 2026, with the Martens 2018 trial as the foundational safety study
- Reliably raises blood NAD+ in dose-dependent manner; 250–1,000 mg/day produces measurable elevation
- No flushing
- Stable, FDA NDI-notified — ChromaDex's Niagen has NDI status, GRAS status for food use, and a long regulatory and safety record
- Well-characterized pharmacokinetics — peak plasma at 1–2 hours after oral dosing
Drawbacks
- More expensive per mg than niacinamide
- Requires two enzymatic steps to NAD+ (NRK phosphorylation then NMNAT adenylylation), so it is technically more "upstream" than NMN
- Like NMN, contributes to methylation cofactor depletion at chronic high doses through nicotinamide methylation by NNMT
For most clinical applications, NR is the conservative, evidence-based choice for NAD+ supplementation. The human evidence base is larger and longer than NMN's.
Nicotinamide Mononucleotide (NMN)
NMN is NR plus a phosphate — the immediate precursor of NAD+ in the salvage pathway. NMN became commercially prominent around 2013–2015, driven largely by David Sinclair's research and public advocacy. The Sinclair lab's mouse experiments showing dramatic phenotypic reversal of aging features with NMN supplementation created enormous consumer interest.
Advantages
- One step from NAD+ in the salvage pathway, so theoretically the most direct precursor
- Slc12a8 NMN transporter in the small intestine allows for direct NMN absorption without prior dephosphorylation to NR
- Raises blood NAD+ reliably; 250–1,000 mg/day produces measurable elevation comparable to NR
- No flushing
- Sinclair lab's mouse data shows impressive phenotypic reversal of aging in multiple organ systems
- Now lawful as US dietary supplement following the September 2025 FDA reversal
Drawbacks
- Smaller human evidence base than NR — the rigorous human trials are fewer in number and shorter in duration
- Brenner critique on bioavailability — the argument is that NMN must be dephosphorylated extracellularly to NR before cellular uptake, in which case oral NMN and oral NR end up doing the same thing biochemically, with NR being more efficient per mg
- Generally more expensive than NR per mg
- Quality variation in the supplement market is a real concern — analytical surveys have found commercial NMN products with less NMN than labeled
- Like NR, contributes to methylation cofactor depletion at chronic high doses
- FDA regulatory history was turbulent through 2022–2025 (see below)
Side-by-Side Comparison Table
| Property | Niacin (NA) | Niacinamide (NAM) | NR (Niagen) | NMN |
|---|---|---|---|---|
| Steps to NAD+ | 3 (Preiss-Handler) | 2 (salvage) | 2 | 1 |
| Typical dose for NAD+ raising | 500–1,500 mg/day | 500–1,500 mg/day | 300–1,000 mg/day | 250–1,000 mg/day |
| Vasodilator flush | Yes (significant) | No | No | No |
| Effect on lipids | Lowers LDL/TG; raises HDL | Minimal | Minimal | Minimal |
| Methylation cost | Low (NA does not pass through NAM in the same way) | Moderate | Moderate-high | Moderate-high |
| Human RCT evidence | Extensive (lipid trials; less on NAD+ outcomes) | Moderate (skin cancer; deficiency) | Extensive (30+ trials) | Growing (10+ trials) |
| Cost per month (typical dose) | $5–15 | $5–15 | $30–70 | $30–90 |
| FDA status (US) | Dietary supplement & OTC drug | Dietary supplement | Dietary supplement (NDI notified) | Dietary supplement (reinstated Sept 2025) |
| Best for | Lipid optimization, Lp(a) lowering | Skin cancer prevention; pellagra | Evidence-based NAD+ raising; cardiovascular support | NAD+ raising with Sinclair-aligned framework; metabolic support |
The Niacin Flush — Why It Happens and Why NR/NMN Are Flush-Free
The flush is mediated by a specific receptor: GPR109A (also called HM74A or HCAR2), a G-protein coupled receptor expressed on dermal Langerhans cells, adipocytes, immune cells, and some neurons. Niacin (nicotinic acid) is the GPR109A agonist. When niacin binds the receptor on dermal Langerhans cells, phospholipase A2 is activated, arachidonic acid is released, and cyclooxygenase-1 produces prostaglandin D2 (PGD2). PGD2 then activates DP1 and DP2 receptors on cutaneous vasculature, producing the characteristic vasodilation, warmth, redness, and pruritus.
Two important consequences flow from this mechanism:
- NR and NMN do not activate GPR109A because GPR109A is specific to the nicotinic acid (carboxylic acid) form. Nicotinamide and its derivatives (NAM, NR, NMN) have the amide instead of the carboxylic acid and do not bind GPR109A. Hence they do not flush.
- Aspirin pretreatment blocks the niacin flush because COX-1 inhibition prevents PGD2 production. 325 mg aspirin 30 minutes before niacin substantially reduces flush intensity. Tolerance also develops with chronic dosing.
For patients who specifically want niacin's lipid effects but cannot tolerate flushing, options include: (1) starting at low dose (100–250 mg) and titrating up, (2) aspirin pretreatment, (3) extended-release formulations (which spread the flush over time, though they carry higher hepatotoxicity risk), or (4) the no-flush form (inositol hexaniacinate — but the no-flush form may also be less effective for NAD+ raising, with mixed data).
For patients who want NAD+ raising without the flush, NR or NMN is the answer.
The Methylation Cofactor Debate (Brenner Critique)
Charles Brenner has been the most prominent voice raising the concern that chronic high-dose NMN or NR supplementation depletes the body's methyl donor pool. The mechanism:
- NAD+-consuming enzymes (sirtuins, PARPs, CD38) release nicotinamide (NAM) as a byproduct of their reactions
- NAM accumulates and feedback-inhibits sirtuins
- To prevent this feedback inhibition, the body methylates NAM (via N-methyltransferase, NNMT) to N1-methylnicotinamide (1-MNA), which is then excreted
- Each NAM methylation consumes one methyl group from S-adenosylmethionine (SAM)
- SAM is the universal methyl donor for hundreds of methylation reactions including DNA methylation, neurotransmitter synthesis, phospholipid synthesis, creatine synthesis, and homocysteine remethylation
- High-dose chronic NMN or NR supplementation increases the methylation demand, potentially depleting SAM
- SAM depletion can elevate homocysteine, alter DNA methylation patterns, and affect neurotransmitter synthesis
The clinical evidence for actual methyl-donor depletion in NMN/NR users is mixed:
- Some studies have measured small but statistically detectable increases in plasma homocysteine on chronic NR/NMN
- Other studies have shown no change or even decreased homocysteine
- The magnitude of the effect, if real, is small and easily mitigated by methyl donor co-supplementation
The practical recommendation that has emerged: when taking NMN or NR chronically at doses ≥500 mg/day, co-supplement with TMG (trimethylglycine, also called betaine) at 500–1,000 mg/day. TMG donates methyl groups to homocysteine to remethylate it back to methionine, which is then converted to SAM. This sidesteps the depletion concern almost entirely.
Periodic monitoring of homocysteine (target <9 µmol/L, ideally <7 µmol/L) is reasonable for anyone on chronic high-dose NMN/NR.
The Sinclair NMN Advocacy
David Sinclair's public advocacy for NMN over NR has been one of the most consequential factors in the consumer NAD+ market. Sinclair has been outspoken about taking 1 g NMN daily himself, along with resveratrol, metformin, statin, and vitamin D, in his personal longevity protocol. He has consistently framed NMN as the more "direct" precursor.
The case for NMN over NR (Sinclair-aligned):
- NMN is one step closer to NAD+ in the salvage pathway than NR
- The Slc12a8 transporter allows direct NMN uptake at the intestine
- Sinclair lab's extensive mouse data are NMN-centric and show dramatic effects
- NMN raised muscle insulin sensitivity in prediabetic women (Yoshino Science 2021)
The case for NR over NMN (Brenner-aligned):
- Larger and longer human evidence base for NR specifically
- Argument that NMN must be dephosphorylated to NR before cellular uptake (making them equivalent)
- NR is cheaper per mg
- NR has more established regulatory history (continuously on the US market since 2013)
The honest scientific assessment: both raise blood NAD+ reliably, both appear safe at the doses studied, and the absolute superiority of one over the other is not established. Personal financial interests on both sides (Sinclair's Metro International Biotech for pharmaceutical NMN; Brenner's ChromaDex for NR) should be acknowledged but should not override the published clinical data. For most users, the choice between NR and NMN is a coin flip biochemically — pick the one that fits your budget, regulatory comfort, and ideological alignment.
For the broader Sinclair lab program, see Longevity & Sirtuins.
The FDA NMN Reclassification (2022) and Reversal (2025)
The NMN regulatory history in the US has been unusually turbulent for a dietary supplement:
Timeline
- 2013–2022 — NMN sold as a dietary supplement in the US without major regulatory challenge
- October 2021 — FDA accepted an Investigational New Drug (IND) application for Metro International Biotech's pharmaceutical-grade NMN (MIB-626), authorizing it for investigation as a new drug
- November 2022 — FDA announced that NMN could not be sold as a dietary supplement ingredient. The rationale: under the FFDCA, a substance authorized for investigation as a new drug cannot be sold as a dietary supplement unless it was marketed as such before the drug investigation began. The Agency's initial reading was that NMN did not meet this exception.
- 2022–2025 — the Natural Products Association (NPA) and other industry groups filed legal challenges and lobbied for reversal, arguing that NMN was in fact marketed as a dietary supplement in the US before the MIB-626 IND was authorized
- September 29, 2025 — FDA reversed its 2022 position, confirming that beta-nicotinamide mononucleotide (NMN) is lawful for use in dietary supplements. The Agency's new analysis concluded that NMN was marketed as a dietary supplement in the US before drug investigation authorization, qualifying it for the "race to market" exception.
- December 2025 — FDA issued additional clarifying letters to NMN ingredient manufacturers (SyncoZymes, Inner Mongolia Kingdomway) confirming that NMN is no longer excluded from the dietary supplement definition.
Current status as of 2026
- NMN is lawful as a US dietary supplement
- It remains classified as a New Dietary Ingredient (NDI), so manufacturers must file an NDIN unless their supplier has already done so
- Pharmaceutical-grade NMN (Metro International's MIB-626) remains in clinical development as a pharmaceutical product, but this does not preclude dietary supplement sale of standard NMN
- Internationally: Japan and South Korea have established consumer markets; China has approved NMN as a cosmetic ingredient; the EU has not yet established a specific NMN framework
The practical implication for consumers: NMN can be purchased without legal concern in the US as of 2026. Quality varies substantially across brands; purchase from manufacturers that publish third-party certificates of analysis for both purity and potency.
Cost-Effectiveness
If the primary goal is raising blood NAD+ at the lowest cost, the precursors rank approximately:
- Niacin (NA) — cheapest, $5–15/month, but flushing limits practicality
- Niacinamide (NAM) — nearly as cheap, $5–15/month, but the 2026 head-to-head data suggest less efficient NAD+ raising than NR or NMN
- NR — $30–70/month, reliable NAD+ raising, strong evidence base
- NMN — $30–90/month, reliable NAD+ raising, growing evidence base
For cost-sensitive patients who want NAD+ raising and can tolerate niacin's flush, niacin is a reasonable choice and adds cardiovascular lipid benefits. For most patients who want NAD+ raising without flushing, NR is the most evidence-based choice. For patients who specifically buy into the Sinclair-aligned framework or want the "most direct" precursor, NMN is the choice.
Combination strategies are also reasonable: 500 mg NR or NMN once daily with intermittent niacin (250–500 mg) one or two days per week for the lipid effects.
A Practical Decision Framework
For the patient or practitioner trying to choose between the four precursors, the decision points are:
Primary goal
- Lipid optimization (high LDL, low HDL, high Lp(a)) → niacin
- Pellagra or niacin deficiency → niacin or niacinamide
- Skin cancer prevention in high-risk patients → niacinamide (per ONTRAC)
- NAD+ raising for healthspan/longevity → NR or NMN
- Cognitive support → NMN (preferred for BBB-crossing rationale)
- Cardiovascular healthspan → NR (preferred for stronger trial evidence)
- Athletic performance / exercise capacity → NMN 600–1,200 mg/day per Liao 2021
- Insulin sensitivity in prediabetic women → NMN per Yoshino 2021
Tolerance considerations
- Will flush? Avoid niacin; use NR/NMN
- On insulin or sulfonylureas? Monitor glucose closely with any precursor that improves insulin sensitivity (NR/NMN have this effect)
- Active or history of liver disease? Avoid high-dose niacin; NR/NMN are safer
- Gout? Avoid niacin (raises uric acid)
- On statin? Niacin combination has not improved cardiovascular outcomes in trials (AIM-HIGH, HPS2-THRIVE); NR/NMN are not contraindicated with statins
Budget considerations
- Tight budget → niacin (with aspirin pretreatment for flush) or niacinamide
- Moderate budget → NR
- Comfortable budget → NMN if Sinclair-aligned, or NR for the evidence base
Almost always add
- TMG 500–1,000 mg/day for any chronic high-dose NR or NMN regimen, to offset methylation cost
- Periodic homocysteine monitoring
Cautions
- Niacin and hepatotoxicity — sustained-release formulations and doses >3 g/day carry real liver toxicity risk. Get baseline and periodic LFTs.
- Niacin and diabetes — can raise blood glucose by 5–15 mg/dL; may require diabetes medication adjustment.
- Niacin and gout — can precipitate gout attacks by raising uric acid; avoid in gout-prone patients.
- Niacinamide at >3 g/day — potential hepatotoxicity; theoretical sirtuin inhibition; avoid chronic high-dose use.
- NR/NMN and methylation — co-supplement TMG at chronic doses ≥500 mg/day.
- NMN supplement quality — analytical surveys have found commercial NMN products with less NMN than labeled. Purchase from third-party-tested brands.
- NR/NMN and insulin sensitivity — can lower blood glucose; monitor closely in insulin-treated or sulfonylurea-treated diabetics.
- Theoretical cancer concern — see Longevity & Sirtuins.
- Pregnancy/breastfeeding — standard B3 RDA (14–18 mg) is safe and required; high-dose NR/NMN have no safety data in pregnancy; avoid.
- Long-term safety — multi-year effects of any of these precursors at supraphysiologic doses are not yet characterized in humans.
Key Research Papers
- Bieganowski, P., Brenner, C. (2004). Discoveries of Nicotinamide Riboside as a Nutrient and Conserved NRK Genes Establish a Preiss-Handler Independent Route to NAD+ in Fungi and Humans. Cell 117(4), 495–502. — PubMed
- Martens, C.R., et al. (2018). Chronic Nicotinamide Riboside Supplementation Is Well-Tolerated and Elevates NAD+ in Healthy Middle-Aged and Older Adults. Nature Communications 9(1), 1286. — DOI
- Grozio, A., et al. (2019). Slc12a8 Is a Nicotinamide Mononucleotide Transporter. Nature Metabolism 1(1), 47–57. — PubMed
- Yoshino, J., Baur, J.A., Imai, S. (2018). NAD+ Intermediates: The Biology and Therapeutic Potential of NMN and NR. Cell Metabolism 27(3), 513–528. — DOI
- Yoshino, M., et al. (2021). Nicotinamide Mononucleotide Increases Muscle Insulin Sensitivity in Prediabetic Women. Science 372(6547), 1224–1229. — DOI
- Pencina, K.M., et al. (2023). MIB-626, an Oral Formulation of a Microcrystalline Unique Polymorph of Beta-Nicotinamide Mononucleotide, Increases Circulating NMN and NAD in a Randomized Clinical Trial. Journals of Gerontology: Series A 78(1), 90–96. — DOI
- Trammell, S.A., et al. (2016). Nicotinamide Riboside Is Uniquely and Orally Bioavailable in Mice and Humans. Nature Communications 7, 12948. — PubMed
- Chen, A.C., et al. (2015). A Phase 3 Randomized Trial of Nicotinamide for Skin-Cancer Chemoprevention (ONTRAC). New England Journal of Medicine 373(17), 1618–1626. — PubMed
- AIM-HIGH Investigators (2011). Niacin in Patients with Low HDL Cholesterol Levels Receiving Intensive Statin Therapy. New England Journal of Medicine 365(24), 2255–2267. — PubMed
- HPS2-THRIVE Collaborative Group (2014). Effects of Extended-Release Niacin with Laropiprant in High-Risk Patients. New England Journal of Medicine 371(3), 203–212. — PubMed
- Hwang, E.S., Song, S.B. (2017). Nicotinamide Is an Inhibitor of SIRT1 in Vitro, But Can Be a Stimulator in Cells. Cellular and Molecular Life Sciences. — PubMed
- Yang, Y., et al. (2025). An Updated Review on the Mechanisms, Pre-Clinical and Clinical Comparisons of NMN and NR. Food Frontiers 6(1), e511. — PubMed
- US FDA (2025). Letters Confirming NMN Is Lawful for Use in Dietary Supplements (SyncoZymes, Inner Mongolia Kingdomway).
PubMed Topic Searches
- PubMed: NMN vs NR head-to-head
- PubMed: niacin flush mechanism
- PubMed: NMN bioavailability/Slc12a8
- PubMed: NR clinical trials
- PubMed: NMN FDA regulatory
- PubMed: TMG/betaine methylation
Connections
- NAD+ & NMN Overview
- NAD+ Benefits Hub
- NAD+ for Longevity & Sirtuins
- NAD+ for Cognition
- NAD+ for Energy & Mitochondria
- Vitamin B3 (Niacin)
- Niacin & Cholesterol
- Pellagra & Niacin Deficiency
- All Antioxidants
- CoQ10
- NAC
- Glutathione
- Alpha Lipoic Acid
- Methylene Blue
- Longevity Protocols
- Cholesterol Management
- Cardiovascular Disease
- Insulin Resistance