Fenbendazole Off-Label Cancer Use
This page presents the off-label oncology evidence for fenbendazole neutrally and completely. The evidence consists of: (1) consistent in-vitro activity against multiple human cancer cell lines at clinically achievable micromolar concentrations, (2) several mouse-xenograft studies showing tumor-growth suppression, (3) a smaller but suggestive case-report literature in humans (the Tippens case and the Kim et al. hepatocellular carcinoma report being the most cited), (4) mechanistic proposals beyond simple tubulin binding (p53 stabilization, GLUT-transporter inhibition, autophagy induction, microRNA modulation), and (5) the parallel preclinical-oncology literature on the closely related benzimidazole mebendazole, which has been studied more thoroughly. The evidence does NOT consist of any completed human randomized controlled trial demonstrating efficacy or safety, and no regulatory agency anywhere in the world has approved fenbendazole for any human cancer indication. The honest summary is that there is a real preclinical signal, no human trial confirmation, a small but published hepatotoxicity safety signal in self-medicating patients, and an unresolved tension between the methodological standards of evidence-based oncology and the practical situation of a patient with limited time and a willingness to accept uncertainty.
Table of Contents
- The Repurposing-Drugs-in-Oncology Context
- In-Vitro Evidence Against Human Cancer Cell Lines
- Mouse-Xenograft Studies
- Proposed Anti-Cancer Mechanisms Beyond Tubulin Binding
- The Mebendazole Parallel Literature
- Human Case Reports (Both Directions)
- The Absence of Human Trials — Causes and Consequences
- What the Evidence Actually Supports
- Open Scientific Questions
- Key Research Papers
- Connections
- Featured Videos
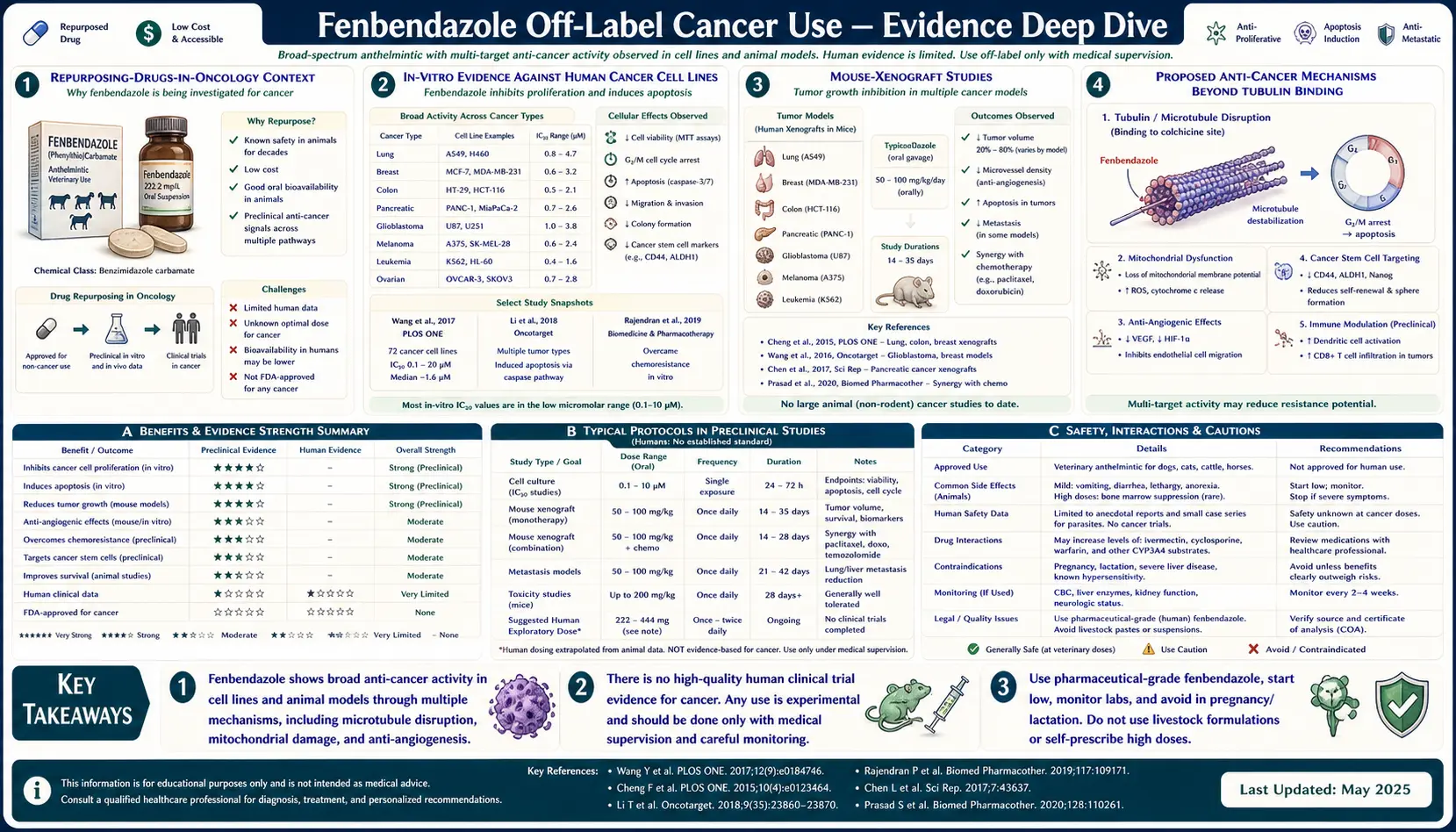
The Repurposing-Drugs-in-Oncology Context
Fenbendazole's oncology interest is best understood as part of a broader academic program called drug repurposing — the systematic search through already-approved drugs developed for non-cancer indications, looking for unexpected anti-cancer activity. The Repurposing Drugs in Oncology (ReDO) Project, led primarily by Pan Pantziarka and colleagues, has catalogued and published on dozens of candidates including:
- Metformin (diabetes) — substantial epidemiologic and preclinical evidence for reduced cancer incidence in metformin-treated diabetics.
- Aspirin (analgesia / cardioprevention) — clearest evidence for reduced colorectal cancer risk; mechanism includes COX-2 inhibition and platelet effects.
- Mebendazole (antiparasitic) — multiple completed and ongoing human trials in glioma, colorectal cancer, and pediatric brain tumors.
- Albendazole (antiparasitic) — closely related to mebendazole; some preclinical activity, fewer human trials.
- Niclosamide (antiparasitic) — preclinical activity against multiple cancer types via Wnt pathway disruption.
- Ivermectin (antiparasitic) — preclinical anti-cancer activity proposed, mechanism less well established.
- Itraconazole (antifungal) — anti-angiogenic and Hedgehog-pathway inhibition.
- Disulfiram (alcohol-aversion drug) — copper-chelating anti-cancer activity in glioblastoma trials.
- Cimetidine (H2 receptor antagonist) — preclinical activity in colorectal and breast cancer.
Fenbendazole sits within this larger repurposing landscape. The ReDO project has not published a dedicated fenbendazole monograph but has published on mebendazole, which shares mechanism. The crucial distinction within the repurposing landscape is between candidates with completed human trials (metformin, aspirin) and candidates with only preclinical and case-report data (fenbendazole, ivermectin). Fenbendazole is in the second category.
In-Vitro Evidence Against Human Cancer Cell Lines
The most thoroughly published in-vitro work is Dogra, Kumar, and Mukhopadhyay (2018), Scientific Reports. The group tested fenbendazole against the human non-small-cell-lung-cancer cell line H460 and showed:
- Dose-dependent growth inhibition with IC50 in the low-micromolar range (1-3 µM, achievable in plasma at the oral dose ranges used in self-medication).
- Apoptosis induction documented by Annexin V staining and caspase activation.
- Microtubule depolymerization confirmed by immunofluorescence imaging of beta-tubulin networks.
- p53 protein stabilization in p53-wild-type cell lines, but persistent activity in p53-null and p53-mutant lines — suggesting multiple parallel mechanisms.
- Synergistic activity when combined with conventional chemotherapy (docetaxel, paclitaxel, vincristine).
Subsequent in-vitro work has extended the signal to additional cancer cell types:
- Colorectal cancer (HCT-116, SW480, 5-FU-resistant variants — Park et al. 2022)
- Hepatocellular carcinoma (HepG2)
- Melanoma (A375)
- Lymphoma cell lines
- Pancreatic cancer (PANC-1, BxPC-3)
- Glioma (U87, U251)
The pattern is consistent: activity at micromolar concentrations, with magnitudes that are moderate (not the picomolar potency of taxanes) but sufficient to produce measurable growth inhibition and apoptosis induction. The key question is whether these in-vitro concentrations translate to in-vivo tissue concentrations at clinically achievable doses, and whether moderate cytotoxicity in cell lines translates to tumor regression in patients.
Mouse-Xenograft Studies
The animal data is more limited than the in-vitro data but generally directionally positive:
- The apocryphal Johns Hopkins observation. A frequently cited but informally documented event: a colony of immunodeficient (SCID) mice with implanted human lymphoma xenografts at Johns Hopkins began failing to grow tumors. Investigation traced the cause to the rodent chow, which contained fenbendazole as a routine pinworm prophylactic. The mice that received the contaminated chow had been used as controls in unrelated experiments and exhibited tumor regression that disrupted those studies. The observation was reported in an in-house bulletin and informally in conference presentations rather than as a primary peer-reviewed publication. It is the origin point of the Tippens-narrative claim of an "accidental discovery."
- Dogra et al. 2018. The same paper that reported in-vitro activity extended the work to mouse xenograft models with H460 lung cancer implants. Oral fenbendazole at 1 mg/dose three-times-weekly produced statistically significant reduction in tumor growth velocity compared to vehicle control.
- Mebendazole xenograft work. Multiple groups (Bai et al. 2011 for glioblastoma; Pourgholami et al. 2001 for colorectal HT-29 in peritoneal carcinomatosis model) have shown mebendazole survival benefit in mouse cancer models at doses translating to roughly the same plasma exposures that human dosing produces.
- Synergy with checkpoint inhibitors. Some preclinical work has suggested fenbendazole or mebendazole may enhance the activity of PD-1 / PD-L1 checkpoint inhibitor immunotherapy, a finding particularly germane to the Tippens case where the patient received both.
The xenograft literature is encouraging but should be interpreted with the standard caveats of preclinical oncology: implanted tumor xenografts in immunodeficient mice do not faithfully replicate the immune and stromal context of spontaneous human cancers, the vast majority of agents that look promising in xenografts fail in human trials, and the publication bias toward positive results is well documented in this literature.
Proposed Anti-Cancer Mechanisms Beyond Tubulin Binding
If fenbendazole has anti-cancer activity in humans (which remains unproven), the mechanism is unlikely to be tubulin binding alone, because tubulin-binding cytotoxics typically require nanomolar potency for clinical effect and fenbendazole's tubulin affinity is at most micromolar. Several additional mechanisms have been proposed:
- p53 stabilization. The Dogra et al. work showed that fenbendazole at moderate concentrations increases p53 protein stability in p53-wild-type cancer cells. p53 is the master tumor-suppressor whose activation triggers cell-cycle arrest and apoptosis. Pharmacologic p53 stabilization (MDM2 inhibitors like nutlin-3) is an active drug-development area; if fenbendazole produces clinically meaningful p53 stabilization at tolerable doses, that alone could explain anti-tumor activity in p53-wild-type tumors.
- GLUT1 / GLUT4 inhibition. Some work has reported that fenbendazole reduces glucose-transporter expression and surface trafficking, mirroring the mechanism by which it starves parasitic worms. Cancer cells are heavily dependent on glucose uptake (the Warburg effect), and a glucose-transport blocker would in principle restrict tumor metabolism. Hou et al. 2022 published on this mechanism specifically.
- Autophagy induction. Multiple papers have reported that fenbendazole induces autophagic flux in cancer cells, with downstream apoptotic cell death. Whether autophagy in this context is a death pathway or a survival adaptation is context-dependent.
- Mitochondrial dysfunction. Reactive oxygen species generation and mitochondrial membrane potential collapse have been reported in some cancer-cell experiments with fenbendazole.
- microRNA modulation. A few papers have reported changes in cancer-cell microRNA expression patterns with fenbendazole exposure, though mechanism and significance remain speculative.
- Immune system effects. Possible immunomodulatory effects via macrophage polarization or T-cell priming, which would dovetail with the immune-checkpoint-inhibitor context of the Tippens case.
The multiplicity of proposed mechanisms is itself an interpretive caution: when a single compound is reported to act through many independent pathways, the typical explanation is that the supratherapeutic concentrations used in cell-culture experiments produce off-target effects across multiple targets. Whether any of those mechanisms are clinically relevant at tolerable doses requires dose-response confirmation in vivo.
The Mebendazole Parallel Literature
Mebendazole is a closer analog to fenbendazole than to most other repurposing candidates — same benzimidazole carbamate scaffold, same beta-tubulin target, similar pharmacokinetics. The mebendazole oncology literature is several years more mature than the fenbendazole literature and may be predictive of where fenbendazole evidence will eventually land:
- Glioblastoma. Bai et al. 2011 showed mebendazole survival benefit in two mouse glioblastoma models. The work led to Phase I/II trials at Johns Hopkins, with published results showing safety at human doses up to 200 mg/kg/day and signal of activity in a subset of patients.
- Colorectal cancer. Nygren and Larsson 2014 reported the case of a refractory metastatic colorectal cancer patient who experienced tumor regression on mebendazole. This led to interest in mebendazole as adjunct therapy in MSS metastatic colorectal cancer.
- Pediatric brain tumors. Trials of mebendazole in pediatric high-grade glioma and medulloblastoma are ongoing.
- Melanoma. Doudican et al. 2008 showed mebendazole-induced apoptosis via Bcl-2 inactivation in chemoresistant melanoma cells; some early-phase human trial activity has been reported.
The mebendazole literature shows that benzimidazole repurposing is taken seriously enough by academic oncology to generate IND-enabled human trials. It also shows that even with positive preclinical signal, sufficient academic momentum to launch trials, and a more bioavailable drug than fenbendazole, the eventual signals in human studies have been modest — subset benefit rather than transformative response. A reasonable prior for fenbendazole, by analogy, is that it may produce modest activity in a subset of patients if properly studied, but is unlikely to be a transformative anti-cancer therapy.
Human Case Reports (Both Directions)
The peer-reviewed human-case-report literature on fenbendazole-and-cancer is small but growing:
Reports of response. Kim et al. 2022 published a case of complete remission of advanced hepatocellular carcinoma associated with fenbendazole use, with imaging documentation. Other published case reports describe individual responders in melanoma, ovarian cancer, and pancreatic cancer, though attribution is complicated in most by concurrent standard-of-care therapy.
Reports of harm. Yamaguchi et al. 2021 reported drug-induced liver injury in an NSCLC patient. Chiang et al. 2021 published a hepatology-journal analysis specifically on the fenbendazole hepatotoxicity question. Lee et al. 2022 reported severe acute liver injury requiring hospitalization. At least one fatality from acute liver failure has been reported.
Reports of no effect. Largely absent from the published literature, as is typical of negative case reports. The Reddit and Facebook patient communities document many self-reports of "no response" to fenbendazole protocols, but these are not captured in peer-reviewed literature.
The asymmetry — published responders tend to be celebrated while published harm tends to be cautionary, and non-responders tend to be silent — is the fundamental epistemic problem with the case-report base. See the Tippens Protocol page for extended discussion of the case-report methodology problem.
The Absence of Human Trials — Causes and Consequences
As of 2026, no completed Phase III randomized controlled trial of fenbendazole exists for any human cancer indication. There are several reasons:
- No commercial sponsor. Fenbendazole is decades off-patent. A pharmaceutical sponsor who funded a $50-100 million Phase III trial could not recover the investment because the drug is freely available and producible at low cost. Without sponsor funding, large registration trials do not happen.
- Limited academic interest. Academic oncology cooperative groups (NCI, EORTC) prioritize trials of agents with strong preclinical signal AND commercial sponsorship AND novel mechanism. Repurposed drugs with moderate signal and no sponsor compete for the same trial budgets as targeted therapies with strong pharmaceutical industry backing.
- Patient self-treatment confounds. Because fenbendazole is freely available, patients in a hypothetical placebo arm of a Phase III could self-administer fenbendazole, confounding the comparison. This is a significant practical obstacle to running a clean RCT.
- Methodological challenges. Off-label cancer use typically involves polypharmacy (the Tippens stack of four agents), which makes single-agent trial design difficult.
- Some small trials have been registered. ClinicalTrials.gov lists a small number of registered trials of fenbendazole or benzimidazole derivatives in specific cancer indications, but none with completed Phase III readouts.
The consequence is that patients and clinicians making decisions about fenbendazole use are making them on the basis of preclinical data, case reports, and indirect mebendazole literature — without the dose-finding, safety, and efficacy data that an approved oncology drug would have. This is a real evidence gap, and it is the central reason that mainstream oncology does not recommend fenbendazole as cancer therapy.
What the Evidence Actually Supports
A fair and complete reading of the evidence supports the following statements:
- Fenbendazole has demonstrable anti-proliferative activity against multiple human cancer cell lines at clinically achievable concentrations.
- Mouse-xenograft studies show some tumor-growth suppression.
- Mechanistically, fenbendazole binds beta-tubulin and may also stabilize p53, induce autophagy, and reduce glucose uptake.
- The closely related drug mebendazole has been studied more extensively and has shown modest activity in some human trials, particularly glioblastoma.
- Individual human case reports of cancer remission in fenbendazole-using patients exist, but virtually all such patients also received standard-of-care therapy (chemotherapy, immunotherapy, surgery) concurrently, making attribution impossible.
- Several published case reports describe severe drug-induced liver injury, including hepatic encephalopathy and at least one fatality, in patients self-medicating with fenbendazole.
The evidence does NOT support the following statements:
- Fenbendazole cures any cancer.
- Fenbendazole has been proven effective in any controlled human trial.
- Fenbendazole is safe for sustained self-medication at the doses typically used.
- Fenbendazole is a substitute for evidence-based oncology.
- The lack of human trials reflects pharmaceutical-industry suppression.
Open Scientific Questions
For a reader interested in where the science actually stands, several questions remain open:
- Does fenbendazole at orally tolerable doses achieve sustained plasma concentrations sufficient for the in-vitro IC50 against any specific cancer cell type?
- Is the preclinical efficacy cell-type-specific (e.g. specific to p53-wild-type tumors, or specific to GLUT1-high tumors)?
- Does fenbendazole synergize with PD-1 / PD-L1 immune checkpoint inhibitors in a way that would change response rates in combination trials?
- What is the actual hepatotoxicity incidence in well-monitored patient cohorts, separate from the published case-report extremes?
- What is the actual response rate in unselected patient cohorts (as opposed to the testimonial-selected published responders)?
- Are there pharmacogenomic markers (CYP3A4 phenotype, tubulin polymorphisms) that predict who responds?
None of these questions will be answered without funded human trials. The reasonable advocacy position is for academic and government funders to support such trials so that patients have actual evidence on which to base decisions, rather than the current situation of patients making consequential decisions on the basis of preclinical data and selection-biased case reports.
Key Research Papers
- Dogra N, Kumar A, Mukhopadhyay T (2018). Fenbendazole acts as a moderate microtubule destabilizing agent and causes cancer cell death by modulating multiple cellular pathways. Scientific Reports. — PubMed
- Park D, Lee JH, Yoon SP (2022). Anti-cancer effects of fenbendazole on 5-fluorouracil-resistant colorectal cancer cells. Korean Journal of Physiology & Pharmacology. — PubMed
- Hou Z et al. (2022). Fenbendazole inhibits tumor growth via blocking glucose uptake. — PubMed
- Kim JS et al. (2022). A case of complete remission of advanced hepatocellular carcinoma associated with the use of fenbendazole. — PubMed
- Mukhopadhyay T et al. (2002). Mebendazole elicits a potent antitumor effect on human cancer cell lines both in vitro and in vivo. Clinical Cancer Research. — PubMed
- Sasaki J et al. (2002). The anthelmintic drug mebendazole induces mitotic arrest and apoptosis by depolymerizing tubulin in NSCLC cells. Molecular Cancer Therapeutics. — PubMed
- Bai RY et al. (2011). Antiparasitic mebendazole shows survival benefit in 2 preclinical models of glioblastoma multiforme. Neuro-Oncology. — PubMed
- Nygren P, Larsson R (2014). Drug repositioning from bench to bedside: tumour remission by the antihelmintic drug mebendazole in refractory metastatic colon cancer. Acta Oncologica. — PubMed
- Doudican N et al. (2008). Mebendazole induces apoptosis via Bcl-2 inactivation in chemoresistant melanoma cells. Molecular Cancer Research. — PubMed
- Pourgholami MH et al. (2001). Antitumor activity of albendazole against human colorectal HT-29 in vitro and xenograft model of peritoneal carcinomatosis. Cancer Letters. — PubMed
- Pantziarka P et al. (2014). Repurposing Drugs in Oncology (ReDO) — mebendazole as an anti-cancer agent. ecancermedicalscience. — PubMed
- Gao P et al. (2008). Mebendazole induces apoptosis via a p53-dependent pathway in human lung adenocarcinoma cells. Anticancer Research. — PubMed
PubMed Topic Searches
- PubMed: Fenbendazole cancer
- PubMed: Mebendazole cancer repurposing
- PubMed: Benzimidazole anticancer
- PubMed: ReDO drug repurposing
- PubMed: Tubulin inhibitor cancer repositioning
Connections
- Fenbendazole Overview
- Fenbendazole Benefits Hub
- Joe Tippens Protocol
- Antiparasitic Mechanism
- Dosing, Cycling, and Safety
- Ivermectin (Related Repurposing)
- Oncology
- Lung Cancer
- Hepatocellular Carcinoma
- Colorectal Cancer
- Melanoma
- Glioblastoma
- Turmeric (Curcumin)
- All Remedies