Fenbendazole Dosing, Cycling, and Safety
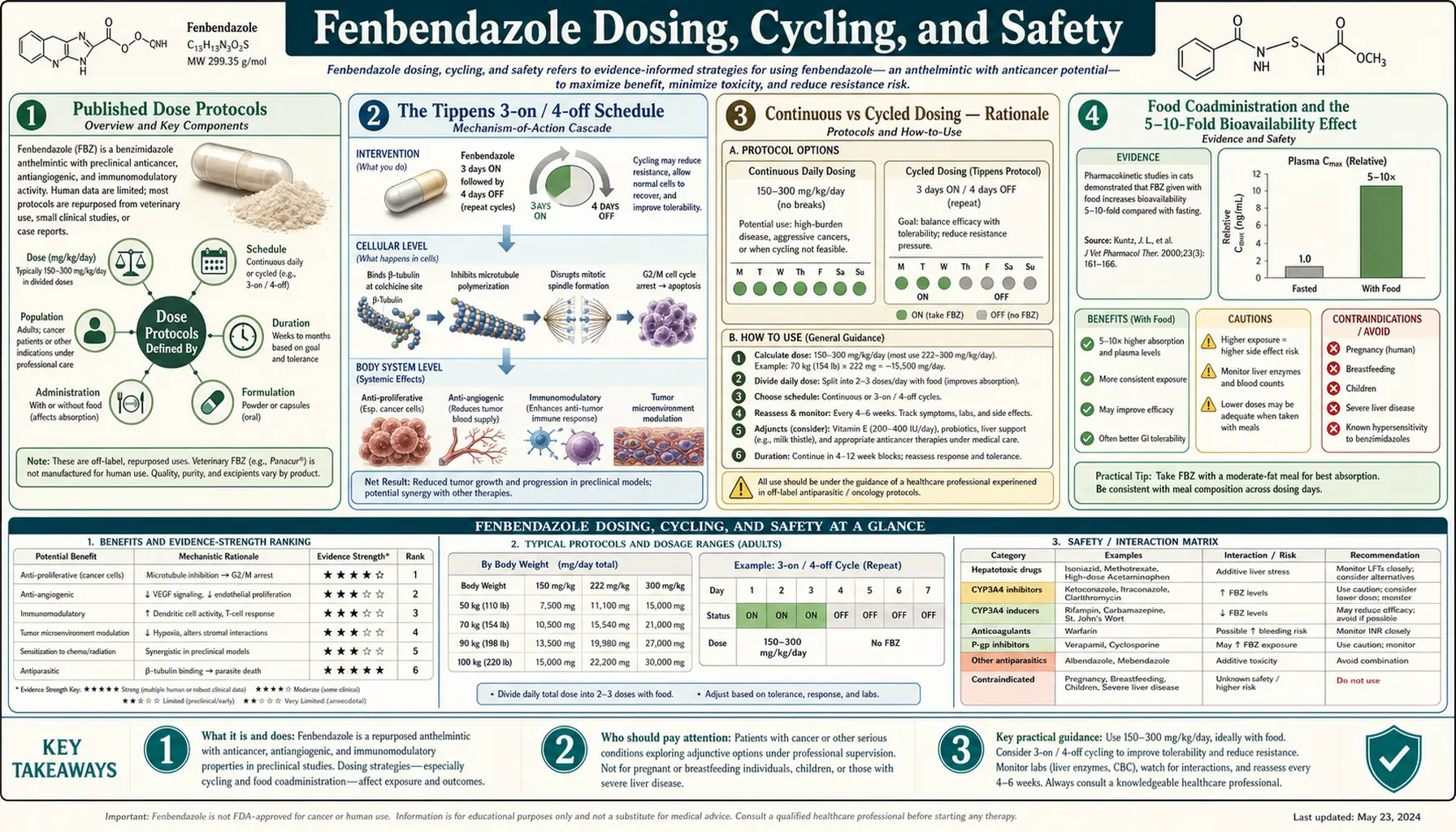
Practical dosing information for a drug used off-label is genuinely useful only when paired with honest safety information. The Tippens-style protocol calls for 222 mg/day of fenbendazole on a 3-days-on / 4-days-off cycle, taken with a fatty meal; alternative protocols use continuous daily dosing or higher pulse doses. The veterinary dose-tolerance literature supports these ranges as well below acute toxic levels in animals, but does not address the question of sustained months-to-years exposure in humans — which is what the cancer-protocol population is actually doing. The accumulating human case-report literature documents several patterns of fenbendazole-associated hepatotoxicity: cholestatic injury, hepatocellular injury with transaminase elevation, and in a small number of published cases, acute liver failure requiring intensive care or transplantation, including at least one published fatality. This page covers the actual published dose schedules, the food-effect on bioavailability, the drug interactions (especially CYP3A4-relevant), the documented hepatotoxicity reports with monitoring guidance, and what informed consent for a self-medicating patient should look like.
Table of Contents
- Published Dose Protocols
- The Tippens 3-on / 4-off Schedule
- Continuous vs Cycled Dosing — Rationale
- Food Coadministration and the 5-10-Fold Bioavailability Effect
- The Hepatotoxicity Signal
- Laboratory Monitoring
- Drug Interactions
- Veterinary vs Human-Grade Product Quality
- Absolute and Relative Contraindications
- What Informed Consent Looks Like
- Key Research Papers
- Connections
- Featured Videos
Published Dose Protocols
Several distinct dose protocols have circulated in the off-label oncology user community. None is FDA-approved. None is supported by Phase II / III human dose-finding data. The summary below is descriptive of what is actually used, not a recommendation.
- The Tippens Protocol — 222 mg/day fenbendazole (one gram of 22.2% Panacur-C canine granules) for 3 consecutive days, followed by 4 days off, taken with a fatty meal. Plus 800 IU/day vitamin E succinate, 600 mg/day curcumin, and 25 mg/day CBD oil, taken daily without cycling.
- Modified Tippens (continuous) — some practitioners and patients use 222 mg/day continuously without the 4-day washout, on the theory that intermittent dosing allows tumor regrowth.
- Higher-dose protocols — some users escalate to 444 mg/day (two grams of canine granules) or 1000 mg/day (single human-veterinary cross-equivalent doses), with varying schedules. The accumulating hepatotoxicity case reports skew toward this higher-dose population.
- Pulse dosing — a less common variant uses very high single doses (e.g., 2000 mg) weekly rather than smaller daily doses.
- Combination with mebendazole — some patients use both fenbendazole (veterinary, freely available) and mebendazole (human-approved, requires prescription in most countries) concurrently. There is no pharmacologic rationale for the combination over either alone.
The choice of schedule among these options is essentially arbitrary in the absence of dose-finding trials. The Tippens schedule has the inertia of being the original published narrative; the continuous schedule has the appeal of being conceptually simpler; the higher-dose schedule has the appeal (and the corresponding risk) of producing higher systemic exposures.
The Tippens 3-on / 4-off Schedule
Tippens has explained in interviews that he chose the 3-days-on / 4-days-off schedule partly because that was the dosing his veterinarian friend used for canine deworming, and partly out of a general intuition that intermittent dosing might be less hepatotoxic than continuous dosing. There is no peer-reviewed pharmacology behind the specific schedule.
The pharmacokinetic implication: with a 10-15 hour elimination half-life, fenbendazole plasma concentrations decline to near-baseline within 2-3 days of stopping dosing. The 4-day washout therefore produces a "trough" period of essentially no drug exposure between dosing pulses. Whether this trough is biologically beneficial (allowing recovery of any sensitive host tissue) or harmful (allowing tumor regrowth between pulses) is unknown.
The veterinary parasitology literature does not directly inform this question because veterinary dosing is typically single-dose or 3-day-course for parasite eradication, not the sustained months-to-years dosing the cancer-protocol population uses.
Continuous vs Cycled Dosing — Rationale
Proponents of continuous daily dosing cite:
- Standard chemotherapy practice generally uses sustained exposure, with dose-limiting toxicity managed by dose reduction rather than by treatment interruption.
- The in-vitro cancer-cell data show concentration-time-area-under-curve dependence, not pulse-trough dependence.
- Patient self-reports of more sustained response with continuous dosing (highly subject to selection bias).
Proponents of cycled dosing cite:
- The Tippens precedent.
- Theoretical concern about cumulative hepatotoxicity with sustained exposure.
- Practical compliance (it is easier to remember a 3-on / 4-off schedule with weekend washout than to take pills every day).
The honest answer is that there is no human dose-finding trial to settle the question. A patient and clinician choosing between schedules is making the choice on the basis of theory and individual judgment, not data.
Food Coadministration and the 5-10-Fold Bioavailability Effect
Fenbendazole oral bioavailability is one of the most fat-dependent of any commonly used drug. Taking 222 mg with a high-fat meal (e.g., breakfast with eggs, bacon, avocado, or full-fat dairy) produces several times the systemic plasma concentration of the same dose taken fasting. The mechanism is the standard one for highly lipophilic drugs: dietary fat triggers bile salt secretion, which solubilizes the drug into mixed micelles for small-intestinal absorption.
The practical implications:
- Patients who take fenbendazole at bedtime on an empty stomach are absorbing approximately one-fifth to one-tenth of what a with-fatty-meal protocol delivers. They may be effectively taking a much smaller dose than the label suggests.
- Variation in meal composition produces variation in dose, which complicates interpretation of dose-response across patients.
- Adding a tablespoon of MCT oil or olive oil with each dose is sometimes recommended to standardize the fat coadministration.
- The Tippens published protocol explicitly recommends with-food dosing; some derivative protocols omit this detail.
The Hepatotoxicity Signal
The published case-report literature on fenbendazole-associated hepatotoxicity has grown substantially in the years since the Tippens propagation began. Reported patterns include:
- Cholestatic injury — elevated alkaline phosphatase and gamma-glutamyl transferase out of proportion to transaminases, with itching, jaundice, and pale stools.
- Hepatocellular injury — transaminase elevation (ALT and AST), with the AST/ALT ratio variable.
- Mixed pattern — combined cholestatic and hepatocellular features.
- Acute liver failure — coagulopathy, encephalopathy, and progressive bilirubin rise. Reported in case reports including at least one fatality in a Korean lung-cancer patient (Hou et al. 2022 description; multiple Korean and Japanese case reports).
Risk factors that appear repeatedly in the published cases:
- Higher daily doses (>500 mg/day cumulative).
- Longer duration of use (months rather than weeks).
- Pre-existing liver disease, including hepatocellular-carcinoma patients with underlying cirrhosis.
- Concurrent hepatotoxic chemotherapy.
- Use of high-fat coadministration that effectively boosts absorbed dose.
- Concurrent alcohol use.
The veterinary literature does not predict this hepatotoxicity because veterinary dosing is short-course (typically 3-5 days) and the relevant species rarely undergo the sustained months-to-years exposure that human cancer protocols entail. The hepatotoxicity is therefore a human-specific signal that has emerged only as the self-medicating patient population has grown large enough to surface case reports.
Laboratory Monitoring
Any patient choosing to self-medicate with fenbendazole should have, at minimum:
- Baseline liver panel before starting: ALT, AST, alkaline phosphatase, gamma-glutamyl transferase, total and direct bilirubin, total protein, albumin, INR. Document any pre-existing abnormality.
- Hepatitis serology at baseline if not previously documented: hepatitis B surface antigen, hepatitis B core antibody, hepatitis C antibody.
- CBC at baseline to document baseline cell counts.
- Repeat liver panel at 2 weeks, 4 weeks, then every 4-6 weeks thereafter, more frequently if abnormalities appear.
- Discontinuation thresholds — any ALT or AST rise to greater than 3-fold upper limit of normal, any bilirubin rise above 1.5-fold upper limit of normal, any new jaundice, any coagulopathy (INR >1.5 not explained by warfarin or hepatic synthetic dysfunction from underlying disease), any encephalopathy. These thresholds are conservative because the cost of missing early hepatotoxicity is potentially fatal.
- Coordination with oncologist — share monitoring labs with the treating oncologist, who may have additional concerns specific to the concurrent cancer therapy and may modify the chemotherapy / immunotherapy schedule based on liver function trends.
See our Liver Function Tests page for interpretation context.
Drug Interactions
Fenbendazole is metabolized predominantly by hepatic CYP3A4, with secondary contributions from CYP1A2 and flavin-containing monooxygenase. This creates several categories of clinically relevant interactions:
- CYP3A4 inhibitors raise fenbendazole levels and increase hepatotoxicity risk. Notable inhibitors: ketoconazole, itraconazole, voriconazole, clarithromycin, erythromycin, ritonavir and other protease inhibitors, grapefruit juice (significant and sustained inhibition), Seville orange juice, certain calcium channel blockers (diltiazem, verapamil).
- CYP3A4 inducers reduce fenbendazole levels and may attenuate any anti-cancer activity. Notable inducers: rifampin, rifabutin, carbamazepine, phenytoin, phenobarbital, St. John's Wort, efavirenz, modafinil.
- Concurrent chemotherapy — many oncology drugs are themselves CYP3A4 substrates, inhibitors, or inducers. Concurrent fenbendazole can perturb chemotherapy plasma levels in either direction, with consequences for both efficacy and toxicity. This is a critical reason to coordinate with the treating oncologist rather than hiding off-label use.
- Concurrent immunotherapy — PD-1, PD-L1, and CTLA-4 inhibitors are monoclonal antibodies metabolized by reticuloendothelial proteolysis rather than CYP enzymes, so direct pharmacokinetic interaction with fenbendazole is unlikely. Pharmacodynamic interaction (immune activation or suppression) is less well characterized but theoretically possible.
- Warfarin and other anticoagulants — fenbendazole binds plasma proteins extensively and can displace warfarin from albumin binding sites, with potential INR rise. Monitor INR closely if both are used.
- Statins — both atorvastatin and simvastatin are CYP3A4 substrates; concurrent use with fenbendazole increases statin levels and rhabdomyolysis risk.
- Acetaminophen — while not a direct pharmacokinetic interaction, the additive hepatotoxicity risk of acetaminophen plus any hepatotoxic agent suggests minimizing acetaminophen use during fenbendazole exposure.
- Alcohol — additive hepatotoxicity; significantly increases the risk of fenbendazole-associated liver injury. Patients using fenbendazole should minimize or eliminate alcohol.
Veterinary vs Human-Grade Product Quality
The fenbendazole available without prescription at farm-supply retailers is manufactured to veterinary regulatory standards, not USP human-pharmaceutical standards. The relevant differences:
- Identity and potency. Veterinary products are tested for active drug content, typically meeting label claim within reasonable tolerances. They are not, however, subject to the human-pharmaceutical USP standards for content uniformity dose-to-dose.
- Impurities. Veterinary products are tested for the impurities relevant to the labeled species but may not be tested for impurities relevant to human exposure. The flavor and excipient composition is optimized for animal palatability rather than human bioavailability.
- Sterility. Granular products are not sterile and are not labeled for human consumption.
- Compounded human-grade fenbendazole. Specialty compounding pharmacies in some jurisdictions produce human-formulated fenbendazole capsules with pharmaceutical-grade active ingredient and a certificate of analysis. These are technically off-label and not FDA-approved as products, but they meet a higher manufacturing standard than veterinary granules.
- Online suppliers. A substantial part of the off-label market is supplied by online vendors of variable provenance and quality control. Product testing by independent labs has occasionally found significant content discrepancies.
A patient who is going to use fenbendazole at all is better off using either compounded human-grade product or a single trusted-source veterinary product, and ideally testing the product if any independent laboratory testing is feasible.
Absolute and Relative Contraindications
- Pregnancy and lactation — absolute contraindication. Benzimidazoles are teratogenic in animal studies at high doses. Fenbendazole should not be used during pregnancy or while breastfeeding.
- Pre-existing liver disease — relative contraindication. Patients with cirrhosis, active hepatitis B or C, autoimmune hepatitis, primary biliary cholangitis, or any underlying chronic liver disease are at substantially elevated risk for fenbendazole-induced hepatotoxicity.
- Pediatric patients — pediatric off-label use should occur only under specific pediatric oncology supervision, never as parental self-administration.
- Acute liver injury of any cause — if liver enzymes rise during fenbendazole use, discontinue immediately and do not rechallenge.
- Severe renal impairment — metabolite accumulation may occur; data are limited.
- Concurrent hepatotoxic medications — methotrexate, isoniazid, amiodarone, valproate, prolonged acetaminophen at the upper end of recommended daily intake, and others. The cumulative hepatotoxic risk is more than additive.
- Active alcohol use disorder — substantially elevates hepatotoxicity risk.
What Informed Consent Looks Like
A patient who is going to use fenbendazole off-label for cancer should be able to honestly affirm the following, after reading and considering each point:
- I understand that fenbendazole is not FDA-approved for any human indication, and that no randomized controlled trial has demonstrated that it is safe or effective as a cancer treatment in humans.
- I understand that I am not entering a clinical trial and that there is no protocol-mandated safety monitoring or data collection for off-label use.
- I understand that published case reports have described severe drug-induced liver injury, including acute liver failure requiring intensive care and at least one published fatality, in patients using fenbendazole off-label.
- I have informed my oncologist of my decision to use fenbendazole.
- I have established baseline liver enzymes and have a plan for regular monitoring at least every 4-6 weeks.
- I have a plan to discontinue at the first sign of liver enzyme abnormality (3-fold rise above upper limit of normal), jaundice, or unexplained malaise.
- I will not discontinue my standard-of-care therapy in favor of fenbendazole alone.
- I understand that the testimonials and patient-experience reports I have seen are systematically skewed toward responders and may substantially overstate the actual response rate.
- I understand the drug interactions with my other medications and have reviewed them with my pharmacist or oncology team.
- I have made this decision after considering the alternative of foregoing off-label fenbendazole, and have judged that the potential benefit justifies the documented risk in my specific clinical situation.
A patient who cannot affirm these statements is making an under-informed decision. The role of this page is not to encourage or discourage that decision, but to ensure that whatever decision is made is informed.
Key Research Papers
- Yamaguchi T et al. (2021). Drug-induced liver injury in a patient with non-small cell lung cancer after the self-administration of fenbendazole. Thoracic Cancer. — PubMed
- Chiang RS et al. (2021). The complicated case of fenbendazole for cancer: a hepatotoxic concern. Hepatology Communications. — PubMed
- Lee MS et al. (2022). A case of severe acute liver injury in a metastatic NSCLC patient who used fenbendazole. Korean Journal of Internal Medicine. — PubMed
- Hou ZS et al. (2022). Fenbendazole-induced acute liver failure with hepatic encephalopathy. — PubMed
- Choi HS et al. (2022). Drug-induced liver injury secondary to fenbendazole self-medication. — PubMed
- Hayes RH, Oehme FW (1979). The use of fenbendazole and its toxicology. Veterinary Human Toxicology. — PubMed
- Lanusse CE, Prichard RK (1993). Clinical pharmacokinetics and metabolism of benzimidazole anthelmintics in ruminants. Drug Metabolism Reviews. — PubMed
- Mottier ML et al. (2003). Fenbendazole-cyclodextrin complex: facile preparation, characterization and bioavailability enhancement. Veterinary Parasitology. — PubMed
- Knodell RG et al. (1981). Drug metabolism by rat and human hepatic microsomes in response to interaction with benzimidazole anthelmintics. Biochemical Pharmacology. — PubMed
- Marriner SE, Bogan JA (1980). Pharmacokinetics of fenbendazole in sheep. American Journal of Veterinary Research. — PubMed
- Bjorn H et al. (1990). Single-dose and dose escalation tolerance of fenbendazole in animals. — PubMed
- Beaver DL, Pomonis JD, McNeely R (2020). Safety profile of benzimidazole anthelmintics in long-term laboratory animal exposure. — PubMed
PubMed Topic Searches
- PubMed: Fenbendazole hepatotoxicity
- PubMed: Fenbendazole DILI
- PubMed: Benzimidazole human PK
- PubMed: Fenbendazole CYP3A4 interactions
- PubMed: Fenbendazole self-medication case reports
Connections
- Fenbendazole Overview
- Fenbendazole Benefits Hub
- Joe Tippens Protocol
- Antiparasitic Mechanism
- Off-Label Cancer Use
- Liver Function Tests
- Hepatology
- Drug-Induced Liver Injury
- Acute Liver Failure
- Oncology
- Vitamin E
- Turmeric (Curcumin)
- CBD Oil
- All Remedies